0510
Preoperative personalized 3D printing technology enhanced glioblastoma patient survival by improving fractal dimensions of wound surface1The Second Hospital of Lanzhou University, lanzhou, China
Synopsis
Keywords: Tumors (Post-Treatment), Tumor, Radiomics; fractal dimensions; 3D-printing technology
Motivation: This study sought to forecast the prognosis of glioblastoma patients by conducting a retrospective analysis of their fractal dimensions (FD) from postoperative multimodal MRI and radiomics features within surgical regions. Additionally, it aimed to assess the potential for improving clinical therapeutic outcomes using preoperative personalized three dimensional (3D)-printing technology.
Goal(s): Exploring whether personalised 3D-printing technology can improve surgical precision and thus prolong survival in glioblastoma patients
Approach: Using questionnaires, radiomics, and FD to evaluate whether preoperative 3D-printing technology improves postoperative outcomes and survival
Results: The FD of surgical regions was associated with overall survival, and preoperative 3D-printing improves patient prognosis and prolongs survival
Impact: Multimodal magnetic resonance imaging radiomics and fractal dimension can predict patient survival by analyzing postoperative images, while personalized 3D printing technology can improve surgical accuracy, reduce the fractal dimension of the surgical regional, and prolong the overall survival of patients
Intrduction
Clinicians have always faced the challenge of optimizing treatment measures, appropriately combining various therapeutic means, and removing the lesion while ensuring the functional area around the or glioblastoma’s special location, rapid progression, greater harm, and numerous complications.Method
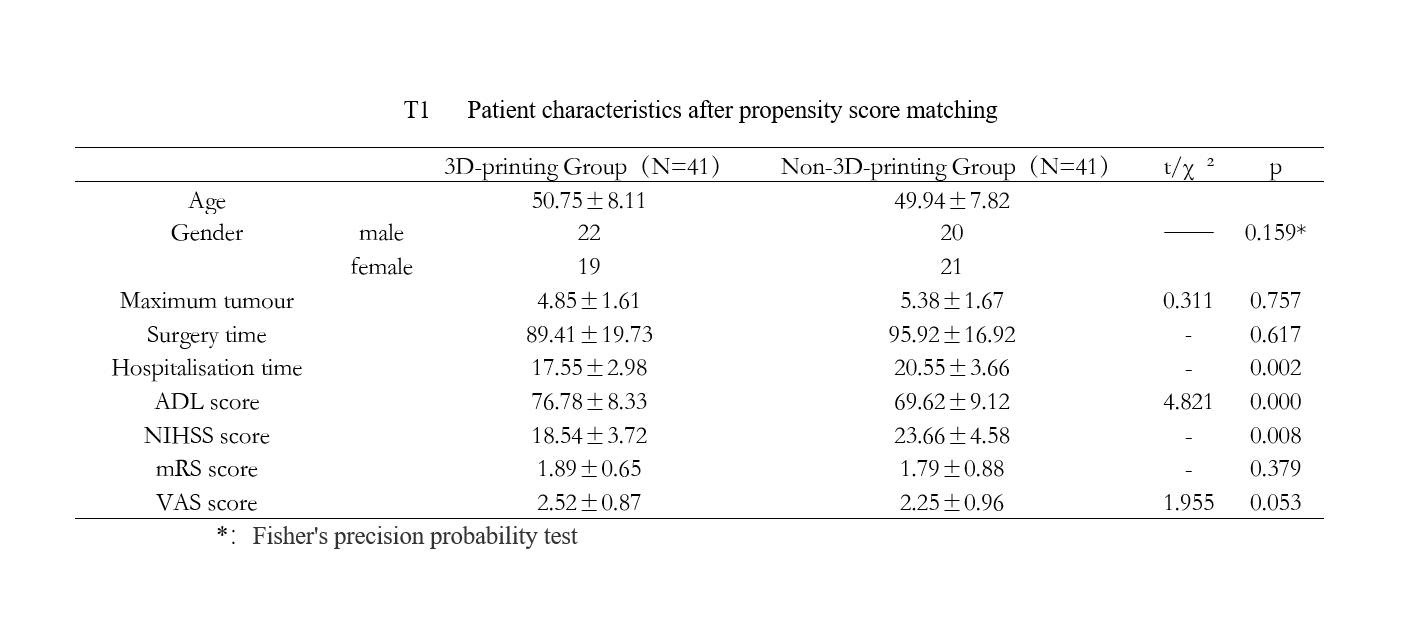
This study conducted a retrospective analysis of 161 pathologically confirmed glioblastoma cases treated at our hospital from January 2018 to January 2022. Among these cases, 42 underwent preoperative personalized 3D printing technology prior to craniotomy, while the remaining patients underwent direct craniotomy. Propensity score matching (PSM) was employed to equate the baseline characteristics of the two groups. The final match was 41 pairs of patients. The surgical boundaries were manually delineated on one-week postoperative images, including T1, T2, FLAIR, T1C, and DWI sequences. Subsequently, fractal dimensions were calculated from the binary images generated. Meanwhile, radiomics features were extracted based on the outlined images. A survival prediction model was then established by comparing surgical performance, pain severity, neurological impairment levels, prognosis, results on the activities of daily living scale, and differences in survival between the two groups.Result
The groups that underwent routine surgical procedures exhibited significantly higher levels of pain severity and neurological impairment compared to the groups that received preoperative personalized 3D printing technology. This difference was particularly pronounced in those with a shorter survival duration. However, there were no notable distinctions in their scores on the activities of daily living scale. Additionally, within-group variations were statistically significant (P<0.05). The Kaplan-Meier curve analysis revealed that an increase in DWI-FD and T2-FD was associated with a shorter overall survival (OS) (p < 0.001). Results from the ROC curve analysis showed that a fusion model based on radiomics features from postoperative MRI of the surgical area and fractal dimensions (FD) could effectively predict patients' prognosis, in which the area under the curve (AUC) was 0.853 and 0.806 in the training and validation set respectively. In contrast, the AUCs for the radiomics-features-based predictive model alone were 0.796 in the training set and 0.713 in the validation set. The use of preoperative 3D printing technology for surgical simulations proved to enhance the accuracy and precision of surgeries, leading to a reduction in the average fractal dimensions of the surgical area from 1.4325 to 1.2578. This subsequently resulted in lower levels of neurological impairment and improved progression-free and overall survival. However, it's worth noting that the technology did not significantly improve postoperative living ability and pain severity in the surgical area.discussion
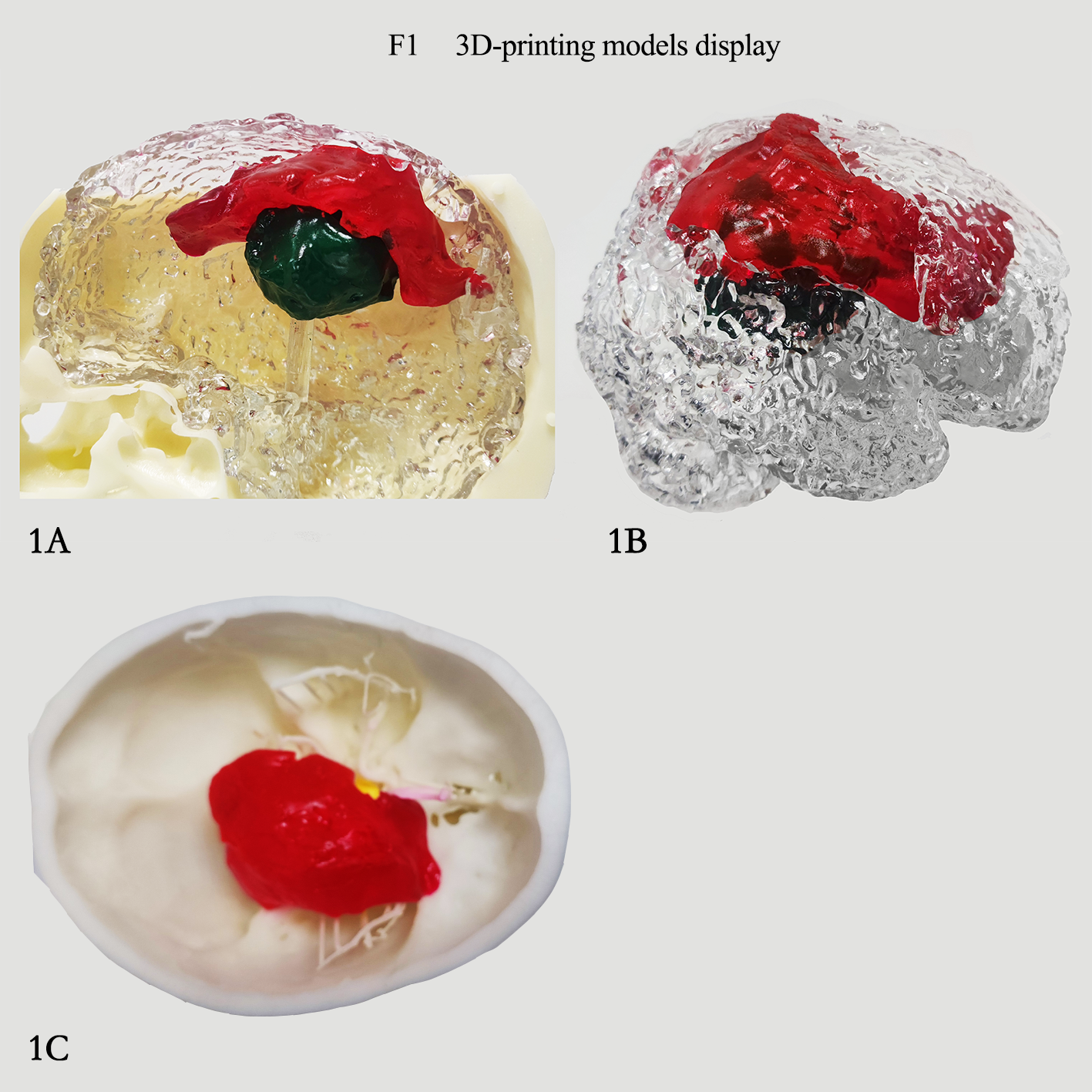
Currently, the conventional treatment pathway for gliomas is surgical resection to maximize the extent of tumor resection until a functional border is encountered, followed by radiotherapy combined with temozolomide or other alkylating agents[1-3] . However, because of the irregular morphology of the tumor and the extensive peritumoral edema, complete resection of the peritumoral edema is often not possible during clinical practice to preserve brain function. The inability to completely resect the peritumoral edema makes the infiltrated tumor cells within the peritumoral edema a serious pitfall for future progression[4,5] and Cho et al. found that more than 70% of tumor recurrences were located within the initially diagnosed peritumoral edema zone. Given the limited radiological and microscopic signs of gliomas that can be identified by the human eyes, it is necessary to more accurately identify information with other more advanced and objective methods and tools. Therefore we used Radiomics to analyse the postoperative images of the patients in the hope of uncovering information that would affect their survival. In this study, we found that the fractal dimension and MRI radiomics features of the operative area correlated with the prognosis of the patients, and patients with lower fractal dimensions had a longer survival time. Also after propensity-matched comparison of the two groups formed it was found that preoperative personalised 3D-printing of patients reduced the fractal dimension. The group of patients who used 3D-printing for preoperative evaluation also had a longer average survival time than those who didn't This is because Personalized 3D-printing technology allows neurosurgeons to visualize the location of the patient’s lesion, the extent of infiltration, and the size of the edema in the surrounding tissues and to accurately locate the anatomical structures through 3D-printing models. It can also increase the precision of surgical resection and reduce unnecessary damage to peripheral nerve fiber bundles.Conclusion
Preoperative 3D-printing technology was demonstrated to significantly enhance the accuracy and precision of surgeries, resulting in reduced fractal dimensions within the surgical area for glioblastoma patients with comparable clinical conditions. This improvement led to a reduction in neurological impairments and subsequently extended patients’ life expectancy.Acknowledgements
No acknowledgement found.References
【1】Stupp R, Brada M, van den Bent MJ, et al. High-grade glioma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2014) 25:iii93–iii101. DOI:10.1093/annonc/mdu050。
【2】Witteler J, Kjaer TW, Tvilsted S, et al. Re-Evaluation of prognostic factors for survival after radiotherapy of cerebral gliomas: a supplementary analysis to a previous study. Anticancer Res. (2020) 40(11):6513–5. DOI:10.21873/anticanres.14674.
【3】Ragnhildstveit A, Li C, Zimmerman MH, et al. Intra-operative applications of augmented reality in glioma surgery: a systematic review. Front Surg. 2023 Aug 21;10:1245851. DOI:10.3389/fsurg.2023.1245851.
【4】L Sheng. The value of magnetic resonance perfusion imaging in the differential diagnosis of high-grade glioma and single brain metastases[J].Chinese Journal of Medical Physics,2019,36(7):808-810. DOI: 10.3969/j.issn.1005-202X.2019.07.012。
【5】Tang W,Chen Y,Wang X,et al. Expression of CXC-motif-chemokine 12 and the receptor C-X-C receptor 4 in glioma and theeffect on peri tumoral brain edema[J].Oncol Lett,2018,15(2):2501-2507. DOI: 10.3892/ol.2017.7547.
Figures
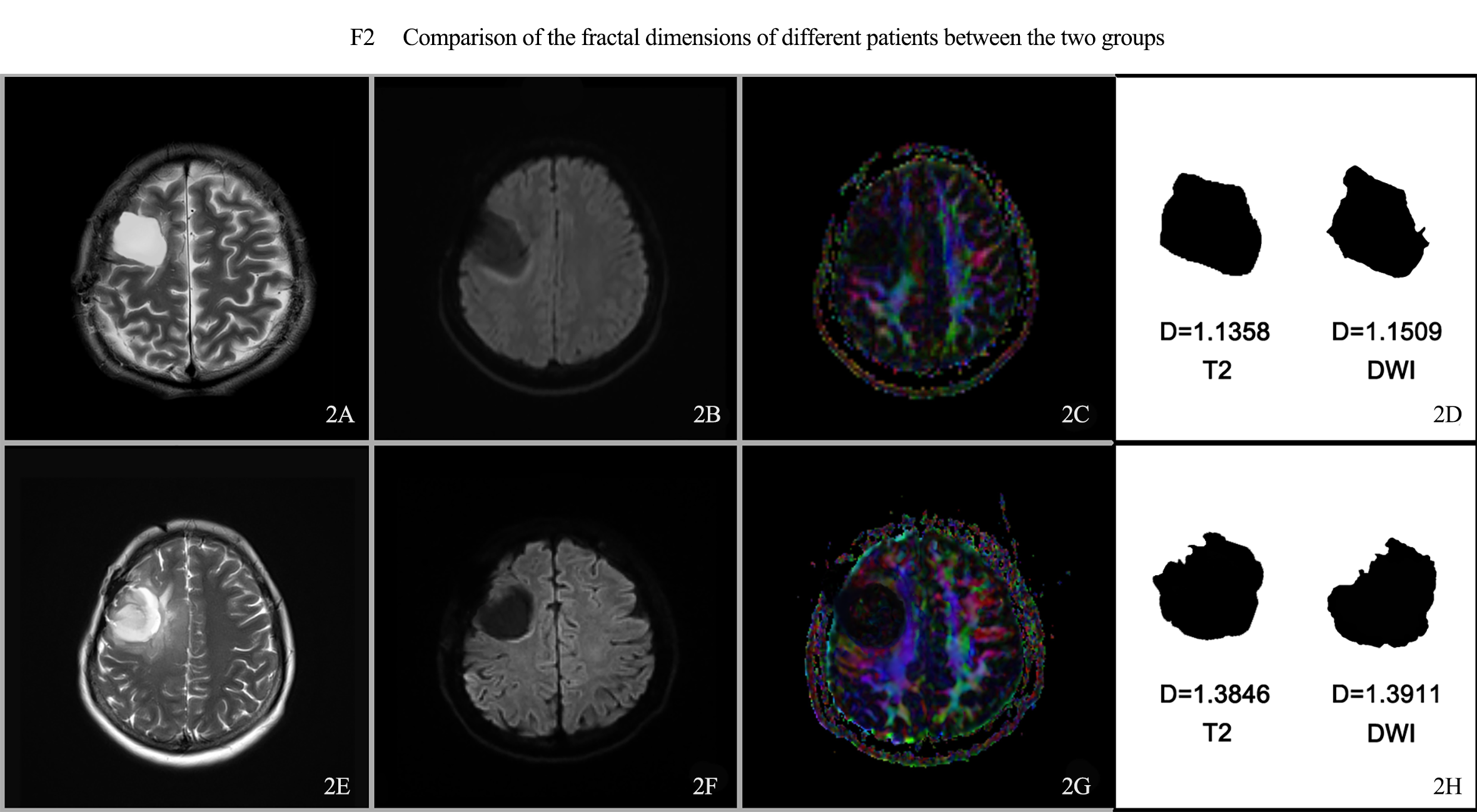
2A-2D: female, 22 years old, right frontal glioblastoma, preoperative evaluation and simulated surgical plan using personalized 3D printing technology, postoperative DTI showed that the right frontal lobe lesion area, the right corticospinal tract and the surrounding sulcus gyrus tract were discontinuous, and no interruption of nerve fiber bundle continuity was observed.
2E-2H: female, 29 years old, right frontal glioblastoma, conventional surgical treatment, postoperative DTI showed that the corticospinal tract around the right frontal lobe lesion was interrupted.
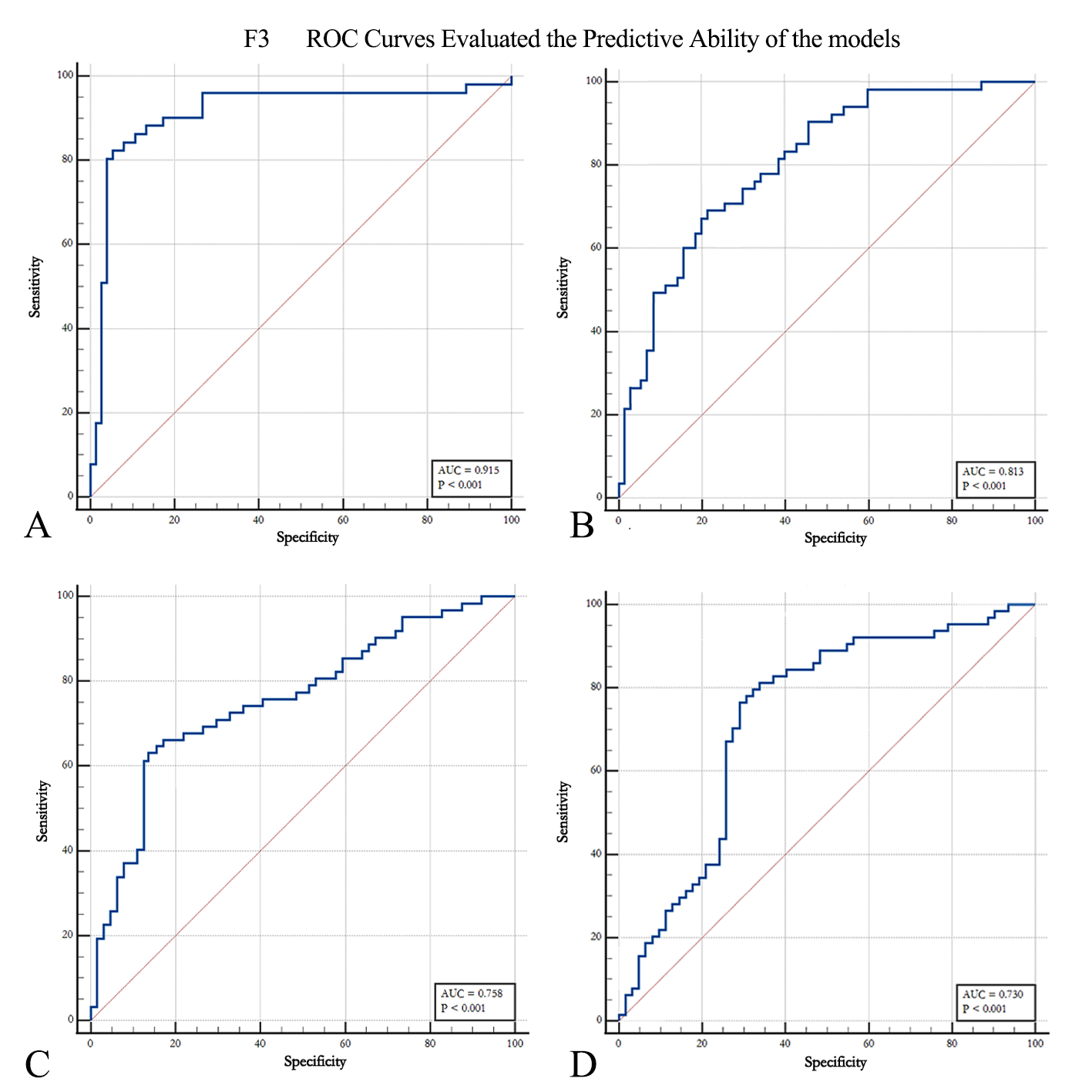
A: Fusion model training set
B: Fusion model validation Set
C: Radiomics model training set
D: Radiomics model validation set
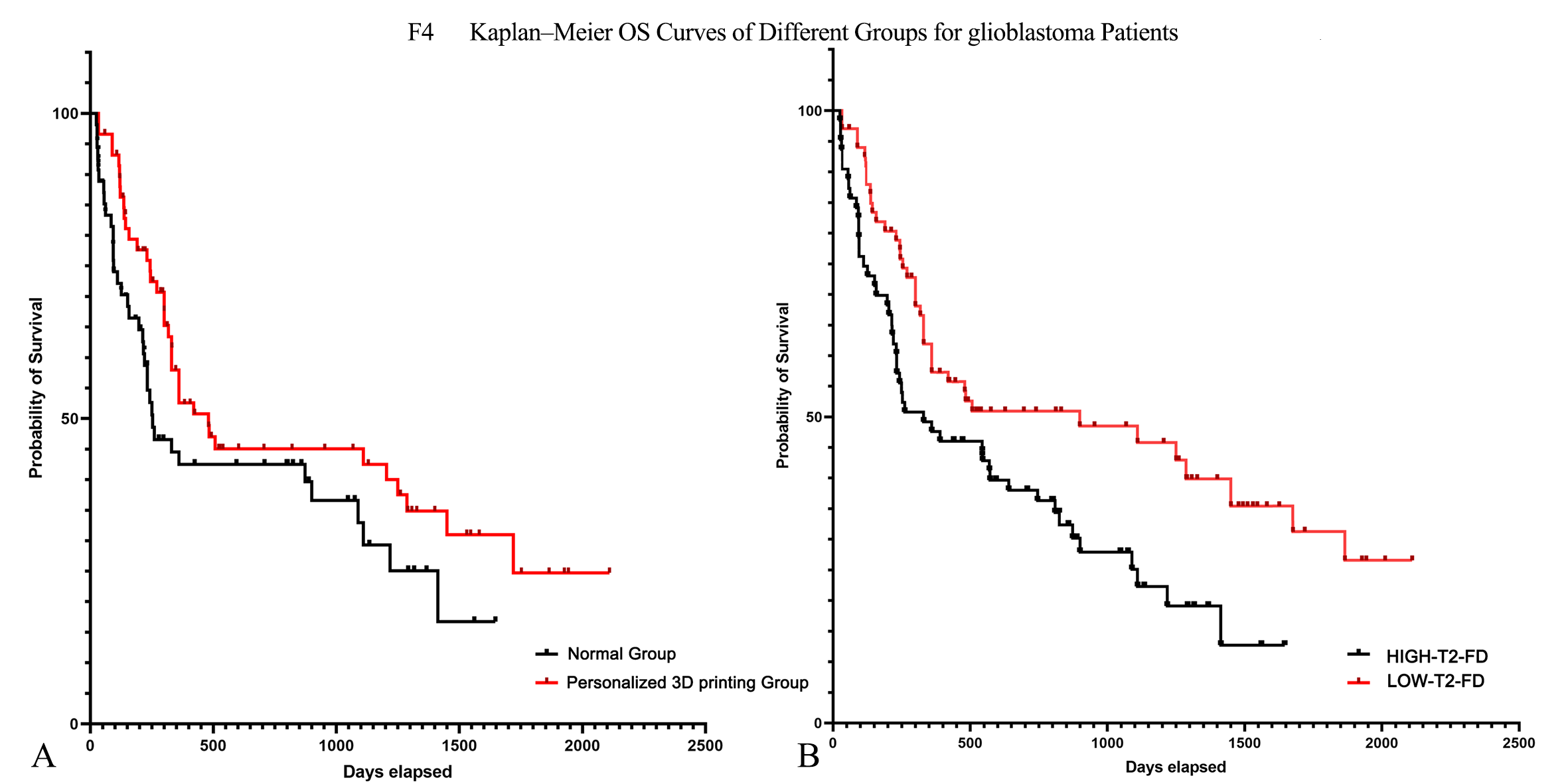
A:The survival curves plotted after grouping patients were assessed based on whether a 3D printed model was used preoperatively
B: Survival curves plotted after grouping all patients according to fractal dimension cut-off values