0492
Direct MRI of Collagen1Institute for Biomedical Engineering, ETH Zurich and University of Zurich, Zurich, Switzerland
Synopsis
Keywords: Bone, MSK, Collagen
Motivation: Diseases in the musculoskeletal system are often characterized by a change in collagen structure and content. Such diseases are common and methods to evaluate collagen are integral in diagnosis and monitoring. Currently, indirect techniques are used for MRI of collagen due to its extremely short T2.
Goal(s): To directly image collagen.
Approach: Bone and tendon specimens, as well as an in-vivo hand, are imaged using advanced short-T2 techniques. The rapidly decaying signal is captured at different echo times, and image subtraction is used to isolate the signal of interest.
Results: Direct collagen MRI was successfully performed with decent SNR and resolution.
Impact: Direct MRI of collagen is reported with the potential for improved evaluation of the collagen structure and content with possible applications in diagnosis and monitoring of collagen-related diseases.
Introduction
In vertebrates, in particular in the musculoskeletal (MSK) system, the extracellular matrix (ECM) supports tissue structure, cell adhesion, and movement, and is crucial for strength and flexibility [1]. Prevalent ECM-based abnormalities in the MSK, such as arthritis, warrant the development of MRI methods to further evaluate ECM-related diseases [2]. The ECM is composed of various protein components, of which collagen is a key contributor [3].Collagen exhibits T2 on the order of approximately 10µs [4-7]. So far, the associated extremely rapid signal decay has hindered the direct observation of collagen with MRI. Instead, protons on the collagen backbone have been studied through imaging of the collagen-bound water [8-10] (T2 of 100s of µs [4,11] ), or through magnetization transfer imaging in tendon [12] and cortical bone [13]. Direct observation of the collagen signal could complement present methods and further support their use in clinical applications. Ultra-short echo time imaging on a clinical scanner, however, has been shown not to capture the collagen signal [14] .
In this study, we report direct collagen imaging, deploying experimental short-T2 hardware and methodology [15]. The rapidly decaying collagen signal is observed in an image series with multiple ultra-short echo times. The approach is demonstrated in collagen-rich specimens and in-vivo in the human hand.
Methods
Fresh bovine femur and tendon were acquired from a local butcher. The acquired tissue samples were cleaned, and sections were cut to be approximately 25x10mm2. All specimens are labelled as either prepared (underwent water removal) or unprepared. For preparation, specimens were subjected to D2O exchange for 4 days (replacing the D2O after 2 days) before freeze-drying for 3 days [14]. Unprepared samples were frozen for storage and thawed prior to imaging.A 3T Philips Achieva system was used in tandem with a custom gradient, capable of exceeding 200mT/m at 100% duty cycle [16], and rapid transmit-receive switches [17]. A 1H-free loop coil with diameter of 40mm diameter was used to image the specimens, and a quadrature birdcage with 100mm diameter was used for in-vivo application.
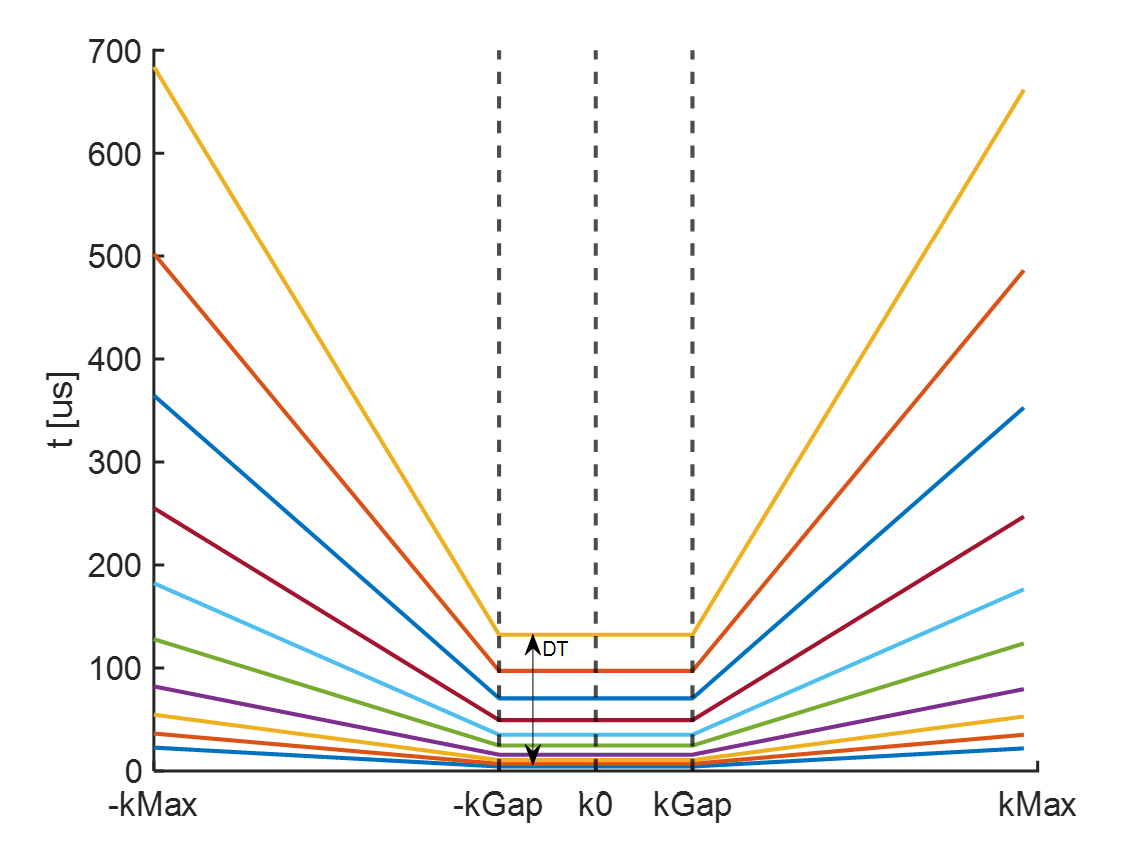
Images were acquired using a PETRA pulse sequence [18] with dead times (DT) of 10-320µs – see Figure 1. The associated effective echo times were TE = DT + dw/2, with Nyquist dwell time dw = 1/BW and imaging bandwidth BW [19]. The sequence parameters were: FOV 64mm, 3D isotropic resolution 0.67mm, angular undersampling factor 2.25. TR 3ms, 2µs block pulse, flip angle 5.7°, signal averages 3, scan time per image 2min, and BW ranging from 18.7-598kHz.
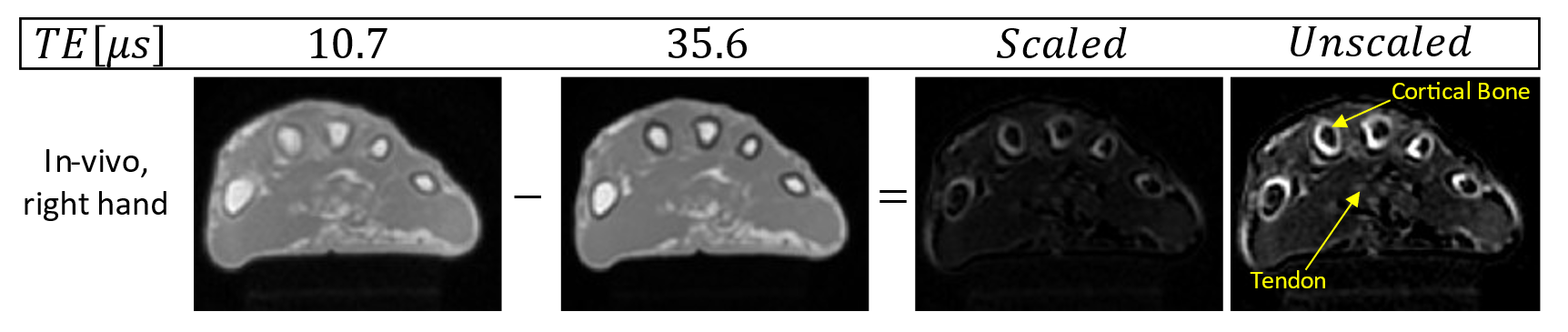
In-vivo images at DT 10µs and 33µs were acquired from the hand of a healthy volunteer, with parameters: FOV 130mm, isotropic resolution 1mm, TR 1ms, sweep pulse 2µs, flip angle 2.6°, averages 9, scan time per image 9min 38s.
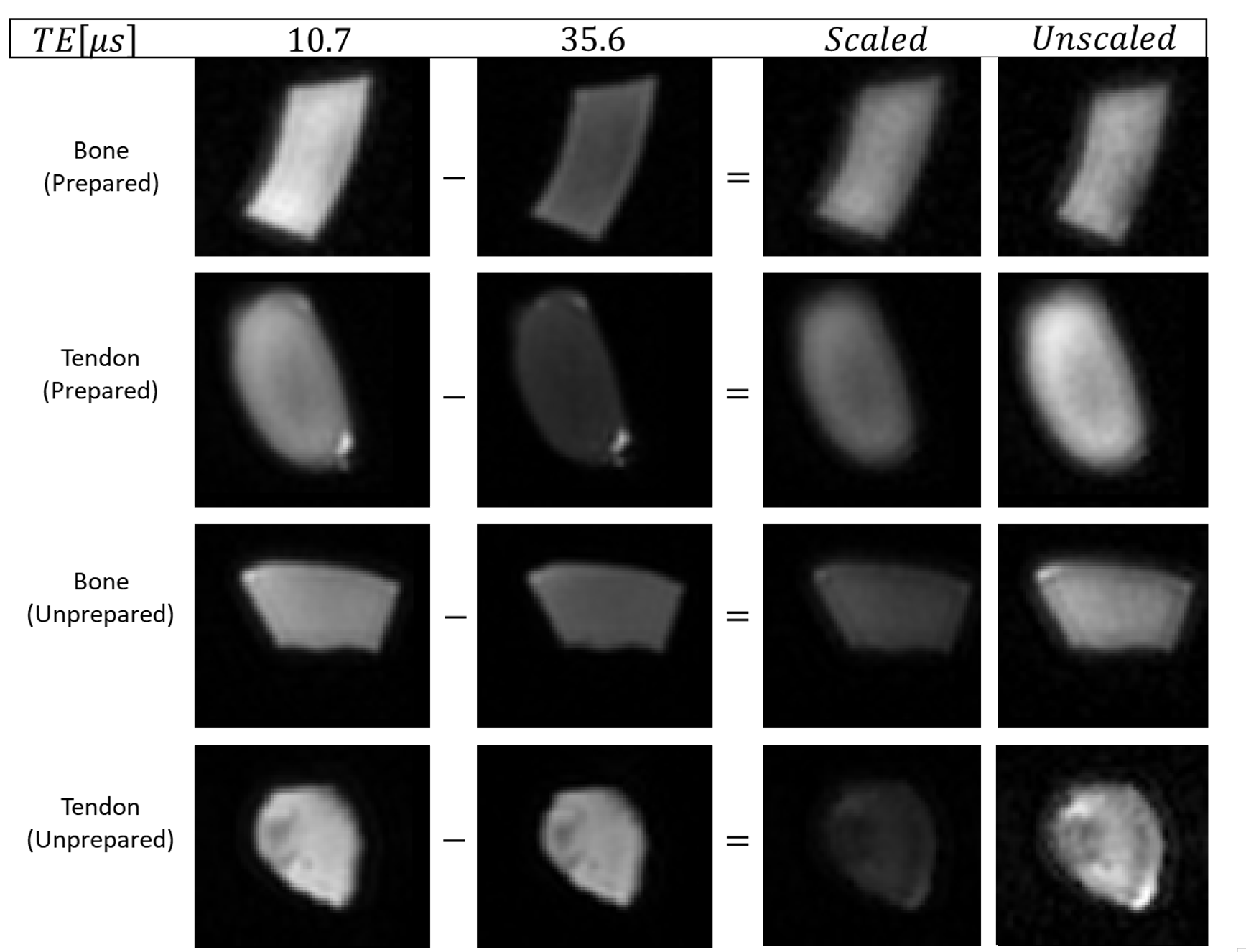
Regions of interest were drawn on the specimen images and the mean signal was determined for different TEs. Additionally, subtraction of two images with different TEs (TEshorter-TELonger) was performed on both specimen and in-vivo images to extract an image of the shortest-lived signals [20].
Results
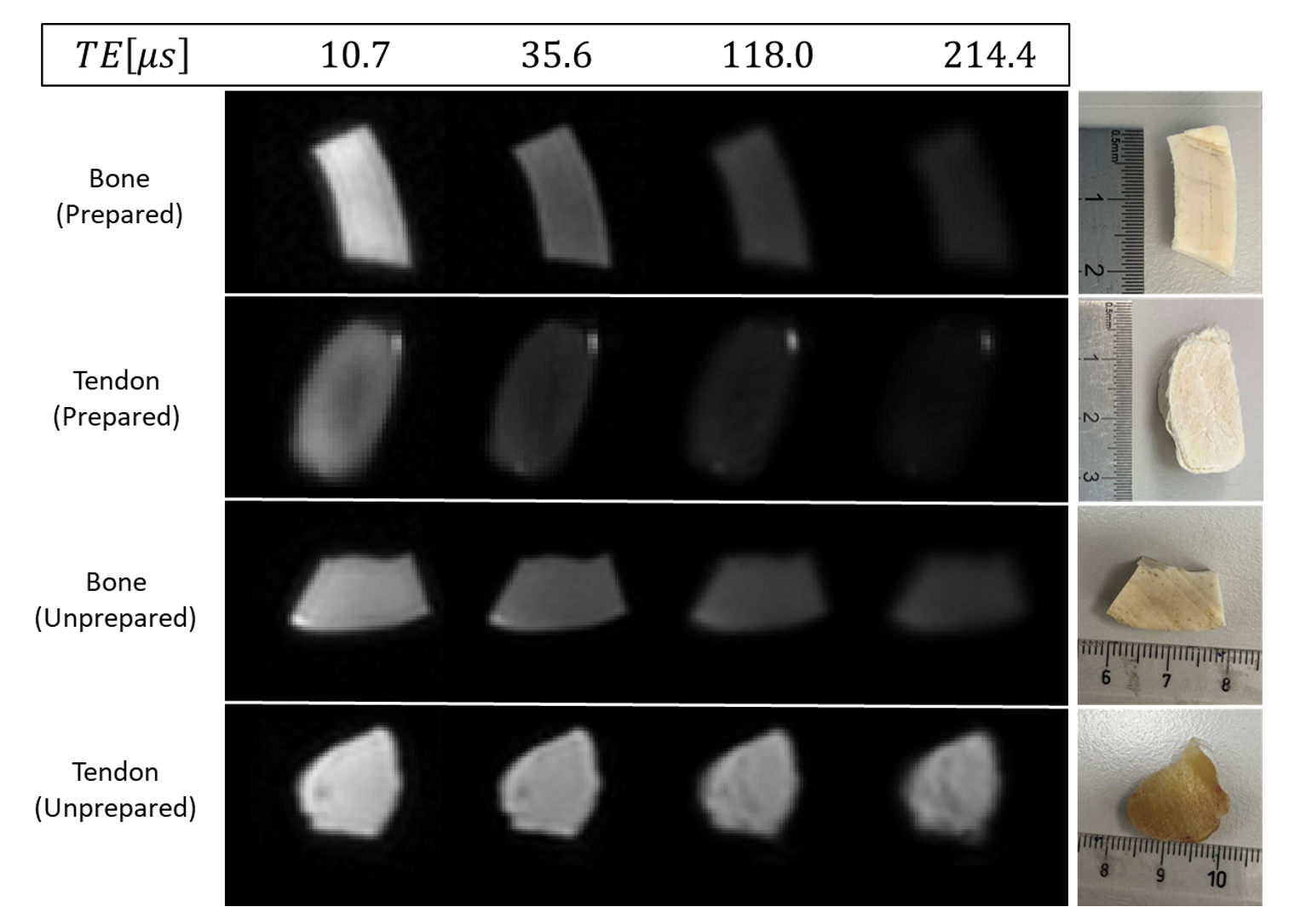
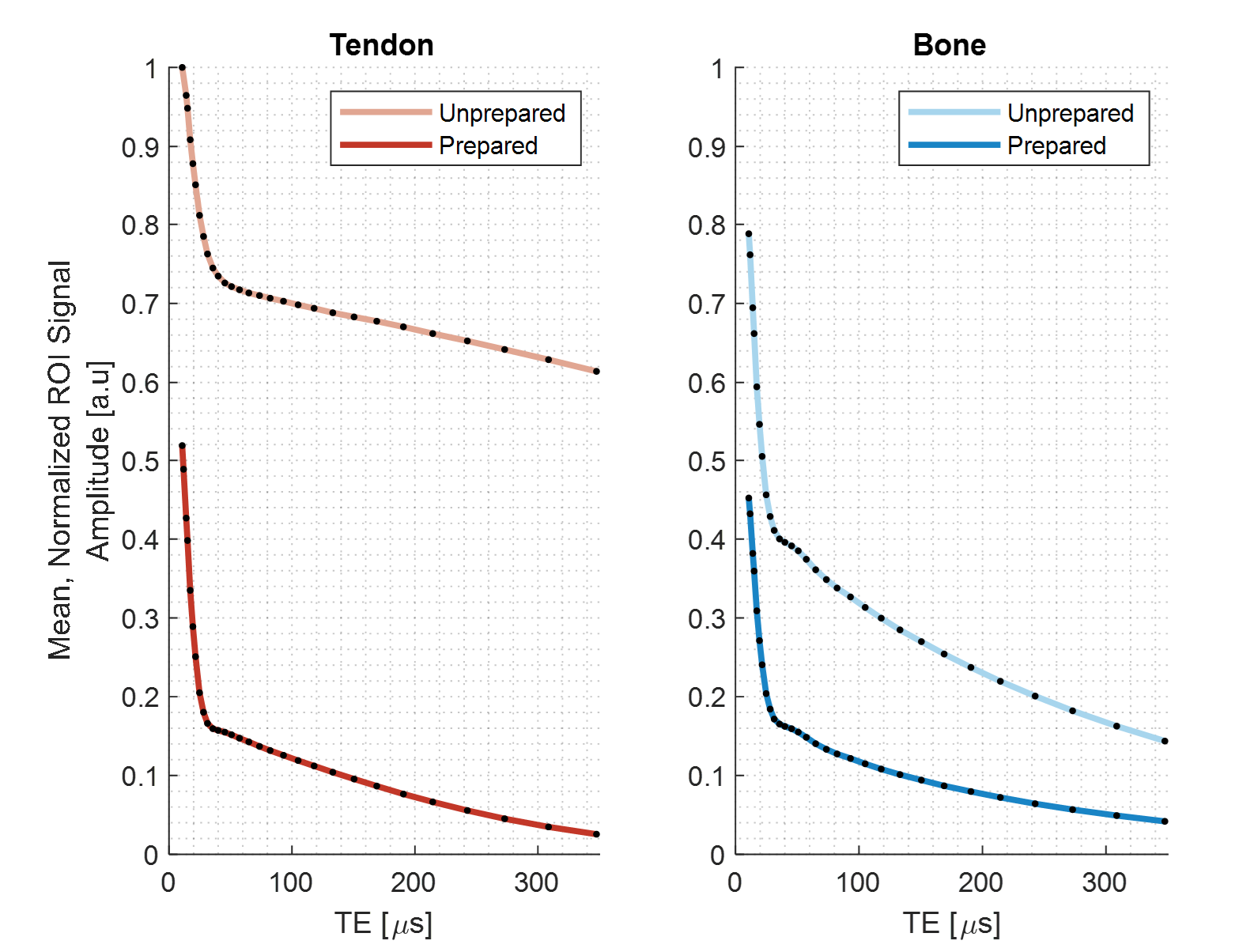
Figure 2 demonstrates that imaging of collagen was successfully performed with high SNR and reasonable resolution. The images of selected TEs convey rapidly decaying signals in the collagen-rich specimens. Figure 3 shows the full decay curves obtained in a region of interest for all TEs. A T2 on the order of 10µs is observed, which is attributed primarily to the collagen constituent. Figure 4 shows the results of performing image subtraction with different echo times leaving an image of only short-lived signal components. Figure 5 demonstrates an in-vivo application, providing a subtraction image conveying the collagen content.Discussion
This work demonstrates successful direct MR imaging of collagen. Moreover, spatially resolved observation of the rapid signal decay was enabled. Direct collagen MRI was achieved by employing hardware which allows for echo and encoding times short enough to capture and localize the elusive collagen signal. However, the effective resolution of the collagen images is still limited by the gradient hardware as even at the highest bandwidth, considerable T2 blurring is observed. Additionally, the short-lived signals constitute not only collagen, but also short-lived components from other macromolecules [22]. Nevertheless, the possibility of direct collagen imaging has been established opening avenues to explore potential clinical applications of the method and comparison with existing collagen imaging approaches.Acknowledgements
No acknowledgement found.References
[1] B. Yue, "Biology of the Extracellular Matrix: An Overview," Glaucoma, pp. S20-S23, 2014.
[2] A. Cieza, K. Causey, K. Kamenov, S. Hanson, S. Chatterji and T. Vos, "Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019," The Lancet, vol. 396, no. 10267, pp. 2006-2017, 2020.
[3] C. Frantz, K. Stewart and V. Weaver, "The extracellular matrix at a glance," Journal of Cell Science, vol. 123, no. 24, pp. 4195-4200, 2010.
[4] R. Horch, J. Nyman, D. Gochberg, R. Dortch and M. Does, "Characterization of 1H NMR Signal in Human Cortical Bone for Magnetic Resonance Imaging," Magnetic Resonance in Medicine, vol. 64, no. 3, pp. 680-7, 2010.
[5] H. Berendson, " Nuclear Magnetic Resonance Study of Collagen Hydration," J. Chem. Phys. , vol. 36, pp. 3297-3305, 1962.
[6] P. Fantazzini, R. Brown and G. Borgia, "Bone tissue and porous media: common features and differences studied by NMR relaxation.," Magn Reson Imaging, vol. 21, no. 3-4, pp. 227-34, 2003.
[7] L. Schreiner, I. Cameron, N. Funduk, L. Miljković, M. Pintar and D. Kydon, "Proton NMR spin grouping and exchange in dentin," Biophys J., vol. 59, no. 3, pp. 629-39, 1991.
[8] F. Wehrli, "Magnetic resonance of calcified tissues," J Magn Reson., vol. 229', pp. 35-48, 2013.
[9] G. Gold, "MR Spectroscopic imaging of collagen - tendons and knee menisci," Magnetic Resonance in Medicine, vol. 34, no. 5, pp. 647-54, 1995.
[10] S. Jerban, Y. Ma, L. Li, H. J. Jang, L. Wan, T. Guo, A. Searleman, E. Chang and J. Du, "Volumetric mapping of bound and pore water as well as collagen protons in cortical bone using 3D ultrashort echo time cones MR imaging techniques," Bone, vol. 127, pp. 120-8, 2019.
[11] J. Chen, S. Grogan, H. Shao, D. D'Lima, G. Bydder, Z. Wu and J. Du, "Evaluation of bound and pore water in cortical bone using ultrashort-TE MRI," NMR in Biomedicine, vol. 28, no. 12, pp. 1754-1762, 2015.
[12] S. Jerban, Y. Ma, B. Namiranian, A. Ashir, H. Shirazian, Z. Wei, N. Le, M. Wu, Z. Cai, J. Du and E. Chang, "Age-related decrease in collagen proton fraction in tibial tendons estimated by magnetization transfer modeling of ultrashort echo time magnetic resonance imaging (UTE-MRI)," Sci Rep, vol. 9, no. 17974, 2019.
[13] S. Jerban, Y. Ma, L. Wan, A. Searleman, H. Jang, R. Sah, E. Chang and J. Du, "Collagen proton fraction from ultrashort echo time magnetization transfer (UTE-MT) MRI modelling correlates significantly with cortical bone porosity measured with micro-computed tomography (μCT)," NMR Biomed, vol. 32, no. 2, 2019.
[14] Y. Ma, E. Chang, G. Bydder and J. Du, "Can ultrashort-TE (UTE) MRI sequences on a 3-T clinical scanner detect signal directly from collagen protons: freeze-dry and D2 O exchange studies of cortical bone and Achilles tendon specimens," NMR Biomed, vol. 29, no. 7, pp. 912-7, 2016.
[15] R. Froidevaux, M. Weiger, M. Rösler, D. Brunner, B. Dietrich, J. Rever and K. Pruessman, "High-resolution short-T2 MRI using a high-performance gradient," High-resolution short-T2 MRI using a high-performance gradient, vol. 84, no. 4, pp. 1933-46, 2020.
[16] M. Weiger, J. Overweg and M. e. a. Rösler, "A High-Performance Gradient Insert for Rapid and Short-T2 Imaging at Full Duty Cycle," Magn Reson Med, vol. 79, no. 6, pp. 3256-3266, 2018.
[17] S. C.M, W. M, R. Froidevaux and P. K.P, "Rapid high power transmit-receive switching using a timed cascade of PIN diodes," in ISMRM & SMRT Annual Meeting & Exhibition, 2021.
[18] D. Grodzki, P. Jakob and B. Heismann, "Ultrashort echo time imaging using pointwise encoding time reduction with radial acquisition (PETRA)," Magn Reson Med., vol. 67, no. 2, pp. 510-8, 2012.
[19] E. Baadsvik, M. Weiger, R. Froidevaux, C. Schildknecht, B. Ineichen and K. Pruessmann, "Mapping the myelin bilayer with short-T2 MRI: Translation to in vivo application," in ISMRM 2023.
[20] H. Lee, M. Weiger, C. Giehr, R. Froidevaux, D. Brunner, M. Rösler and K. Pruessmann, "Long-T2-suppressed zero echo time imaging with weighted echo subtraction and gradient error correction," Magnetic Resonance in Medicine, vol. 83, no. 2, pp. 412-426, 2019.
[21] E. S and J. Creyghton, "High resolution NMR imaging in solids," Physica B+C, vol. 128, no. 1, pp. 81-83, 1985.
[22] A. Seifert and F. Wehrli, "Solid-State Quantitative 1H and 31P MRI of Cortical Bone in Humans," Curr Osteoporos Rep., vol. 14, no. 3, pp. 77-86, 2016.
Figures