0525
T2 Mapping of the Prostate at 7 Tesla: A Feasibility Study1Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Bern, Switzerland, Bern, Switzerland, 2Magnetic Resonance Methodology, Institute of Diagnostic and Interventional Neuroradiology, University of Bern, Bern, Switzerland, Bern, Switzerland, 3Translational Imaging Center (TIC), Swiss Institute for Translational and Entrepreneurial Medicine, Bern, Switzerland, Bern, Switzerland, 4Dept. of Diagnostic, Interventional and Pediatric Radiology, Inselspital, Bern University Hospital, Switzerland, Bern, Switzerland, 5Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, Berlin, Germany, 6Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany, Heidelberg, Germany, 7Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, Minneapolis, MN, United States, 8Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, Lausanne, Switzerland, 9Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, Lausanne, Switzerland, 10LTS5, École Polytechnique Fédérale de Lausanne, Lausanne, Switzerland, Lausanne, Switzerland
Synopsis
Keywords: High-Field MRI, Prostate
Motivation: T2 relaxometry has shown potential to distinguish cancer from prostate tissue at 3T. Despite potential gains in resolution, it has been little explored at ultra-high field due to challenging B1+ homogeneity and efficiency.
Goal(s): To investigate feasibility of prostate T2 mapping at 7T using a robust RF shimming procedure.
Approach: We evaluated conventional 2D multi-echo spin echo and an optimized 3D T2-prepared segmented-FLASH sequence.
Results: Spin-echo T2 maps showed good quality but required long acquisition times for limited coverage. The T2-prepared FLASH sequence showed similar values while providing higher scan efficiency, lower SAR, and whole-organ coverage at the cost of higher motion sensitivity.
Impact: Quantitative T2 mapping at ultra-high field is challenging due to acquisition time and SAR restrictions, especially in the pelvic area. The methods investigated here may be used in future routine to detect and grade prostate cancer.
INTRODUCTION
Quantitative MRI biomarkers such as the apparent diffusion coefficient have shown to be a valuable tool to detect prostate cancer. Similarly, T2relaxometry has shown potential to distinguish between prostate cancer and healthy tissue at 3T [1]. At ultra-high field (UHF), T2mapping has been little explored, mainly in advance centers [2], potentially due to limited B1+ homogeneity and efficiency at the location of the prostate. However, UHF imaging becomes more accessible for clinical exams because the use of parallel transmission (pTx) has become more streamlined and especially more robust while abdominal/pelvic RF coils more available.We investigated the use of multi-echo spin echo (MESE) and fast T2-prepared 3D FLASH sequences in combination with an established static pTx (RF shimming) procedure for T2mapping in the prostate. MESE is robust but requires long acquisition times (TA) and is limited to 2D imaging due to high SAR for the application of multiple refocusing pulses. Alternatively, T2-prepared (T2p) approaches [3] combined with fast gradient echo sequences [4] are more SAR efficient and allow for larger volumetric coverage. Here we report preliminary in vivo tests in our research setting.
METHODS
IRB-approved experiments were performed at 7T (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) using an 8-channel Tx/32-channel Rx body array coil (Tesla Dynamic Coils, Zaltbommel, The Netherlands). Three healthy male subjects (range 33-68 yo.) were scanned in feet-first supine position without special preparation for pelvis imaging.After localization, 2D FLASH-based multi-transmit relative B1+ maps [5] were acquired on a selected transversal slice at the center of the gland. RF phase shim values were optimized offline by increasing the transmit efficiency [6] in a manually drawn ROI including the prostate and were used for all subsequent imaging. For anatomical reference, a turbo spin echo sequence (TSE) was also acquired (Table 1).
A two-dimensional single-slice MESE sequence was acquired with ten TEs (Table 1) in 13:02 min.
For T2-prepared imaging, a segmented 3D-FLASH research application sequence [7] employing a variable-density Cartesian undersampling pattern [8] was acquired. After adiabatic T2 preparation [9], readouts of the FLASH block followed with a center-out trajectory (Figure 1). Three volumes were acquired consecutively with TEp=26, 60, and 90 ms. The tested protocol parameters (Table 1) resulted in TA=3:21 min/volume for a total scan time of 10:01 min. Images were reconstructed on the scanner with compressed sensing [10].
Single-compartment T2maps were generated offline using a log-linear voxel-wise fit of $$$M_{TE(p)}=M_0e^{-(TEp/T_2)}$$$. For T2p-FLASH, volumes were aligned prior to fitting with rigid followed by non-rigid registration [11] using an ROI of the entire prostate. For MESE, the first echo was removed prior to fitting to mitigate stimulated echo effects.
Average T2 values were computed in manually drawn ROIs of the peripheral (PZ) and transitional (TZ) zones on the selected central slice for both methods.
All offline calculations and analyses were performed in MATLAB (MathWorks, Natick, Massachusetts).
RESULTS AND DISCUSSION
The SAR for one T2p-FLASH acquisition was slightly lower than for MESE in all subjects (Table 2A) although whole-prostate coverage is achieved instead of a single slice.TSE and MESE showed very good image quality at the level of the prostate and good contrast between PZ and TZ in all subjects (Figure 2A-B). The volumetric T2p-FLASH acquisition was more affected by pelvic motion artifacts, albeit good T2contrast was observed through different TEp images (Figure 2).
MESE T2 maps showed a homogenous T2 distribution and good depiction of the anatomy. T2p-FLASH maps showed similar quality in two out of the three subjects. In the third subject, the voxel-wise fitting was not successful in the lower portion of the gland (Figure 3, arrow) due to motion within FLASH acquisitions. The zonal T2 analysis showed a trend for higher values in PZ (range: 62-73 ms) than in TZ (range: 65-102 ms), increasing T2 values as a function of the subjects’ age, and good agreement between MESE and T2p-FLASH measurements (Table 2B).
CONCLUSION
For the first time, to the best of our knowledge, we have shown the feasibility of prostate T2 mapping at 7T with a commercial Rx/Tx abdominal array coil and dedicated RF shimming procedures in a clinical research setting. In comparison to a single slice MESE, the accelerated volumetric T2p-FLASH tested here was more sensitive to motion due to the repeated 3D scans but could offer whole-prostate mapping with the same resolution and 3-minute faster acquisition time. While further investigation is warranted to shorten the acquisition, improve its motion robustness and establish comparison with lower fields, T2-prepared sequences may be a more time- and SAR-efficient alternative to spin echo-based methods for quantitative pelvic UHF MRI.Acknowledgements
No acknowledgement found.References
- Mai, Julia; Abubrig, Mohamed MD; Lehmann, Thomas PhD; Hilbert, Tom PhD; Weiland, Elisabeth PhD; Grimm, Marc O. MD; Teichgräber, Ulf MD; Franiel, Tobias MD. T2 Mapping in Prostate Cancer. Investigative Radiology 54(3):p 146-152, March 2019. | DOI: 10.1097/RLI.0000000000000520
- Hu, X. et al. First in-vivo human imaging at 10.5T: Imaging the body at 447 MHz. Magn Reson Med. 2020;84:289–303.
- Brittain JH, Hu BS, Wright GA, Meyer CH, Macovski A, Nishimura DG. Coronary angiography with magnetization-prepared T2 contrast. Magn Reson Med 1995;33(5):689-696.
- Haase A, Frahm J, Matthaei D, Hänicke W, Merboldt K‐D. FLASH imaging: rapid NMR imaging using low flip angle pulses. J Magn Reson 1986; 67: 258–266.
- P-F. Van de Moortele, and K. Ugurbil. Very Fast Multi Channel B1 Calibration at High Field in the Small Flip Angle Regime. Proc. Intl. Soc. Mag. Reson. Med. 17 (2009). P367.
- Schmitter, S. et al. Cerebral TOF angiography at 7T: Impact of B1 (+) shimming with a 16-channel transceiver array. Magn Reson Med 71, 966–977 (2013).
- Bonanno G, et al. (2021) High-resolution T2 maps of the whole brain at 7 Tesla: a proof-of-concept study using adiabatic T2-prepared FLASH and compressed sensing. Proc. Of Intl. Soc. Mag. Reson. Med. (Vol. 30) P3047.
- Forman C, et al. High-resolution 3D whole-heart coronary MRA: a study on the combination of data acquisition in multiple breath-holds and 1D residual respiratory motion compensation. Magn Reson Mater Phy 2014;27:435-443.
- Nezafat R at al., Spectrally Selective B1-Insensitive T2 MagnetizationPreparation Sequence Magnetic Resonance in Medicine 61:1326–1335 (2009).
- Wetzl J, Forman C, Wintersperger BJ, et al. High‐resolution dynamic CE‐MRA of the thorax enabled by iterative TWIST reconstruction. Magn Reson Med. 2017;77:833–840.
- S. Klein, M. Staring, K. Murphy, M.A. Viergever, J.P.W. Pluim, "elastix: a toolbox for intensity based medical image registration," IEEE Transactions on Medical Imaging (2010), vol. 29, no. 1, pp. 196 - 205.
Figures
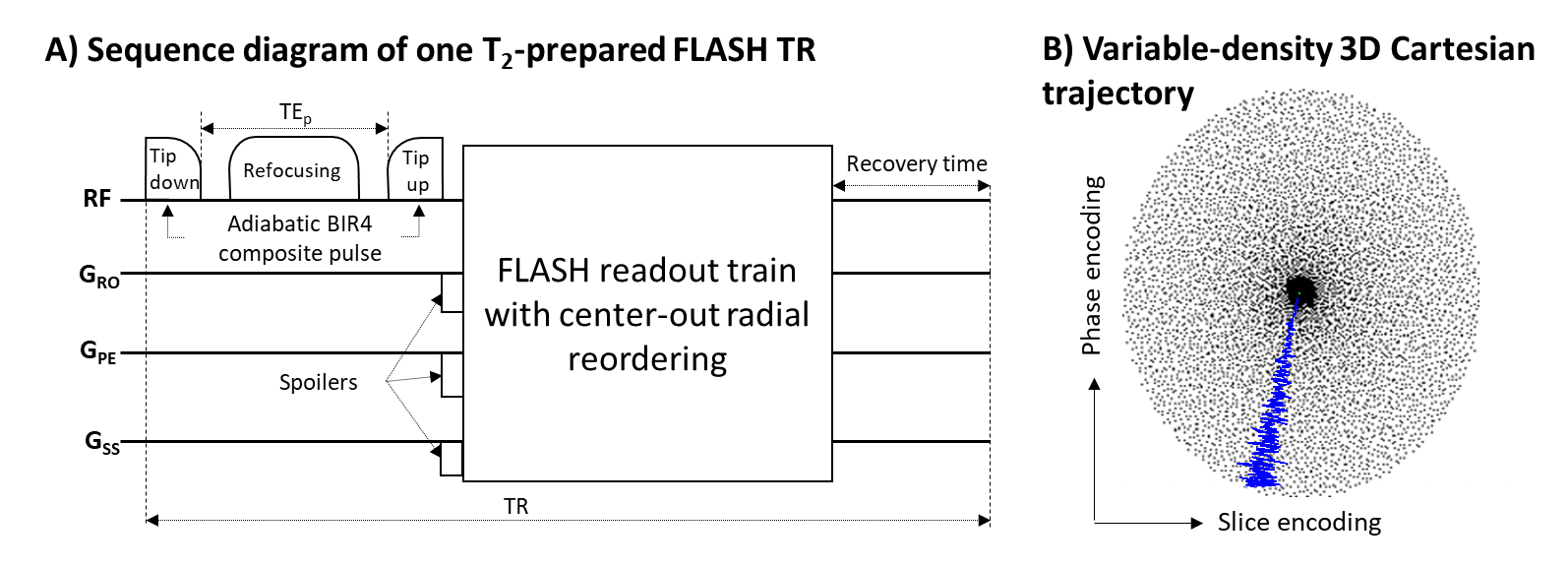
Figure 1. A) One repetition of the proposed segmented T2-prepared segmented FLASH sequence. The adiabatic T2p uses a BIR4 composite pulse with delays between the pulse segments (tip-down/up: 10-ms duration, refocusing: 20-ms duration). The voltage of the BIR4 pulse was chosen empirically of ca. 87 V to stay below the SAR inline tracing limit for each segment (system reference amplitude=300 V). B) Cartesian spiral-phyllotaxis undersampling pattern. Black dots indicate sampled readout lines. The blue line shows an example of the center-out k-space trajectory in one TR.
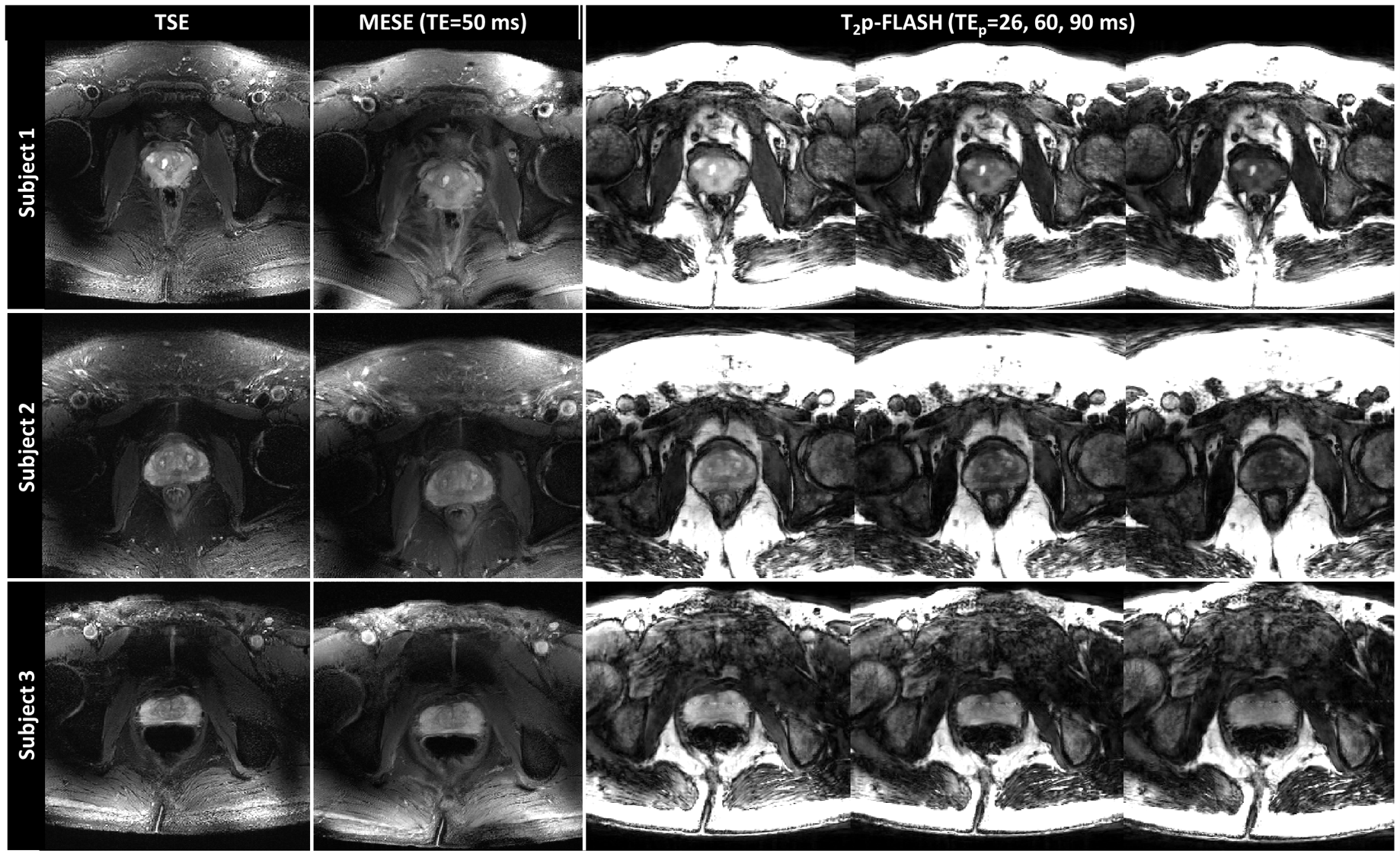
Figure 2. Morphological turbo spin echo (TSE), multi-echo spin echo (MESE) for TE=50 ms, and 3D T2p-FLASH images are shown on the selected central slice of the prostate that was used for RF shimming. TSE shows best contrast and anatomical details. MESE shows similar good depiction of the anatomy and T2 contrast. Central slice of the T2p-FLASH volumes shows good T2-weighted contrast at different TEp and more motion artifacts due to the volumetric acquisition. T2p-FLASH images of subject 3 also show an artifact going through the prostate probably due to RF interference.
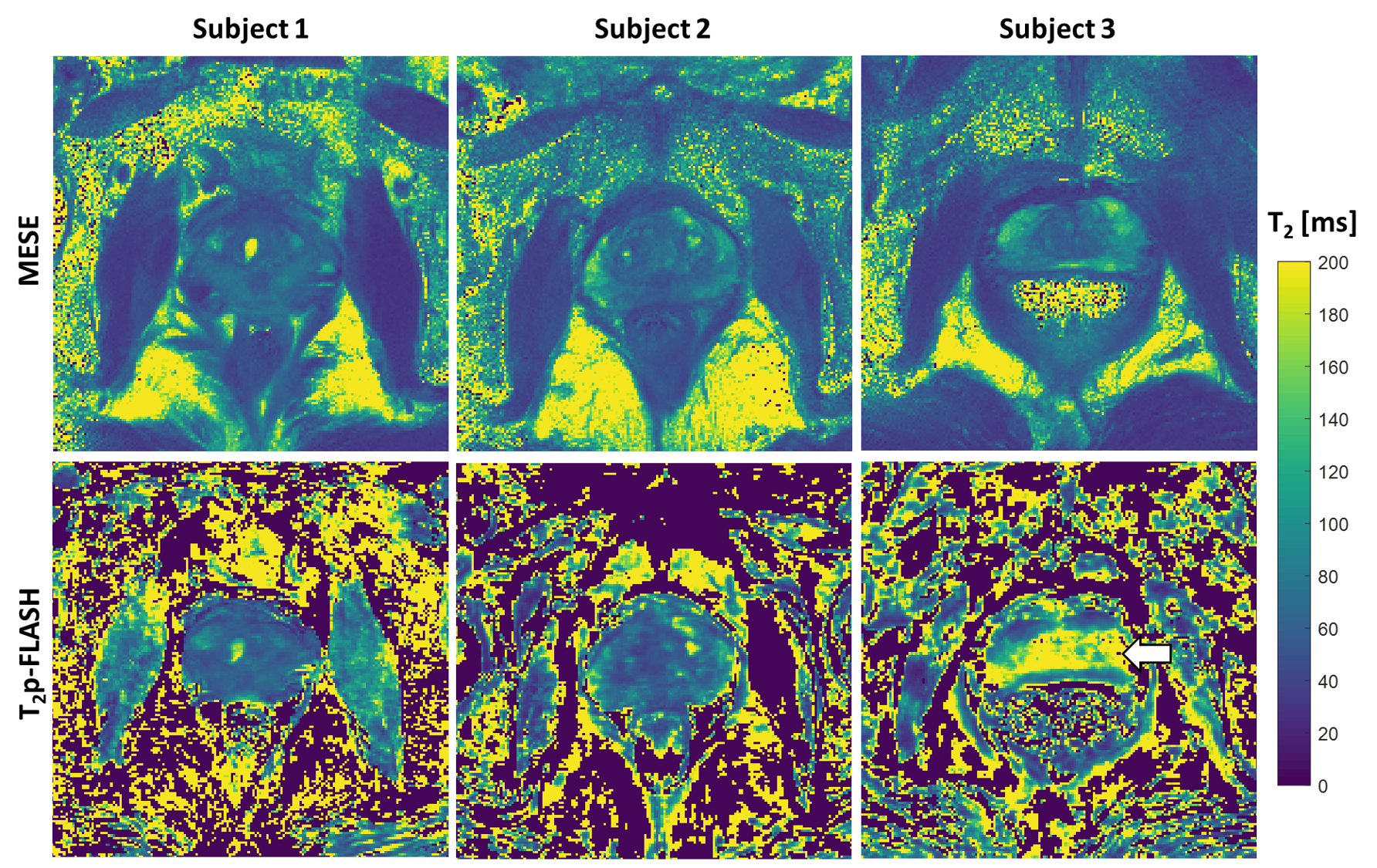
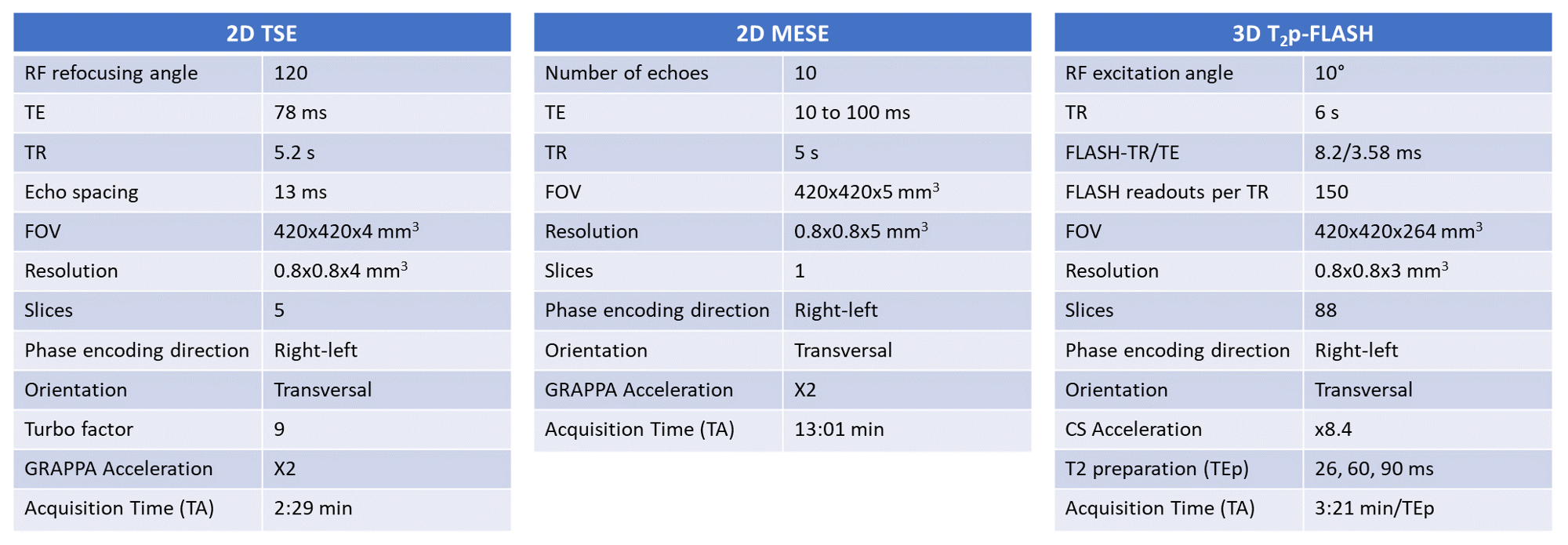
Table 1. Parameters of the sequences employed in the study: a morphological two-dimensional (2D) turbo spin echo (TSE), 2D multi-echo spin echo (MESE) and three dimensional T2-prepared (T2p) FLASH sequence for T2 quantification.
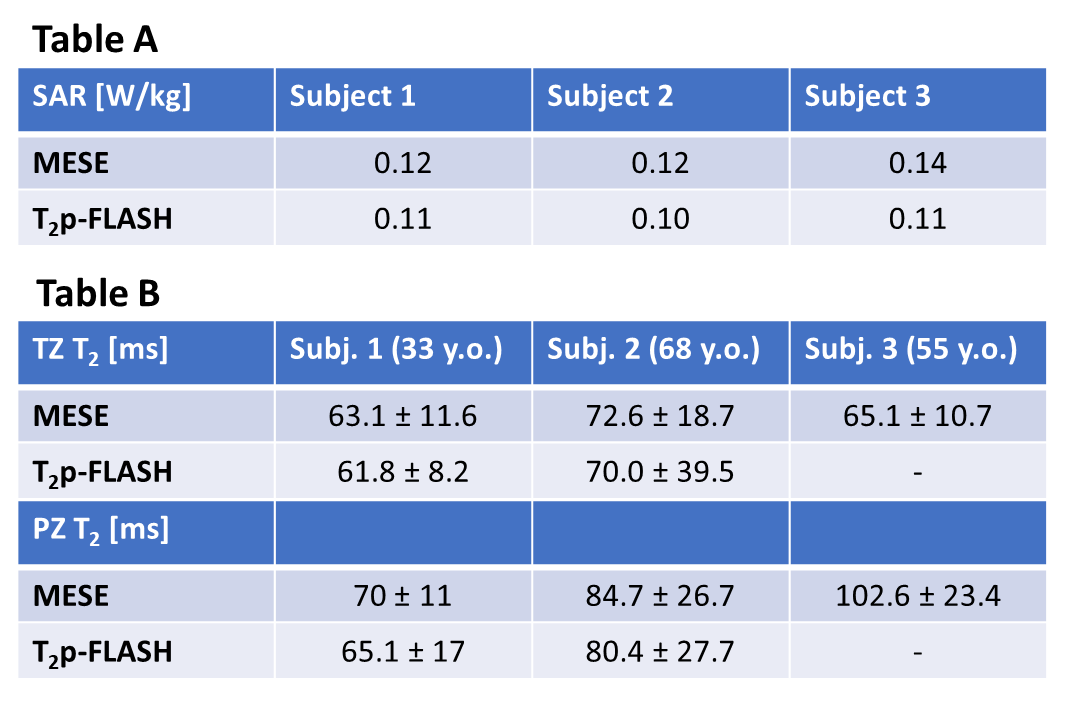
Table 2. A) Specific absorption rate (SAR) values for MESE and T2p-FLASH acquisitions. B) Quantitative T2 values (mean ± standard deviation) from manually drawn ROIs of the transitional (TZ) and peripheral (PZ) zones on the central selected slice (shown in Figure 3) for MESE and T2p-FLASH sequences are reported for all subjects. T2p-FLASH values agree well with MESE. Subjects 3 was not analyzed because failure of fitting in parts of the prostate, due to misregistration.