0522
Quantitative Abdominal Sodium MRI Combined with 32-Channel Proton pTx MRI at 7T in a Large Field-of-View1Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany, 2Faculty of Physics and Astronomy, Heidelberg University, Heidelberg, Germany, 3University Hospital Erlangen, Institute of Radiology, Friedrich‐Alexander‐Universität Erlangen‐Nürnberg (FAU), Erlangen, Germany, 4Faculty of Medicine, Heidelberg University, Heidelberg, Germany
Synopsis
Keywords: High-Field MRI, Quantitative Imaging, 23Na, Sodium, parallel transmit (pTx), TIAMO, tissue sodium concentration (TSC), 7T whole-body coils, Body, Data Acquisition, High-Field MRI, Hybrid & Novel Systems Technology, Kidney, Liver, Multi-Contrast, Non-Proton, Whole Body
Motivation: 23Na MRI enables the quantification of the tissue sodium concentration. A large field-of-view is beneficial for abdominal MRI, especially if several organs are of interest. Due to lower resolution compared to 1H MRI, 23Na MRI is less suited for segmentation.
Goal(s): To combine large field-of-view 1H and quantitative abdominal 23Na MRI in the same position at 7T.
Approach: Employing a custom-built 23Na radiofrequency coil and reference vial setup together with a 32-channel proton pTx array to allow dual-nuclei MRI in the same position.
Results: Combination of large field-of-view 1H and quantitative 23Na MRI of the human torso is feasible at 7T in ≤42min.
Impact: This work shows the feasibility of combined 1H and 23Na imaging at 7T in a large field-of-view both under free breathing, laying the ground work for an accurate evaluation of the tissue sodium concentration in several organs at once.
Introduction
The challenges of sodium MRI in the human torso are the relatively low in-vivo concentrations, very short transversal relaxation times and the low NMR sensitivity of the 23Na nucleus compared with 1H, resulting in a low signal-to-noise ratio and rather poor spatial resolutions. As this makes an accurate segmentation of different organs in 23Na images difficult, 1H images acquired in the same position or registered onto the 23Na data in post processing are advantageous. Furthermore, a large field-of-view is beneficial for abdominal MRI, especially if several organs are of interest.In this work, quantitative 23Na images as well as 1H pTx images of the human abdomen were acquired at 7T in the same position for two healthy volunteers under free breathing to show the feasibility of a large field-of-view combination of these two contrast modalities.
Methods
The measurements were performed in two healthy volunteers (one female/one male, age 34/43 years, weight 85/67kg) measured head-first supine with raised arms and their hands placed above the head. For the concentration determination, four external reference vials with NaCl solutions (20mM, 60mM, 100mM, 140mM) were positioned under the volunteer’s back at fixed positions in a compartment filled with 35mM NaCl solution and 2% agarose. All measurements were performed on a 7T whole-body MR system1 with a custom-built oval-shaped radiofrequency body coil2 for the 23Na measurements and a 32-channel pTx body coil3, placed behind the scanner bore for the 1H images.Density-adapted 3D radial sampling4 (DA-3DPR) with a golden angle projection distribution5 was applied for both 23Na and 1H MRI. For the 1H images, TIAMO6 was utilized by applying two modes that were optimized for a torso-simulating phantom. All images were reconstructed with a NUFFT7.
A 3D 1H GRE sequence with radial phase encoded (RPE) acquisition8 (GRE-RPE) was applied to investigate the possibility to further shorten the total measurement time. Here, a CP+ shim was applied and images were reconstructed using iterative SENSE9.
All sequences were acquired in free breathing. Acquisition parameters and reconstruction settings can be found in Tab. 1.
23Na T1 relaxation effects in the reference vials were corrected according to the FLASH equation. To correct for B1 inhomogeneities, transmit and receive field maps of the 23Na radiofrequency coil were simulated2,10 in human voxel models11,12 (Ella, scaled by 5% to better fit the female’s anatomy, as well as Duke for the male volunteer) using the electromagnetic field simulation software CST13. T1, B1+ and B1- corrections were previously validated for the applied setup in phantom measurements10,14 and showed improved TSC accuracy. Quantitative 23Na images were calculated with a semi-automated segmentation tool self-developed in Matlab15 using the known concentration in the reference vials and interpolation based on a linear fit.
Results
3D 1H images and corresponding quantitative TSC maps acquired with DA-3DPR for the two volunteers as well as an overlay of both are shown in Fig. 1 (total acquisition time: 41 min 40 s). Utilizing the GRE-RPE sequence, the total acquisition time of the scan session could be further reduced to approximately 30 min. Resulting images are shown in Fig. 2 and compared to the DA-3DPR in Fig. 3. Fig. 4 shows an animation of several coronal slices of 1H and quantitative 23Na MRI in volunteer one.Discussion & Conclusion
Acquisition of both 1H and 23Na data with the same sequence (DA-3DPR) under free breathing, as well as reconstruction with the same resolution of (2.5mm)³ allows for a simple overlay of the two 3D datasets. The reference vial setup caused some artefacts in the undersampled 1H DA-3DPR images (≈4-fold undersampling), which might be less pronounced for a smaller undersampling factor. The image quality is nevertheless sufficient for segmentation of different organs such as the kidneys or liver.As no 1H B1+ maps were acquired in this study, transmit fields could not be optimized for each volunteer and the CP+ mode and a TIAMO shim optimized for a phantom were used, which resulted in residual 7T-related 1H signal dropouts (Fig. 1-2). Subject-specific optimization of the TIAMO shims could minimize this problem and would be valuable to implement in the future.
Higher contrast was observed for the GRE-RPE compared to the DA-3DPR image, which may be caused by the higher flip angle and shorter TR.
As the data are acquired in free breathing, respiratory motion blurs the reconstructed images. In the future, it could be investigated how respiratory sorting improves the segmentation and TSC determination in this setup.
Segmentation of different organs will be performed as a next step to compare the TSC in different target organs with previously published data.
Acknowledgements
No acknowledgement found.References
1. MAGNETOM 7T, Siemens Healthcare GmbH, Erlangen, Germany2. T. Platt et al. Magn. Reson. Med. (2018). https://doi.org/10.1002/mrm.27103
3. S. Orzada et al. Plos One (2019). https://doi.org/10.1371/journal.pone.0222452
4. A. M. Nagel et al. Magn. Reson. Med. (2009). https://doi.org/10.1002/mrm.22157
5. R. W. Chan et al. Magn. Reson. Med. (2009). https://doi.org/10.1002/mrm.21837
6. S. Orzada et al. Magn. Reson. Med. (2010). https://doi.org/10.1002/mrm.22527
7. J. A. Fessler et al. IEEE Trans. Signal Process. (2003). https://doi.org/10.1109/TSP.2002.807005
8. S. Dietrich et al. Magn. Reson. Med. (2020). https://doi.org/10.1002/mrm.28602
9. G. Cruz G et al. Magn. Reson. Med. (2016). https://doi.org/10.1002%2Fmrm.25708
10. A. K. Scheipers et al. ISMRM Workshop on Ultra-High Field MR (2022). Poster: 64.
11. A. Christ et al. Phys. Med. Biol. (2010). https://doi.org/10.1088/0031-9155/55/2/N01
12. S. Gabriel et al. Phys. Med. Biol. (1996). https://doi.org/10.1002/10.1088/0031-9155/41/11/002
13. CST Studio Suite 2019/2020 (Dassault Systèmes, Vélizy-Villacoublay, France)
14. A. K. Scheipers et al. Proc. Intl. Soc. Mag. Reson. Med. 30 (2021). Abstract: 0238.
15. The MathWorks Inc., Natick, MA, USA
Figures
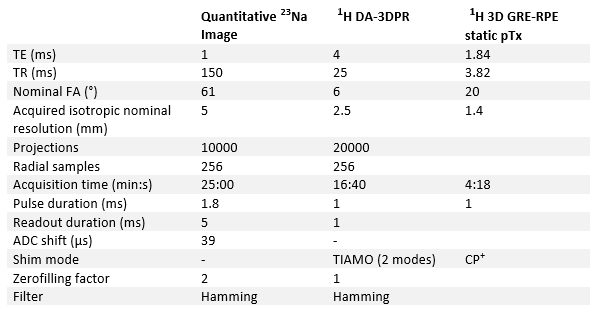
Tab. 1: Acquisition parameters and reconstruction settings for the different sequences
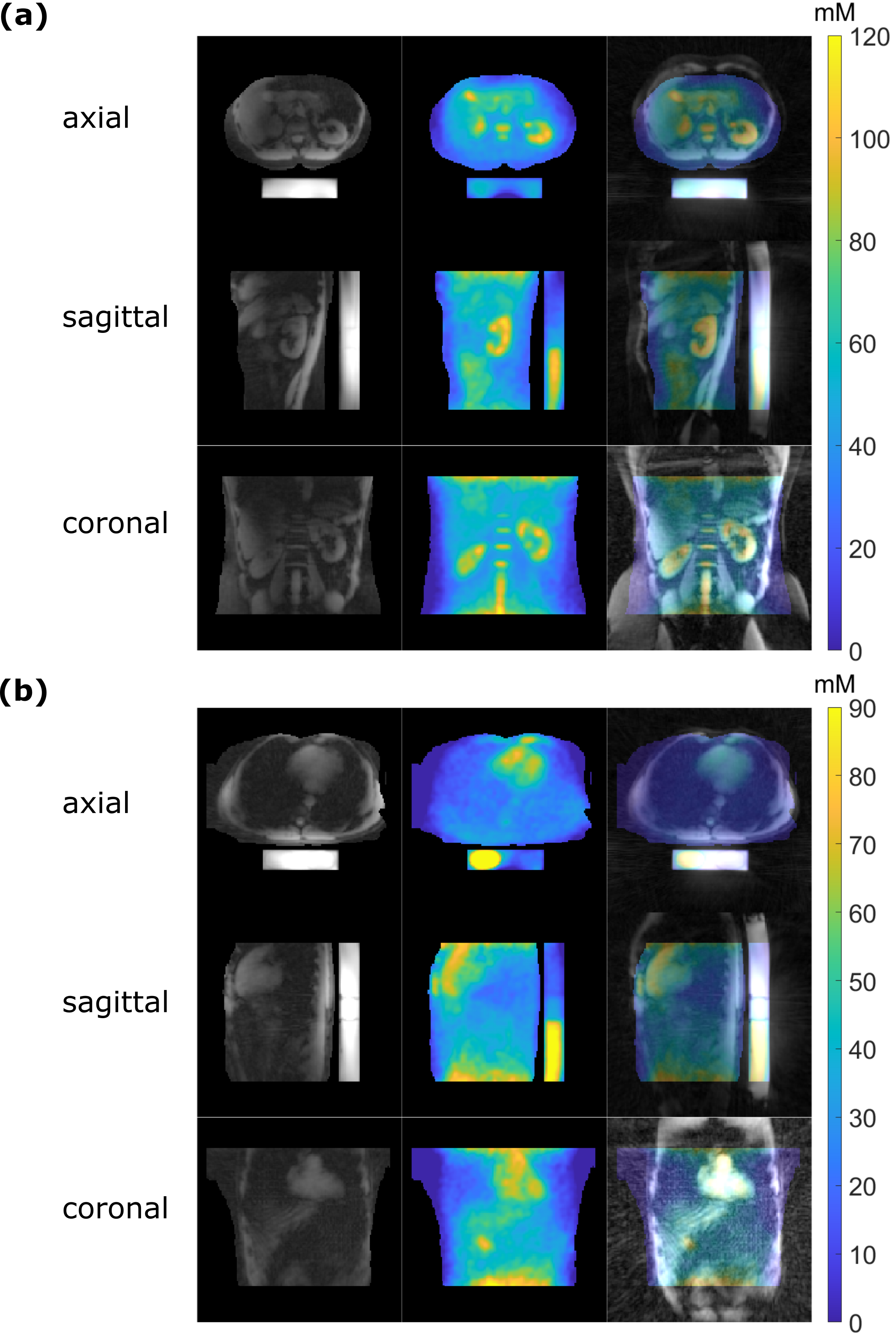
Fig. 1: 1H DA-3DPR image, quantitative 23Na image and overlay for volunteer one (a) with the kidneys visible and for volunteer two (b) with the heart visible. The reference vial setup under the volunteer’s back was used for the concentration determination. 7T-related 1H signal dropouts can be observed in e.g. the liver of volunteer one.
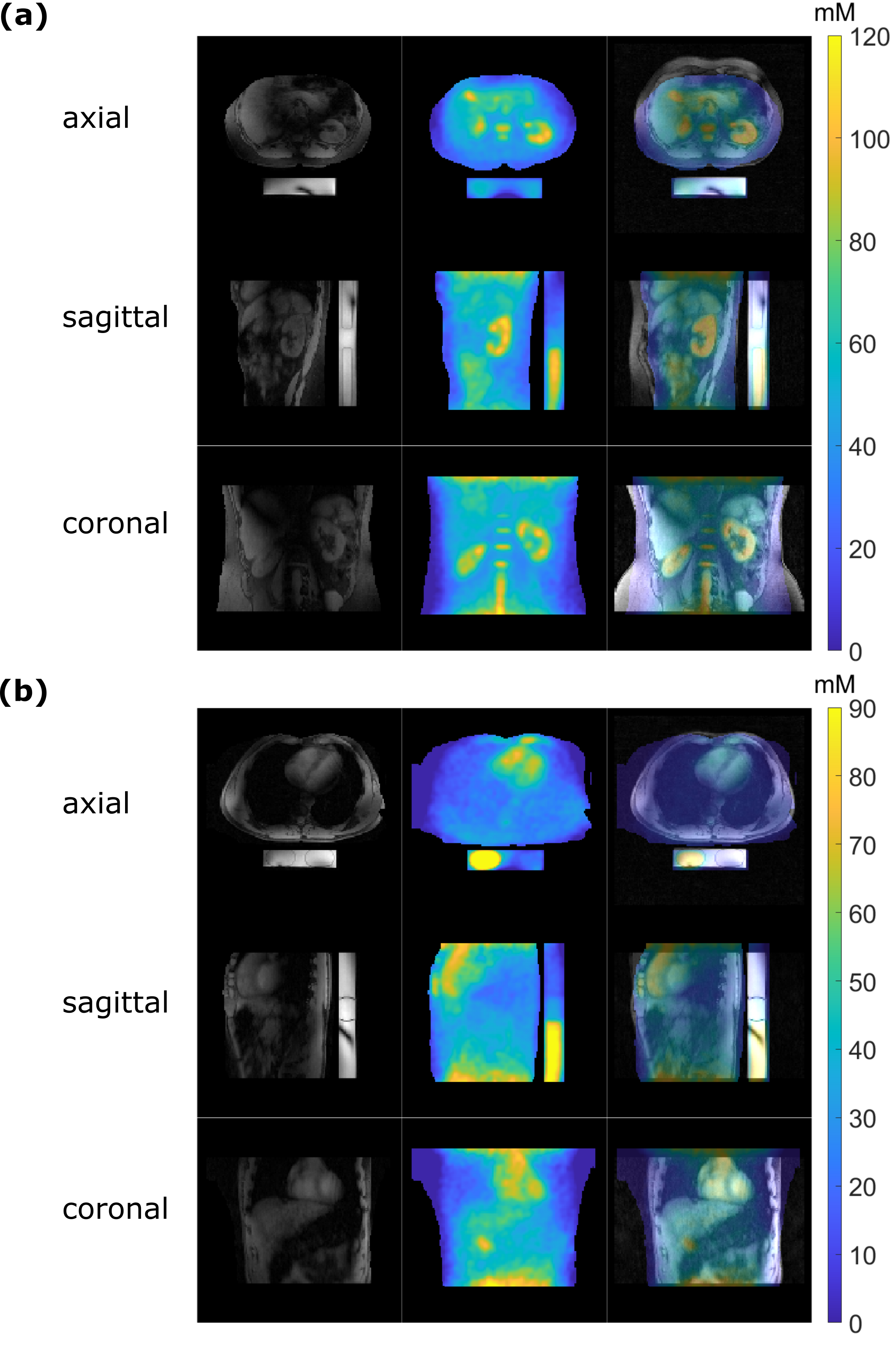
Fig. 2: 1H 3D GRE-RPE static pTx images, quantitative 23Na image and overlay for volunteer one (a) with the kidneys visible and for volunteer two (b) with the heart visible. The contrast within, for example, the kidneys of volunteer one is superior to the undersampled DA-3DPR image in Fig. 1, but there are still some ultrahigh-field-related 1H signal dropouts as can be seen in the liver of volunteer one.

Fig. 3: 1H DA-3DPR and 3D GRE-RPE static pTx images for volunteer one with the kidneys visible. The contrast within the kidneys of volunteer one in the 3D GRE-RPE is superior to the DA-3DPR image, potentially due to the higher flip angle and shorter TR. Ultrahigh-field-related 1H signal dropouts for example in the liver are more pronounced in the 3D GRE-RPE image (CP+) compared to the DA-3DPR image (TIAMO). DA-3DPR images cover a larger field-of-view but also show some artifacts arising from the reference vial setup, which might be less pronounced for a smaller undersampling factor.
Fig. 4: Animated illustration of the 1H DA-3DPR image and quantitative 23Na image of volunteer one showing every third slice in a subset of 14cm.