0512
Platelet Rich Plasma Effects on Knee Cartilage and Osteoarthritis Symptoms: T2, UTE-T2* and Patient Reported Outcomes Over 6-months Follow-Up1Orthopaedic Surgery, Stanford Univesity, Stanford, CA, United States, 2Joint Preservation Center, Palo Alto Veterans Healthcare System, Palo Alto, CA, United States
Synopsis
Keywords: Osteoarthritis, Cartilage, UTE-T2*
Motivation: Clinical evidence of structural benefits to cartilage from Platelet Rich Plasma (PRP) injections to treat knee osteoarthritis is lacking.
Goal(s): Our goal was to use T2 and UTE-T2* relaxation times to assess cartilage structural improvements following PRP therapy.
Approach: Patient reported outcomes, T2 and UTE-T2* maps were acquired before and 6 months after completion of PRP treatment in 50 patients with symptomatic knee osteoarthritis.
Results: On average, participants reported symptomatic improvements following PRP. Significant changes to cartilage T2 and UTE-T2* were also observed. Improvements in patient-reported knee function and stiffness correlated to concurrent decreases in both T2 and UTE-T2*.
Impact: qMRI evaluation of the clinical efficacy of PRP treatment of symptomatic knee OA shows that changes to patient reported knee function associate with concurrent changes to cartilage structure assessed with T2 and UTE-T2*.
INTRODUCTION
Autologous platelet rich plasma (PRP) injections are increasingly used to treat painful knee osteoarthritis (OA)1. PRP therapy is postulated to have anti-inflammatory and regenerative effects, however, individual responses to PRP treatment vary widely2 and clinical evidence of potential benefits to cartilage structure remain lacking3. Our aim was to study osteoarthritis symptoms and articular cartilage structure assessed before and 6 months after completion of PRP treatment for painful knee OA using patient reported outcomes and T2 and UTE-T2* relaxation times, quantitative MRI (qMRI) parameters known to be sensitive to cartilage matrix composition and organization4-6.METHODS
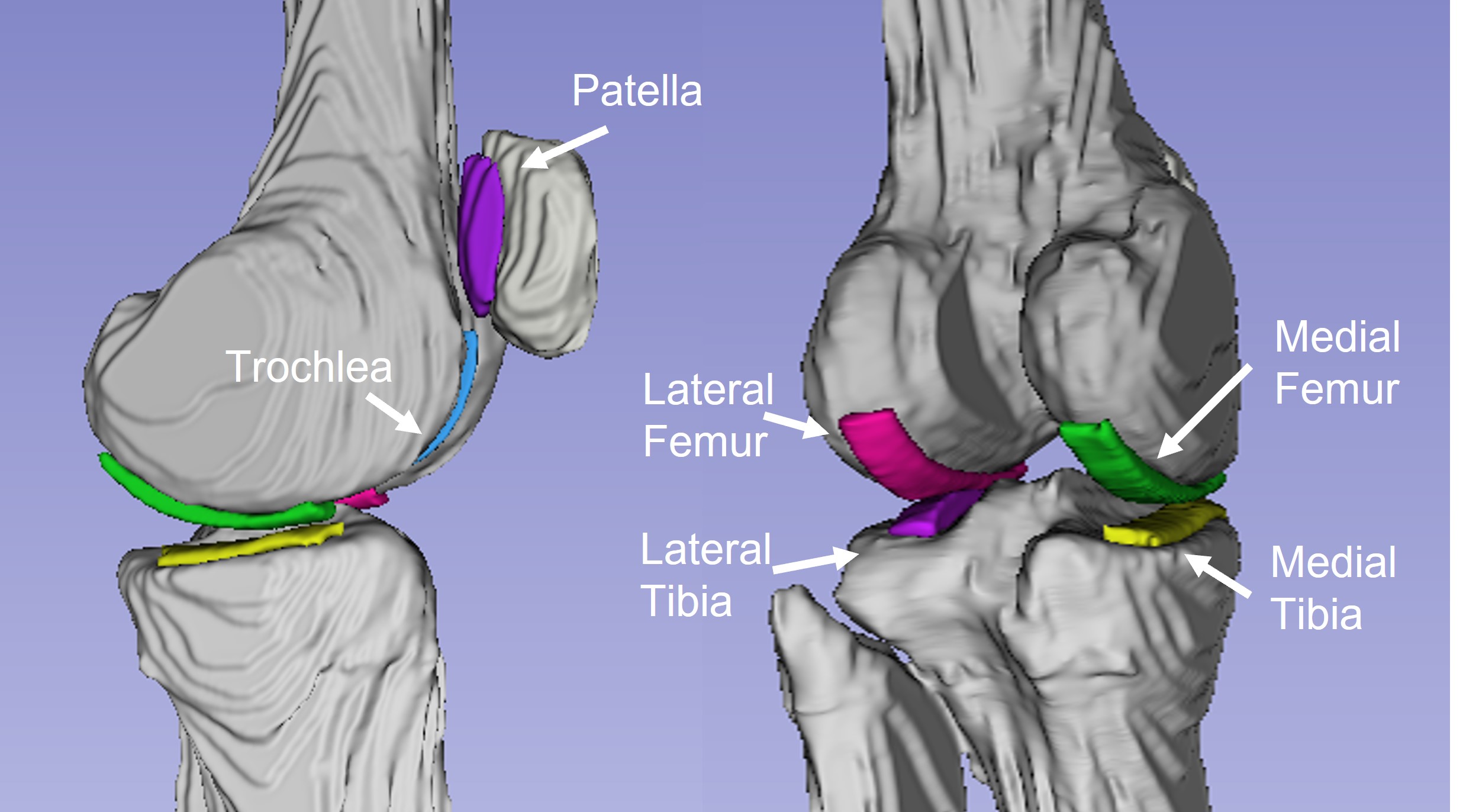
Fifty participants seeking treatment for painful knee OA (22 females; mean age 55±10 years; mean BMI 28±3 kg/m2; mean Kellgren-Lawrence grade 2.1±0.8) consented to participate in this IRB-approved study. PRP treatment consisted of a three-injection series (3.5-4ml) of autologous leukocyte-poor PRP administered within 1 month. Prior to PRP treatment and again 6 months after the last treatment, all participants completed Knee injury and Osteoarthritis Outcome Score (KOOS)7 and Western Ontario and McMasters Arthritis Index (WOMAC)8 questionnaires and underwent 3T knee MRI (GE Healthcare). T2 maps were acquired using a 2-D fast spin echo sequence with 8 echo images9 (TEs: 5-70ms, TR=1500ms, FOV=12cm, matrix=384x256 zero-filled to 512x512, 3mm slice-thickness, no gap). In a subset of 27 participants, UTE-T2* maps were acquired using a radial-out 3-D Cones sequence with 8 echo images10,11 (TEs: 32μs-16ms, TR=23ms, FOV=12cm, matrix=384x384 interpolated to 512x512, 3mm slice thickness). T2 and UTE-T2* maps were generated pixel-wise from mono-exponential fitting using Matlab (TheMathWorks) and Olea Sphere (Olea Medical), respectively. All maps were manually segmented to include 9 mm-wide strips of cartilage (largely consistent with known areas of contact during common daily activities12), from 3 contiguous slices on each of 6 surfaces of the knee: medial and lateral femurs (MFC, LFC), medial and lateral tibias (MTP, LTP), patella (PAT) and trochlea (TRO), Figure 1. T2 regions included full-thickness cartilage; UTE-T2* regions included only deep cartilage. Shapiro Wilks tests assessed normality of data sets. Paired t-tests (Wilcoxon Signed Ranks tests for non-normal data distributions) assessed longitudinal changes in KOOS, T2 and UTE-T2*. Univariate Pearson correlations (Spearman’s rho for non-normal data) assessed relationships between longitudinal (6month – baseline) KOOS and T2 or UTE-T2* changes. Effects of age, BMI, sex and KL grade were assessed with linear regression. Significance was accepted for p<0.05.RESULTS
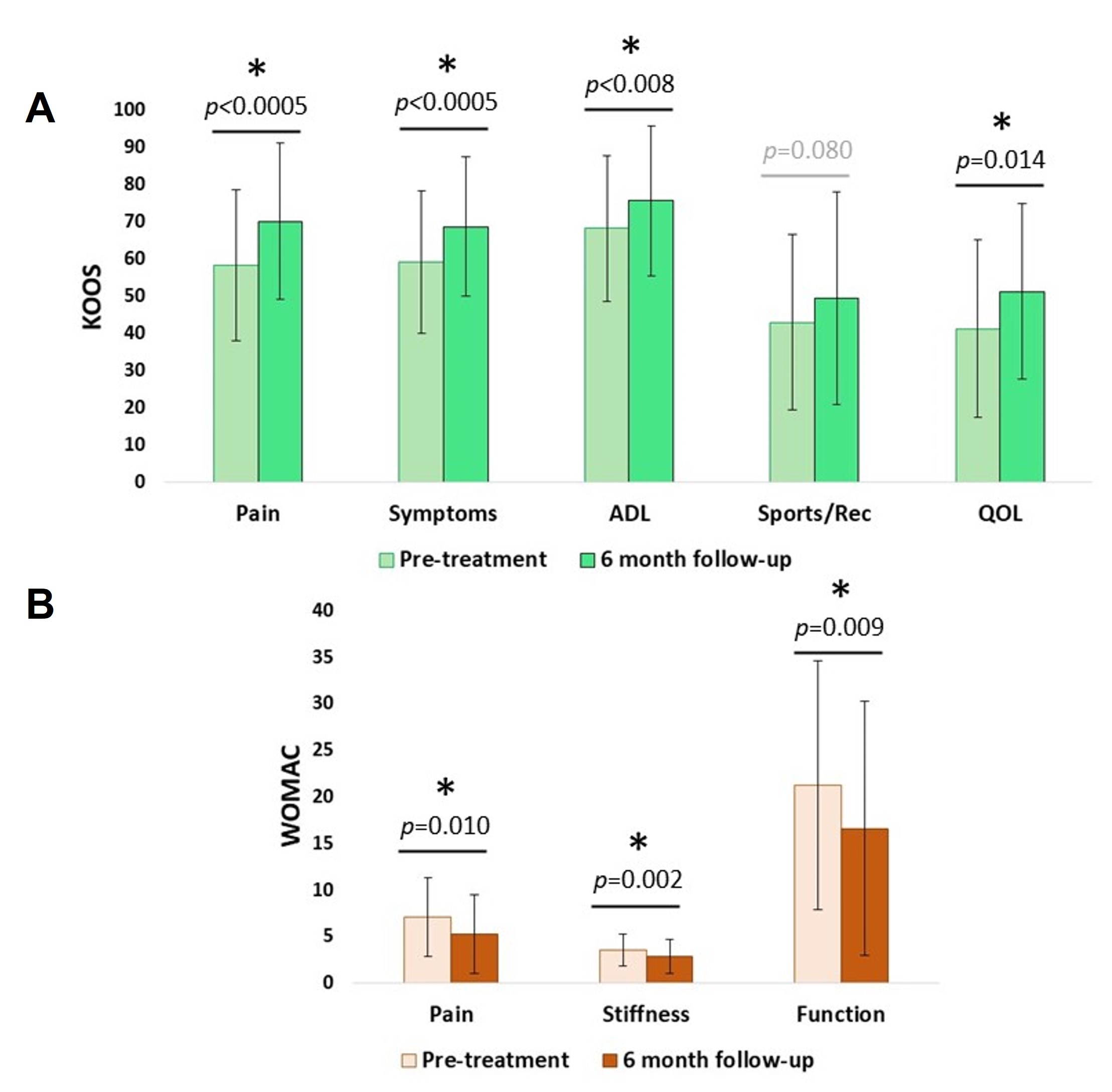
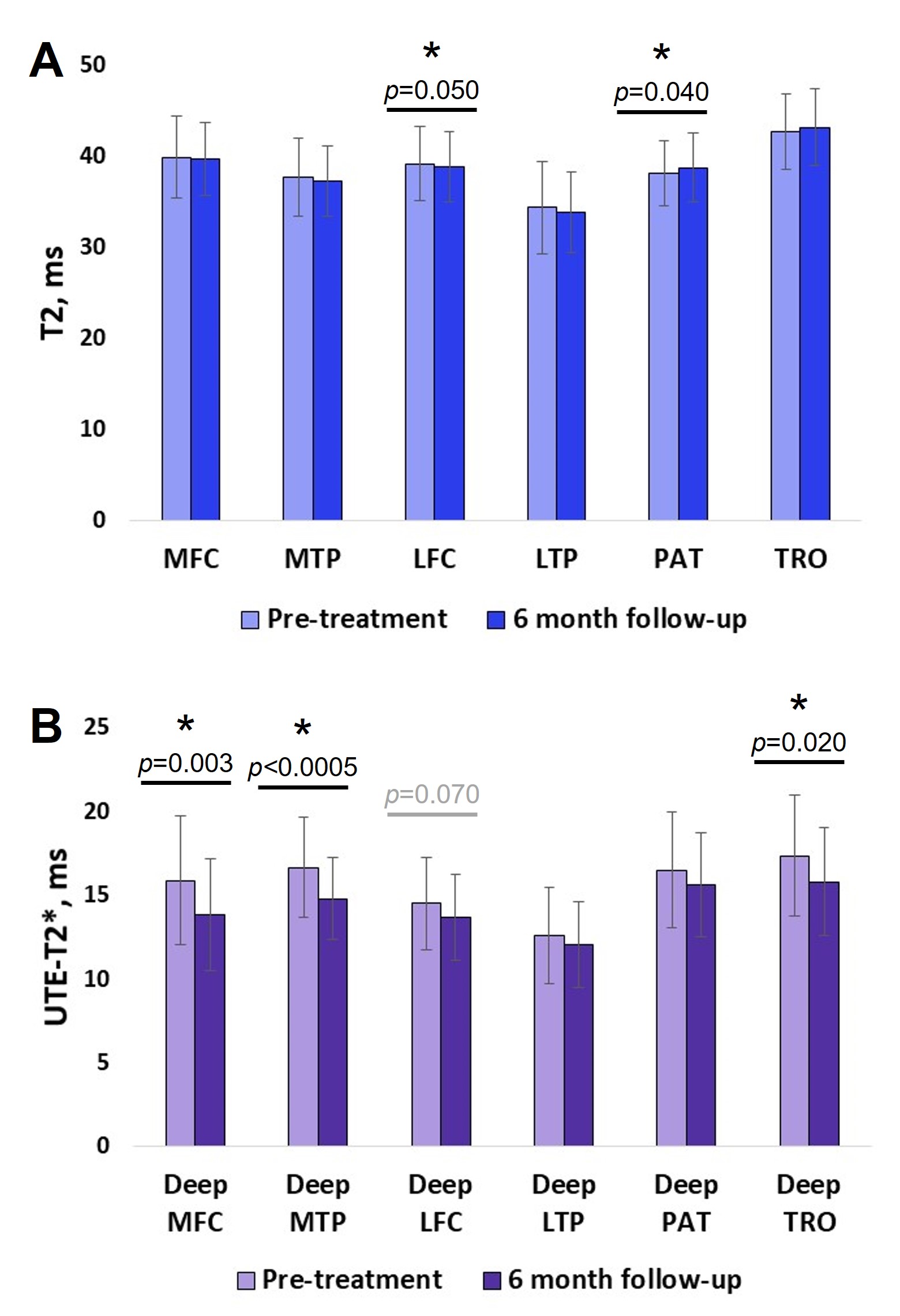
Successful pain reduction (i.e. exceeding minimal important change (MIC) after non-surgical intervention for KOOS Pain change > 12.4pts13) was achieved in 21/50 (42%) of PRP recipients 6 months following completion of the injection series. Successful functional improvement (exceeding MIC for WOMAC function change < -17pts13) was achieved in 9/50 (18%) of PRP recipients. Averaged across all participants, 4 of 5 KOOS subscores and 3 of 3 WOMAC subscores demonstrated improvements, Figure 2.Averaged across all participants, a small but significant T2 decrease was detected in LFC cartilage while a small increase was detected in PAT cartilage 6 months following completion of the PRP intervention, Figure 3a. In the subset of participants who underwent UTE-T2* mapping, substantial and significant decreases to deep cartilage UTE-T2* were detected in MFC, MTP and TRO regions, Figure 3b.
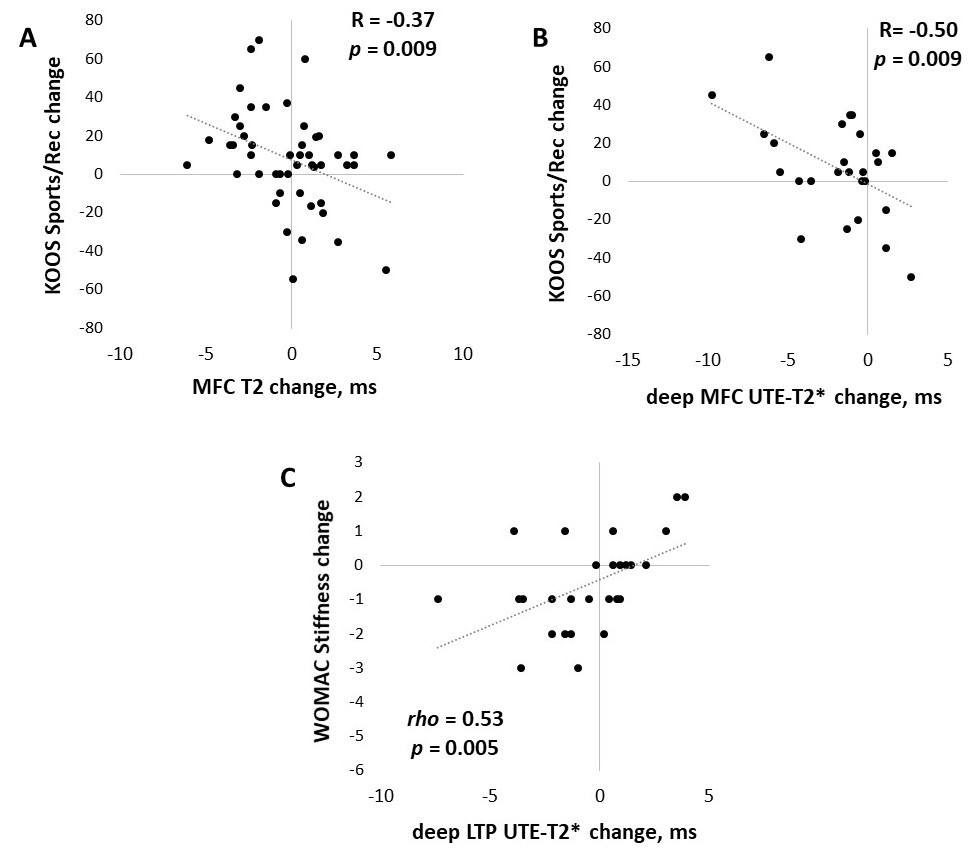
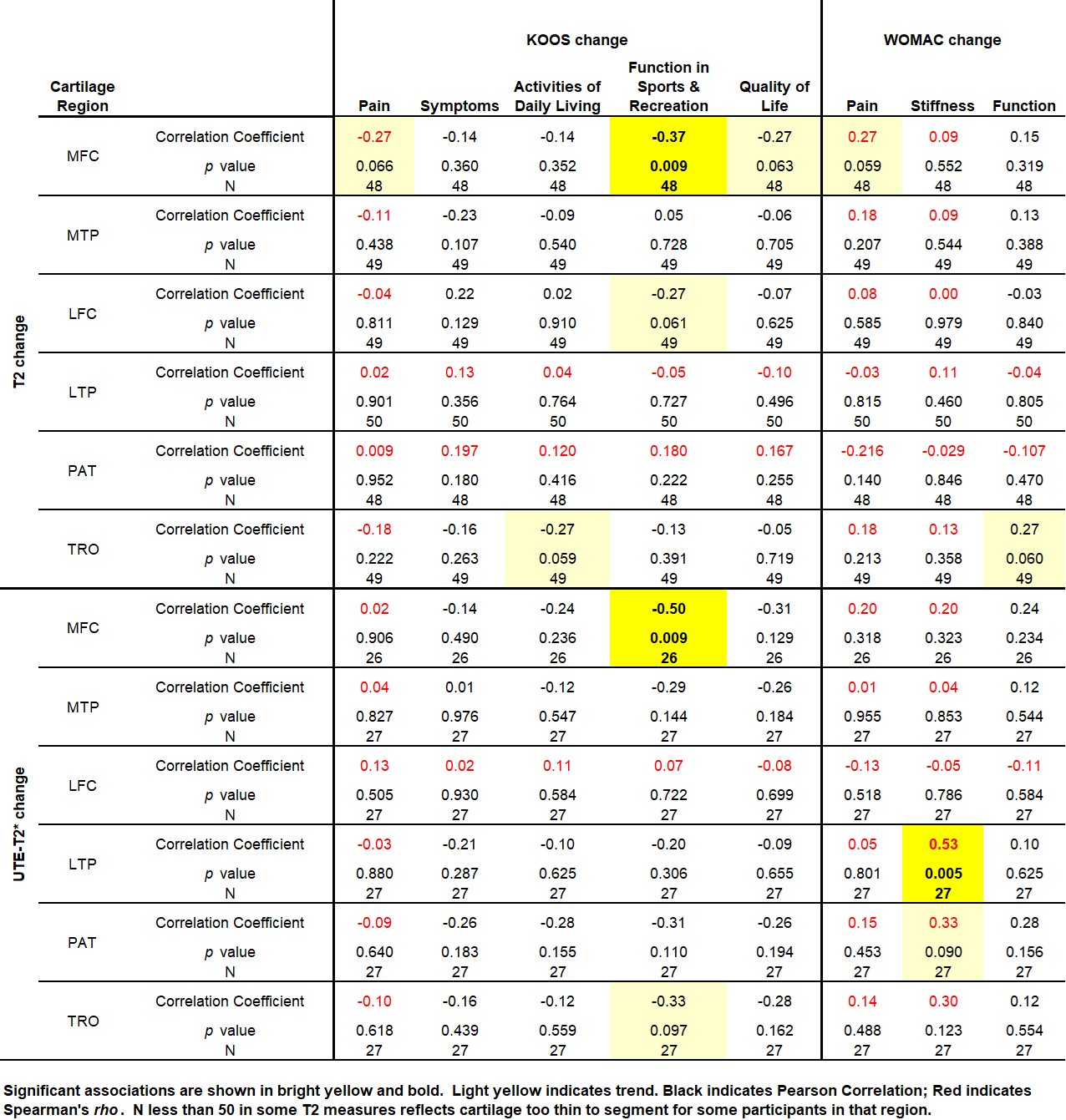
At the individual level, increases (improvements) in KOOS Sports & Recreation scores correlated to decreases (improvements) in both T2 and UTE-T2* (R=-0.37, -0.50; p=0.009, 0.009) in MFC cartilage, Figure 4a,b. Similarly, decreases (improvements) in WOMAC Stiffness correlated to decreases (improvements) in UTE-T2* (rho=0.53, p=0.005) in LTP cartilage, Figure 4c. Linear regression found no effects of age, BMI, sex or KL grade on these results. Additional trends for increasing KOOS subscores with decreasing T2 or UTE-T2* were detected Table 1.
DISCUSSION
Recipients of PRP injections in this study demonstrated wide variations in their responses to treatment but on average reported improvements to knee pain, symptoms and function 6 months following PRP intervention. Significant qMRI changes, including decreases to average deep cartilage UTE-T2* relaxation times, were also observed. On an individual level, changes in participants’ self-reports of osteoarthritis symptoms associated with 2 different quantitative MRI markers of concurrent cartilage compositional change where improved knee function or stiffness correlated to improved T2 or UTE-T2* assessments of cartilage structure. These findings are particularly notable given that a discordance between OA symptoms and structural evidence of disease is common, especially in early stages of disease14-17.CONCLUSION
qMRI evaluation of the clinical efficacy of PRP treatment of symptomatic knee OA shows that changes to patient reported knee function associate with concurrent changes to cartilage structure assessed with T2 and UTE-T2*.Acknowledgements
VA grant RX-002452 (PI-CR Chu), and DOD W81XWH-18-1-0590 (PI-CR Chu)References
- Ip HL, Nath DK, Sawleh SH, Kabir MH, Jahan N. Regenerative Medicine for Knee Osteoarthritis - The Efficacy and Safety of Intra-Articular Platelet-Rich Plasma and Mesenchymal Stem Cells Injections: A Literature Review. Cureus 2020; 12(9): e10575.
- Gato-Calvo L, Magalhaes J, Ruiz-Romero C, Blanco FJ, Burguera EF. Platelet-rich plasma in osteoarthritis treatment: review of current evidence. Ther Adv Chronic Dis 2019; 10: 2040622319825567.
- Fice MP, Miller JC, Christian R, et al. The Role of Platelet-Rich Plasma in Cartilage Pathology: An Updated Systematic Review of the Basic Science Evidence. Arthroscopy 2019; 35(3): 961-76 e3.
- Chu CR, Williams AA, West RV, et al. Quantitative Magnetic Resonance Imaging UTE-T2* Mapping of Cartilage and Meniscus Healing After Anatomic Anterior Cruciate Ligament Reconstruction. Am J Sports Med 2014; 42(8): 1847-56.
- Nissi MJ, Toyras J, Laasanen MS, et al. Proteoglycan and collagen sensitive MRI evaluation of normal and degenerated articular cartilage. J Orthop Res 2004; 22(3): 557-64.
- Williams A, Qian Y, Bear D, Chu CR. Assessing degeneration of human articular cartilage with ultra-short echo time (UTE) T2* mapping. Osteoarthritis Cartilage 2010; 18(4): 539-46.
- Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health and quality of life outcomes 2003; 1: 64.
- McConnell S, Kolopack P, Davis AM. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties. Arthritis Rheum 2001; 45(5): 453-61.
- Williams AA, Deadwiler BC, Dragoo JL, Chu CR. Cartilage Matrix Degeneration Occurs within the First Year after ACLR and Is Associated with Impaired Clinical Outcome. Cartilage 2021; 13(2_suppl): 1809S-18S.
- Gurney PT, Hargreaves BA, Nishimura DG. Design and analysis of a practical 3D cones trajectory. Magn Reson Med 2006; 55(3): 575-82.
- Williams AA, Titchenal MR, Do BH, Guha A, Chu CR. MRI UTE-T2* shows high incidence of cartilage subsurface matrix changes 2 years after ACL reconstruction. J Orthop Res 2019; 37(2): 370-7.
- Thomeer LT, Guan S, Gray HA, Pandy MG. Articular contact motion at the knee during daily activities. J Orthop Res 2022; 40(8): 1756-69.
- Silva MDC, Perriman DM, Fearon AM, Couldrick JM, Scarvell JM. Minimal important change and difference for knee osteoarthritis outcome measurement tools after non-surgical interventions: a systematic review. BMJ open 2023; 13(5): e063026.
- Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BMC Musculoskelet Disord 2008; 9: 116.
- Finan PH, Buenaver LF, Bounds SC, et al. Discordance between pain and radiographic severity in knee osteoarthritis: findings from quantitative sensory testing of central sensitization. Arthritis Rheum 2013; 65(2): 363-72.
- Guermazi A, Niu J, Hayashi D, et al. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: population based observational study (Framingham Osteoarthritis Study). BMJ 2012; 345: e5339.
- Neogi T, Felson D, Niu J, et al. Association between radiographic features of knee osteoarthritis and pain: results from two cohort studies. BMJ 2009; 339: b2844.
Figures