0502
Multiband Real-Time MRI at high frame rate (80fps) for studying the kinematics of joint movement in health and disease.1School of Physics, Engineering and Technology, University of York, York, United Kingdom, 2School of Psychology, University of Nottingham, Nottingham, United Kingdom, 3Sports and Exercise Sciences, Manchester Metropolitan University, Manchester, United Kingdom, 4York Cross-disciplinary Centre for Systems Analysis, University of York, York, United Kingdom
Synopsis
Keywords: Whole Joint, Data Acquisition, Real Time MRI
Motivation: Our research addresses the need for improved imaging techniques to assess joint kinematics in orthopedic and neuro-pathological conditions, with a focus on osteoarthritis.
Goal(s): The goal of this project is to investigate the capability of real-time MRI to assess joint mobility and function to aid clinical diagnosis and health/exercise research.
Approach: We use a multi-band real-time MRI sequence, capturing joint movement at 80 frames per second in various body parts, including the mouth, temporo-mandibular joint, thumb, knee, and foot/ankle.
Results: We demonstrate the feasibility of real-time MRI, offering detailed kinematic information while retaining soft tissue contrast.
Impact: Our real-time MRI technique, capturing joint motion at 80 frames per second, can empower clinical diagnostics and health research related to joint kinematics. It offers precise, dynamic insights into joint function, potentially improving patient care and advancing scientific understanding.
Introduction
Orthopedic and neuropathological conditions can potentially lead to or be affected by joint instability1,2. For example, osteoarthritis (OA), characterized by degeneration of cartilage leading to joint deformity, is the predominant source of chronic musculoskeletal pain worldwide. An estimated 28% of the adult population (1/3 women vs ¼ men)4 aged 60+ are affected3. The huge annual healthcare costs and the associated lost working days represent a significant socioeconomic burden. Imaging can help deliver an in-depth understanding of joint deformity to inform treatment pathways.While kinematic gait analysis with external motion capture devices (now promoted with marker-less tracking5) allows assessment of biomechanics (to assess joint function across a range of motion, accelerations, and velocities), it is difficult to identify the intrinsic factors causing dysfunction or abnormal motion. Standard magnetic resonance imaging (MRI), as a traditionally static technique can meet this need in examining joints and body parts at functional rest. MRI has high soft tissue contrast and easily identifies blood vessels, musculoskeletal, (i.e., tendons, ligaments, and membranes) and nervous structures where disease related changes present. However, when conventional static MRI is used in isolation we then risk underestimating or overlooking key diagnostic findings based upon active motion/kinematics6,7.
In human medicine and health/exercise science, one can overcome this through quasi-static (images repeated after a change in position) or cine-based (imaging over repeated cycles of joint motion) MRI acquisition. Indeed while these approaches are considered a gold standard in the diagnosis of temporomandibular disorders8, the etiology of such disorders is complex, with bio-mechanical, neuromuscular, bio-physiological and biological factors. There remains a prevalence of anxiety, depression and mental disorders linked to self-isolation in response to inhibited articulation for speech formation, chewing and swallowing. In turn high suicide rates in these patient groups are common9. Faster imaging (on the order of seconds as to not lengthen diagnostic examination times), exploring joint rotation and translation, together with protrusion, retraction, and retrusion is required.
Here we demonstrate the application of multiband based real-time MRI for achieving good visualization of foot, knee, elbow, wrist, finger, and mandible joint movement at 80 frames per second. Our technique was feasible in all regions examined. Our data show that simultaneous multi-slice, high frame rate, real-time MRI is a novel imaging technique coupling both the excellent soft tissue contrast and multiplanar capabilities of traditional MRI with kinematic information for further clinical and health/exercise research applications.
Methods
Data were acquired on a Siemens 3T MAGNETOM Vida wide bore (70cm) system (preinstalled XQ gradients 45mT/m @ 200 T/m/s), following ethical approval at Manchester Metropolitan University (Manchester, UK), using a variety of multichannel array coils for RF reception (depending on the target joint).. Radial multiband images were acquired using an adapted radial FLASH pulse sequence10,11. The sequence parameters were TR/TE = 2.5ms/1.4ms, bandwidth = 1444 Hz/pixel, slice thickness = 8mm and 288 read points (including 2x oversampling). CAIPIRINHA was used to modulate RF phase and aid slice separation12. K-space was filled using 95 radial spokes, using 5 shots across 19 segments resulting in an image time of 240ms. A sliding window was used to increase the apparent temporal resolution to 12.5ms (80fps – figure 1)13. . Dynamic repeats were completed over a movement task to the comfort of the participant. Image reconstruction utilized the Alternating Direction Method of Multipliers (ADMM) algorithm14.Results
We assessed the value of real time MR imaging at 80fps for imaging the kinematics of several key moving body parts, including i) mouth/tongue, ii) temporomandibular joint (TMJ), iii) thumb, iv) knee and v) foot/ankle. Figure 2 shows example still images from the dynamic series (~20s) captured for each joint (top row at rest, bottom row during dynamic movement). Images of the mouth were single slice reconstructed via gridding (figure 2i). Use of the ADMM algorithm to reconstruct multi-slice data dramatically reduces radial acquisition noise (figure 2ii-v). Images reach magnetization saturation (due to T1 relaxation) within 1 second. Example multi-slice imaging is shown in figure 3.Discussion
The fast-switching gradients on modern MRI scanners, alongside iterative image reconstruction, now permit deployment of real time imaging. Alongside important cardiac applications, real time (RT) MRI offers new opportunities for the non-invasive functional monitoring of the mechanics of speech/swallowing and joint kinematics/mobility. In health/sports science quantitative monitoring of such mechanics finds relevance before and after surgery/injury. We have identified key points needed for establishing RT MRI methodologies in joint kinematic applications. Our protocols will augment more traditional diagnostic imaging approaches, structural MRI (figure 4) or others. Next steps include clinical exploration and evaluation as part of a longitudinal study.Acknowledgements
IW acknowledges a PhD scholarship by the School of Physics, Engineering and Technology, University of York. JSM/AJK acknowledge provision of MR scanning time from the Manchester Metropolitan University.References
1. Wang, F. et al. The mechanisms and treatments of muscular pathological changes in immobilization-induced joint contracture: A literature review. Chin. J. Traumatol. 22, 93–98 (2019).
2. National Academies of Sciences, Engineering et al. Musculoskeletal Disorders. (National Academies Press, 2020).
3. Valdes, A. M. & Stocks, J. Osteoarthritis and Ageing. Eur. Med. J. (Chelmsf.) 116–123 (2018) doi:10.33590/emj/10313855.
4. Registered charity in England and wales no. 2077711, Scotland no. SCO41156 A company registered in England and wales and limited by guarantee no. 490500. https://www.versusarthritis.org/media/2115/osteoarthritis-in-general-practice.pdf.
5. McGuirk, T. E., Perry, E. S., Sihanath, W. B., Riazati, S. & Patten, C. Feasibility of markerless motion capture for three-dimensional gait assessment in community settings. Front. Hum. Neurosci. 16, (2022).
6. Michelini, G. et al. Dynamic MRI in the evaluation of the spine: state of the art. Acta Biomed. 89, 89–101 (2018).
7. Garetier, M. et al. Dynamic MRI for articulating joint evaluation on 1.5 T and 3.0 T scanners: setup, protocols, and real-time sequences. Insights Imaging 11, (2020).
8. Behr, M., Held, P., Leibrock, A., Fellner, C. & Handel, G. Diagnostic potential of pseudo-dynamic MRI (CINE mode) for evaluation of internal derangement of the TMJ. Eur. J. Radiol. 23, 212–215 (1996).
9. Park, S., Heo, H. A., Yun, K.-I. & Pyo, S. W. High prevalence of stress and suicidal ideation in women with temporomandibular disorder: A population-based cross-sectional survey. Cranio 40, 174–180 (2022).
10. Nayak, K. S., Lim, Y., Campbell-Washburn, A. E. & Steeden, J. Real-time magnetic resonance imaging. J. Magn. Reson. Imaging 55, 81–99 (2022).
11. Kennerley, A. J., Mitchell, D. A., Sebald, A. & Watson, I. Real-time magnetic resonance imaging: mechanics of oral and facial function. Br. J. Oral Maxillofac. Surg. 60, 596–603 (2022).
12. Yutzy, S. R., Seiberlich, N., Duerk, J. L. & Griswold, M. A. Improvements in multislice parallel imaging using radial CAIPIRINHA. Magn. Reson. Med. 65, 1630–1637 (2011).
13. Block, K. T., Uecker, M. & Frahm, J. Undersampled radial MRI with multiple coils. Iterative image reconstruction using a total variation constraint. Magn. Reson. Med. 57, 1086–1098 (2007).
14. Boyd, S. Distributed optimization and statistical learning via the alternating direction method of multipliers. Found. Trends® Mach. Learn. 3, 1–122 (2010).
Figures
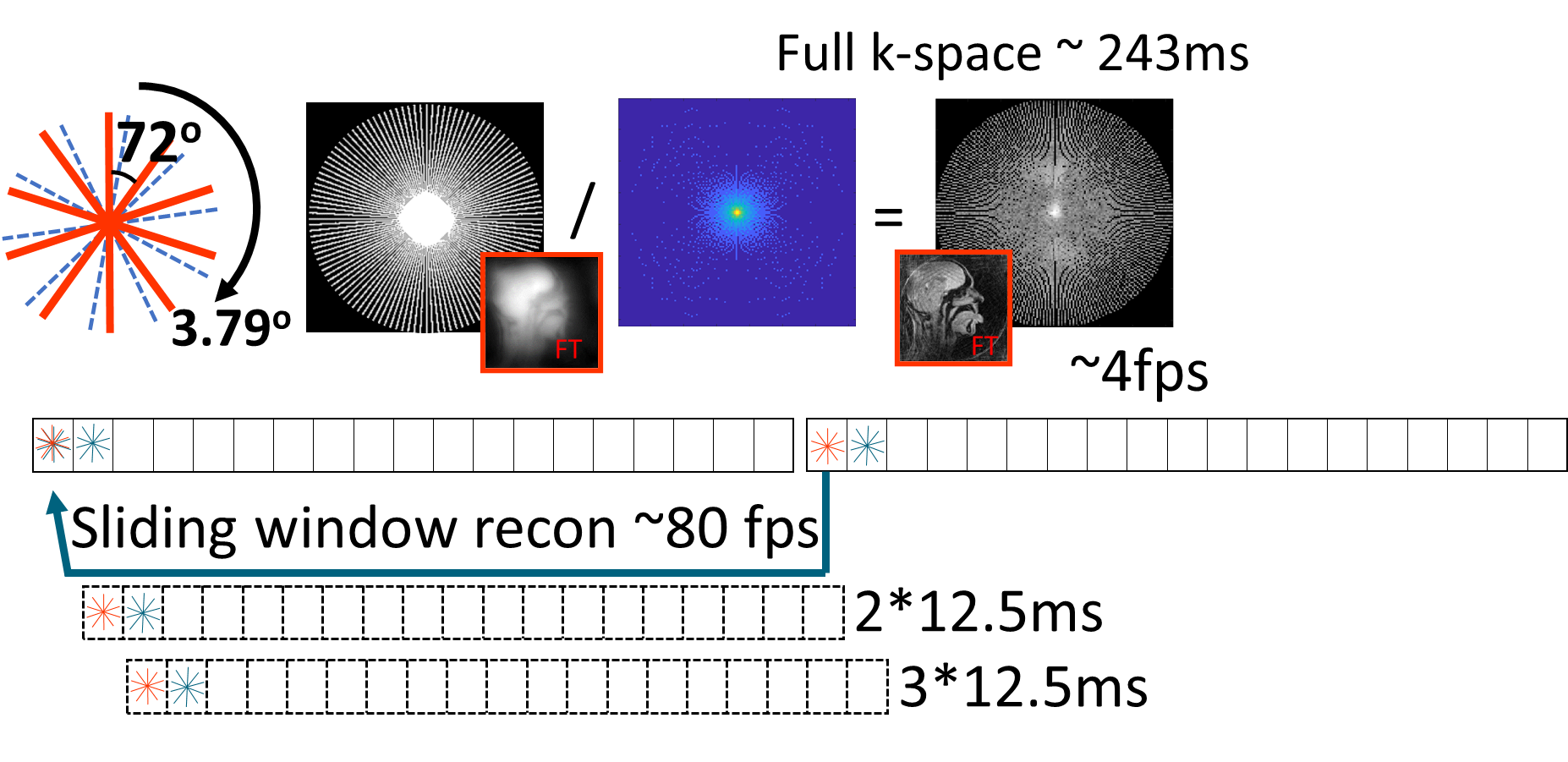
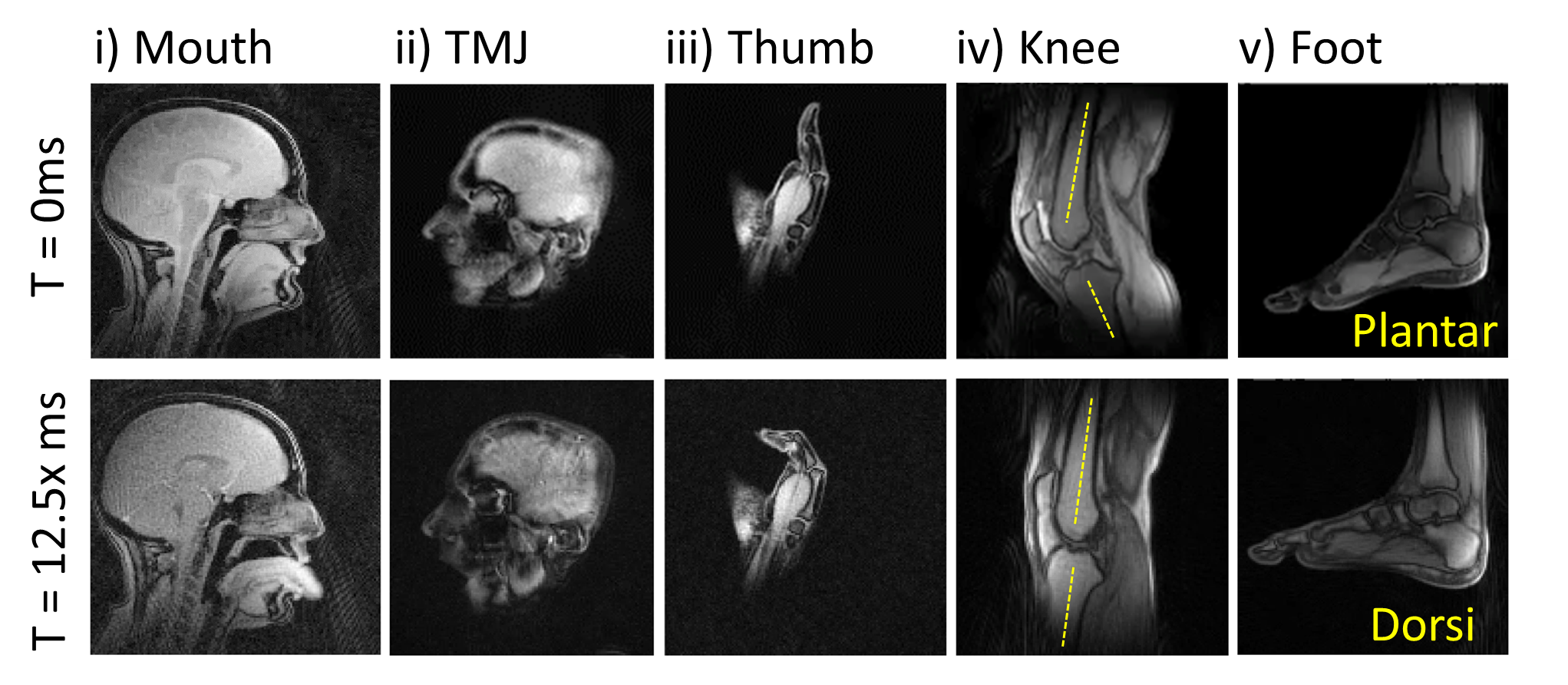
Figure 2 - Still images from real-time series data for tested joints. Row 1 shows position at the start of the acquisition (T=0ms). Row 2 shows position following several 12.5 frames from the beginning of acquisition, highlighting maximum position change for (i) mouth, (ii) temporomandibular joint, (iii) thumb, (iv) knee, and (v) foot. Effects of magnetization saturation are visible for ~1s. Cartesian re-gridding reconstruction background noise apparent in (i) mouth images. Reco is improved using Alternating Direction Method of Multipliers (ADMM) algorithm for other joints.
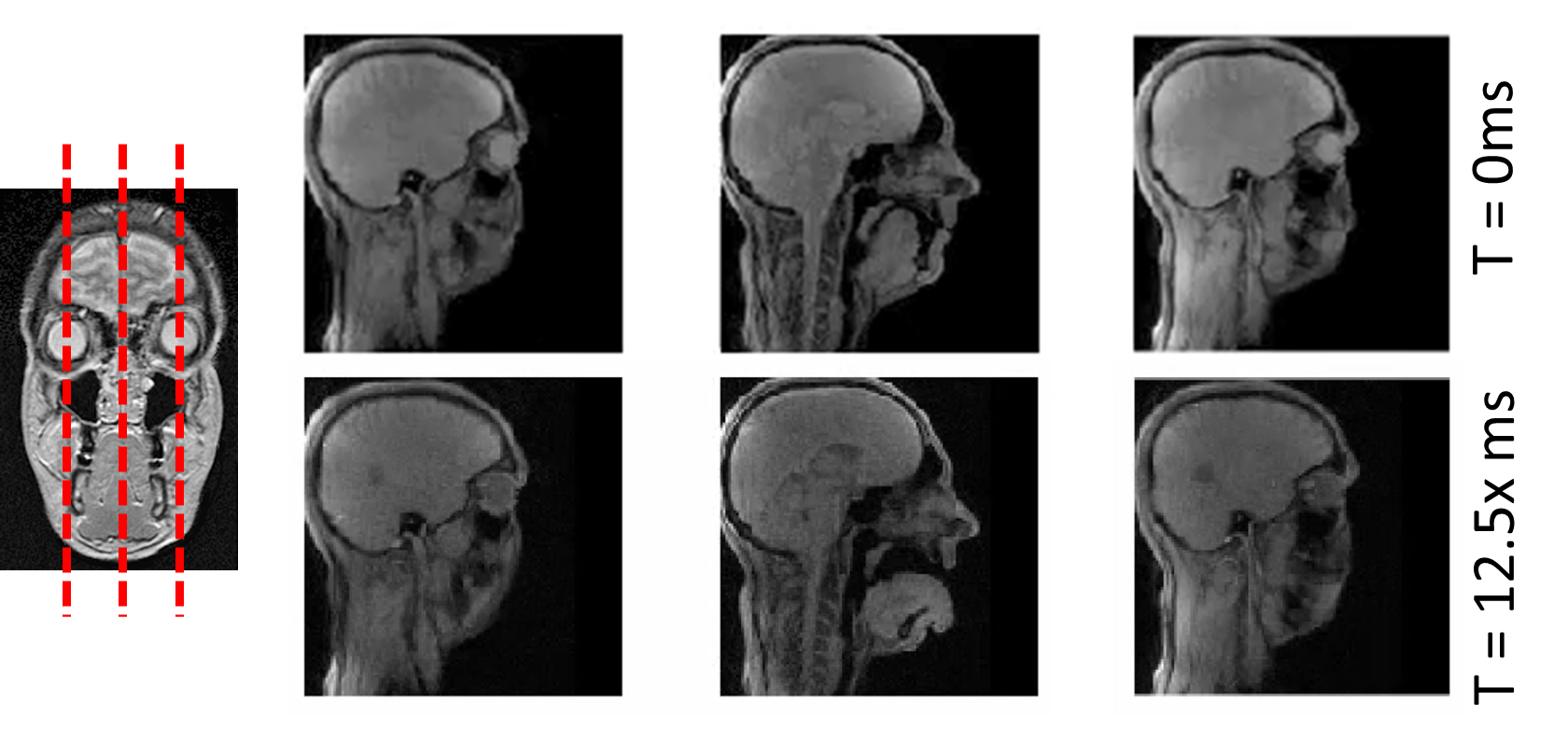
Figure 3 - Schematic and example of multi-slice acquisition. On the left, representation of the slice positioning (red dashed lines) onto coronal view of the head. Panels on the right show images at different time points (row 1 for start of acquisition, row 2 for time at maximum extension of movement) for the three slices acquired (column 1, column 2, column 3). Again, tissue contrast allows identification of specific structures around the tongue/mouth region, with critically reduced radial acquisition noise in the reconstructed multi-slice images.
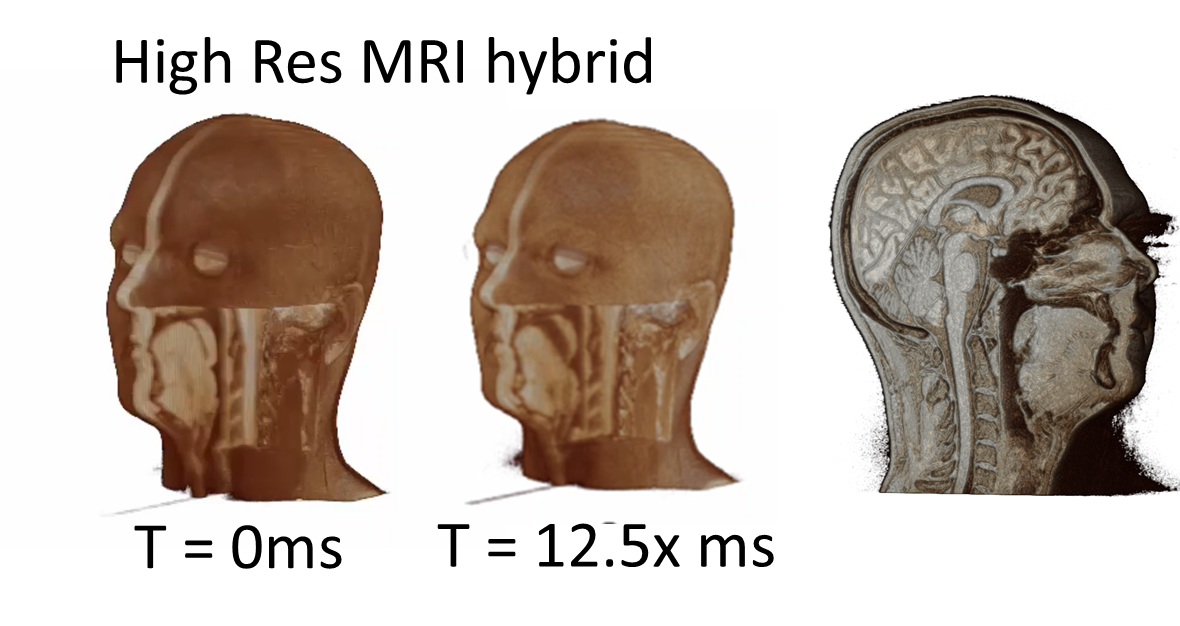
Figure 4 - Example of hybrid approach. Here classical, static, structural MR images are combined with dynamic, real-time acquisitions to augment investigation of structures. This approach can not only identify specific body regions thanks to high contrast and resolution, but also provide insights into changes in such structures during movement. This in turn can inform diagnostics and aid surgery to prevent and lessen post-traumatic/side-effect lesions, facilitating recovery.