0516
Fine-Tuning Deep Learning Model For Quantitative Knee Joint Mapping with MR Fingerprinting1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States
Synopsis
Keywords: Cartilage, MR Fingerprinting, Knee cartilage, Deep learning
Motivation: Estimating MRF quantitative parameters with neural networks (NNs) is faster than dictionary-matching methods (DMs), and it has the advantage of providing continuously distributed parameters.
Goal(s): We investigate different aspects of NN training and evaluate its quantitative MRF performance and compare them with DMs.
Approach: We exploit how training data sizes, noise levels, and SVD compression sizes affect the MRF performance of the NNs and compare them with DMs.
Results: The NN provides a faster way of multi-parametric mapping from NIST/ISMRM phantom and knee joint MRF data sets with comparable performance to DMs.
Impact: Well-tuned NN is much more efficient for quantitative MRF, particularly for the knee joint. Besides computational speed, fine-tuning can also increase the performance and robustness to noise.
Introduction
MR fingerprinting (MRF) probes multiple quantitative MRI parameters simultaneously exploiting the dynamics of MR signals1. MRF also exploits undersampling, which reduces the overall MRI examination time.Dictionary matching methods (DMs) are the most common approach for estimating quantitative parameters from MRF data1. However, it is susceptible to discretization errors depending on the dictionary size. Improving this means increasing memory and computation time due to the large size of the dictionary2,3. In recent years, neural networks (NNs), particularly deep learning (DL), have been proposed to speed up the fitting and address the dimension-related difficulties of DMs2,3,4,5.
While potentially better than DMs, NNs requires proper tuning, with adequate choices of training parameters, such as the training data size, added noise type and level, and number of components in the SVD compression. We hope to address these questions in this study, investigating the effects of these choices for NNs designed to estimate T1, T2, and T1ρ from MRF. The results are compared to those from DMs on a model NIST/ISMRM phantom and knee cartilage from healthy subjects.
Methods
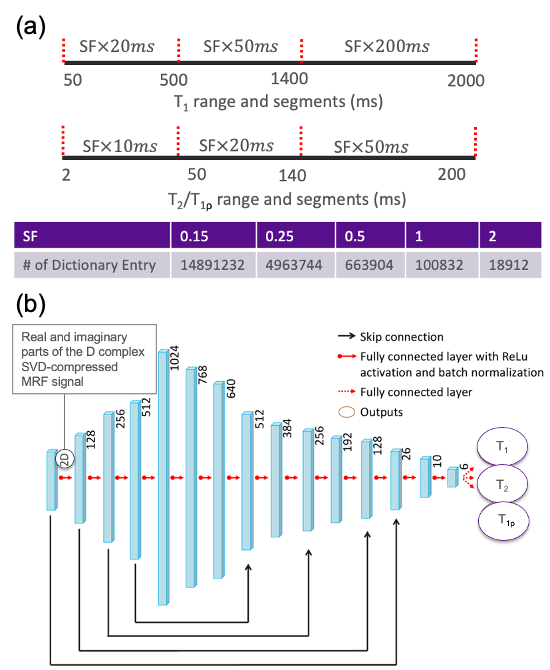
Data acquisition: We scanned 14 healthy subjects (35.4±9.3 years, age range 19-62 years; eight males, after getting informed consent) and a NIST/ISMRM phantom on a 3T scanner6, using a recently developed 3D-MRF sequence for simultaneous T1, T2, and T1ρ mapping7.Data processing: Dictionaries of simulated MR fingerprints based on extended phase graphs were created with a T1 range of 50-2000 ms, T2//T1ρ range of 2-200 ms with different step sizes, and flip angle ranges of 30° to 90° with steps of 15° increments8.
Figure 1 shows the details of the dictionaries used in this study. The measured MR fingerprints and the simulated dictionary were normalized and compressed using SVD to speed up the DMs and NNs3,5.A fully-connected voxel-wise network from Ref.3 was used in this study. Various models were trained: different training data sizes, different learning rates (LR), adding different noise levels, and different SVD dimensions. The noise level is defined as the standard deviation (SD) of a zero-mean Gaussian distribution. Comparisons were conducted on the MRF parametric maps between NNs and DMs.
For the in-vivo knee dataset, five regions of interest (ROIs) were manually drawn: the lateral femur, lateral tibia, medial femur, medial tibia, and patella cartilages. For each subject, the mean and SD for T1, T2, and T1ρ were measured on each ROI of the knee. All MRF parameter comparisons were conducted in those ROIs.
Evaluation metrics: Mean, SD, mean relative absolute error (MRAE) and mean of the normalized absolute error (MNAE).
Results
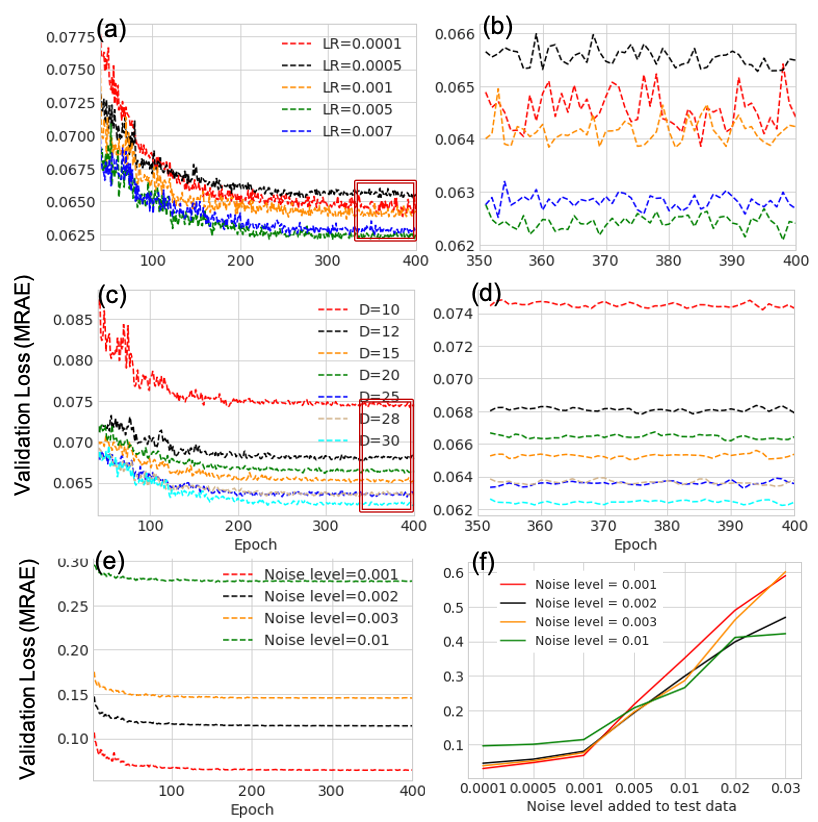
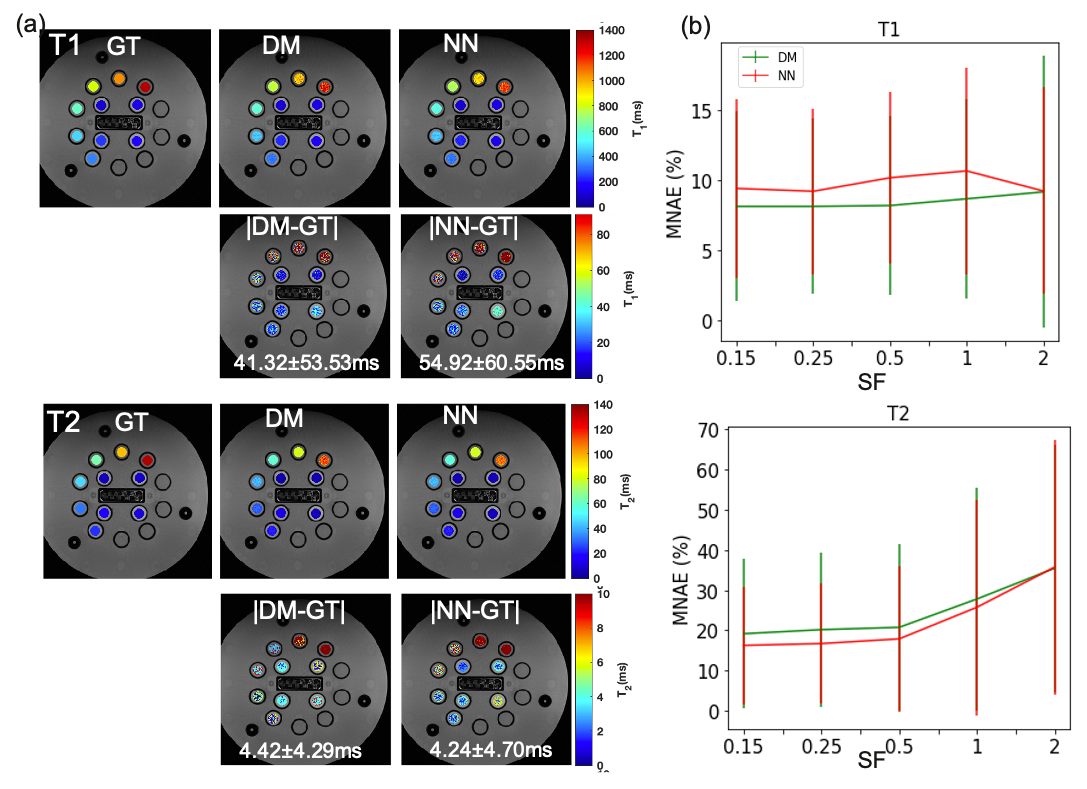
Figure 2 shows the validation loss (MRAE) for LR, noise level, and SVD dimension in the training stage for the NNs using a dictionary with sampling factor (SF)=0.15. As shown in the figure, those aspects affect the convergence value for the training, especially for the noise level. In the fitting of the in-vivo data, we chose LR=0.005, SVD dimension=30, and noise level=0.002 (best overall performance in all added noise level on test data shown in (f)).Figure 3 displays the MNAE of measurements from DMs and NNs for different dictionary sizes on the NIST/ISMRM phantom. The reference values of T1 and T2 in the phantom profile were used as ground truth. This MNAE shows that the dictionary size affects the measurement of T2 more than T1 for both methods. The error of NNs is comparable to DMs on T1 and is lower on T2. For DMs, ideally, the smaller the SF, the smaller the error. However, as shown in Figure 1, the size of the dictionary will increase numerously, therefore, as a compromise we chose SF=0.5 for the DMs for the in-vivo data.
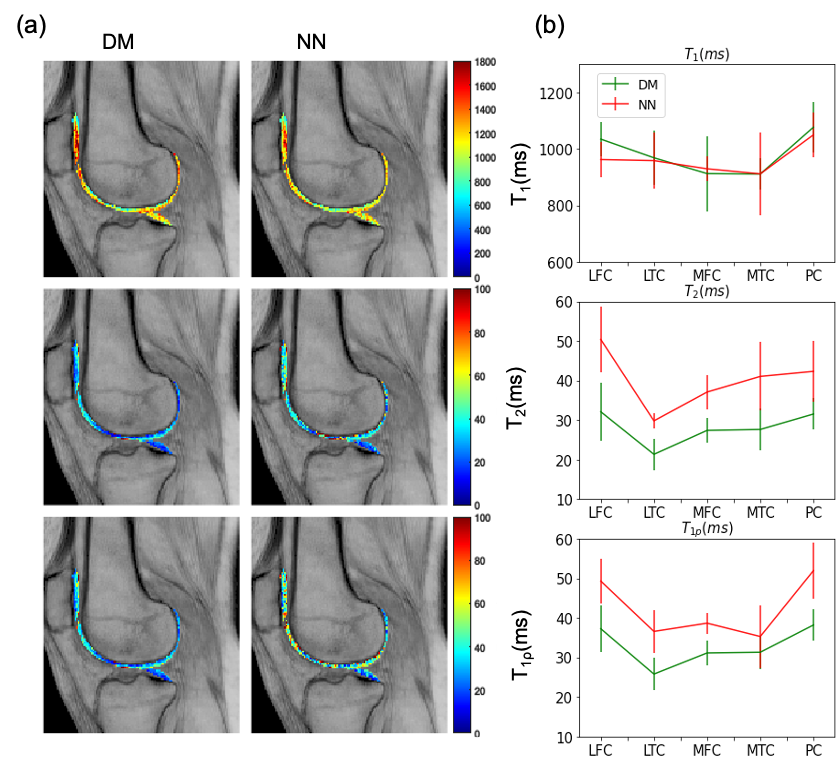
Figure 4 shows measurements of T1, T2, and T1ρ using DMs and NNs for in-vivo knee joint. For all ROIs, T1 has a comparable estimate from NN compared to DM while showing a higher value for T2 and T1ρ, and this discrepancy is consistent with the error values in the NIST/ISMRM phantom as shown in Figure 3.
One slice with dimension 161×161, NNs takes 0.45 seconds while DMs (SF=0.5) takes 42 seconds to compute T1, T2, and T1ρ maps on the same hardware.
Discussion and Conclusion:
NNs is a faster approach for multi-parametric mapping from MRF data with accuracy comparable to DMs. With NNs, hyperparameters and training settings should be carefully tuned. Future work includes the investigation of different networks, loss functions, and different MRF sequences.Acknowledgements
This study was supported by NIH grants, R01-AR076328-01A1, R01-AR076985-01A1, and R01-AR078308-01A1 and was performed under the rubric of the Center of Advanced Imaging Innovation and Research (CAI2R), an NIBIB Biomedical Technology Resource Center (NIH P41-EB017183).References
1.Ma D, Gulani V, Seiberlich N, et al. Magnetic resonance fingerprinting. Nature. 2013;495(7440):187-192. doi:10.1038/nature11971.
2.Hamilton JI, Seiberlich N. Machine learning for rapid magnetic resonance fingerprinting tissue property quantification. Proc IEEE. 2019; 108: 69-85.
3. Zhang X, Duchemin Q, Liu* K, Gultekin C, Flassbeck S, Fernandez‐Granda C, Assländer J. Cramér–Rao bound‐informed training of neural networks for quantitative MRI. Magnetic resonance in medicine. 2022 Jul;88(1):436-48.
4. Fang Z, Chen Y, Hung SC, Zhang X, Lin W, Shen D. Submillimeter MR fingerprinting using deep learning–based tissue quantification. Magnetic resonance in medicine. 2020 Aug;84(2):579-91.
5. McGivney, D. F. et al. SVD Compression for Magnetic Resonance Fingerprinting in the Time Domain. Ieee Transactions on Medical Imaging 33, 2311–2322 (2014).
6. Stupic KF, Ainslie M, Boss MA, et al. A standard system phantom for magnetic resonance imaging. Magn Reson Med. 2021; 86(3): 1194-1211. doi:10.1002/mrm.28779.
7.Sharafi A, Zibetti MVW, Chang G, Cloos M, Regatte RR. 3D MR- fingerprinting for rapid simultaneous T1, T2, and T1ρ volumetric map- ping of the human articular cartilage at 3T. NMR Biomed 2022;34(7): e4800.8. Weigel, M. Extended phase graphs: dephasing, RF pulses, and echoes - pure and simple. J Magn Reson Imaging 41, 266–295 (2015).
Figures