0485
Fast spin-echo triple-echo dixon (fTED) for fat suppression at 0.5T in the presence on knee implant.1GE HealthCare, Bangalore, India, 2Narula Diagnostics, Rohtak, India, 3Manipal Hospital, Bangalore, India
Synopsis
Keywords: Whole Joint, Low-Field MRI
Motivation: Fat saturation in musculoskeletal MRI at 0.5T in the presence of knee implants.
Goal(s): Echo spacing requirement of Fast spin-echo triple-echo Dixon (fTED) renders it as a preferred option for fat suppression even in the presence of implants without significant scan time penalty.
Approach: Commercially available fTED MRI was used to acquire 3 echoes (intra echo spacing of 6.71msec) between two consecutive refocusing pulses of FSE data acquisition at 0.5T research MRI system.
Results: Good quality fat suppression was observed in PD fat saturation knee MRI over 3 patients with knee implants.
Impact: Low and mid field MRI can benefit from fTED algorithm for fat suppression where water and fat are resonating in close proximity (in Hz) of each other without significant scan time penalty.
INTRODUCTION
MR Imaging of knee joint is a non-invasive tool for the evaluation of disorders such as meniscal, ligamental, soft tissue, bone and bone marrow injuries and abnormalities.[1]. Its effectiveness can be challenging when imaging patients with knee implants because of susceptibility induced artifacts near the metal implants. Mid-Field MRI at 0.5T has been shown to generate good quality MR Images compared to 1.5T and 3.0T due to lower susceptibility induced field inhomogeneity. PD-Fat-Sat is essential sequence of Knee MRI and fat saturation can be challenging at 0.5T as water and fat are resonating in proximity of each other (74Hz) requiring long CHESS pulse and any field inhomogeneity near the implant can yield in-appropriate fat saturation [2]. Dixon based fat separation/suppression techniques are robust to B0 inhomogeneity, however they are associated with 2- or 3-fold increase in scan time [3]. In order to overcome this issue, fast spin-echo triple-echo Dixon (fTED) had been proposed to acquire multiple shifted echoes required for Dixon processing between each refocusing pulse of FSE data acquisition [4]. The echo spacing requirement for 180 phase shift among echoes leads to very aggressive receiver bandwidth at 1.5T and 3.0T MRI leading to lower SNR and limiting the clinical use of fTED. In this abstract, we accessed knee joint imaging of patients with implants at 0.5T using fTED technique due to relaxed echo spacing requirement (6.71msec) to generate proton density images with and without fat suppression.METHOD
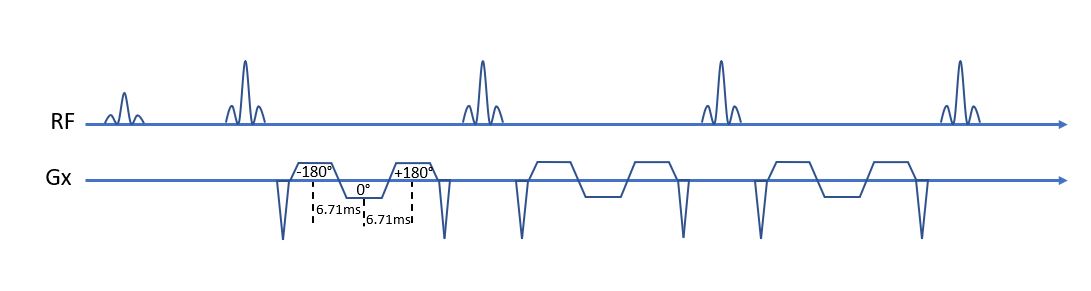
fTED at 0.5T: fTED acquires three-time shifted echoes between two consecutive refocusing pulse of the FSE data acquisition as shown in Figure 1. These echoes are time shifted so that fat can accumulate 180° of phase relative to water in first and third echo. At 0.5T this amounts to 6.71msec echo spacing between neighboring echoes.Imaging System: Research MRI system comprising of commercial 1.5T Signa Creator (GE HealthCare, Milwaukee, WI, USA) ramped down to 0.5T, with modifications made to the RF transmit and receive chain was used for data acquisition. One panel (out of two) of 16 Channel multi-purpose flexible coil was wrapped around the affected knee joint of the patient to acquire data from 8 channels.
Data Acquisition: Patients with knee joint implant referred for knee MR Imaging at 1.5T scanner at the diagnostic center was given an option to participate in the IRB approved study at 0.5T. 3 consecutive patients participated in this study with informed consent. Proton density fTED was acquired in all three planes (FOV=18cm, Matrix Size: 320x224, TR/TE=1674/28.1, rBW= 22.7kHz, slice thickness/spacing=5mm/1.5mm) in 4:15 minutes.
RESULTS
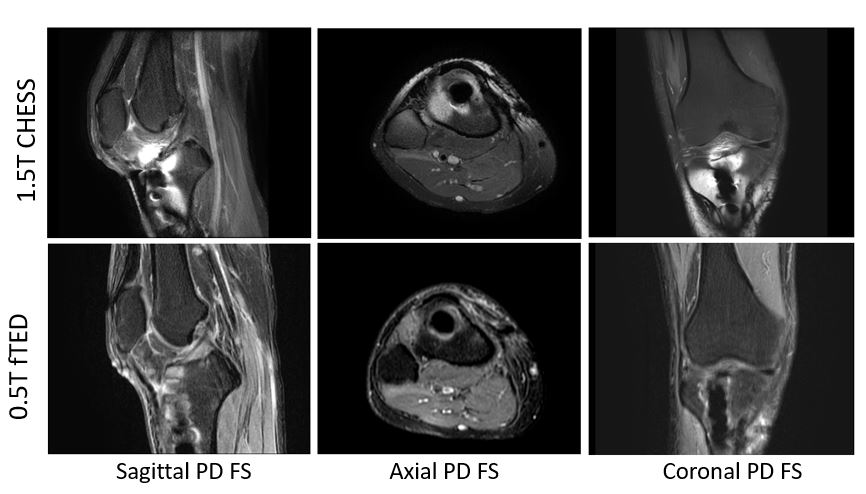
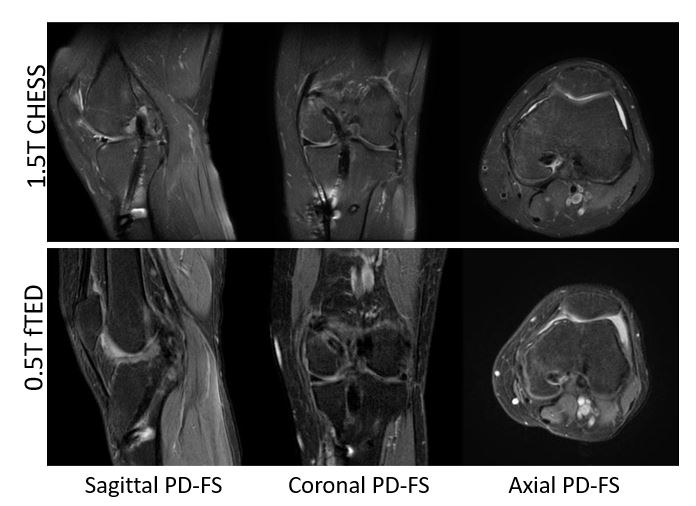
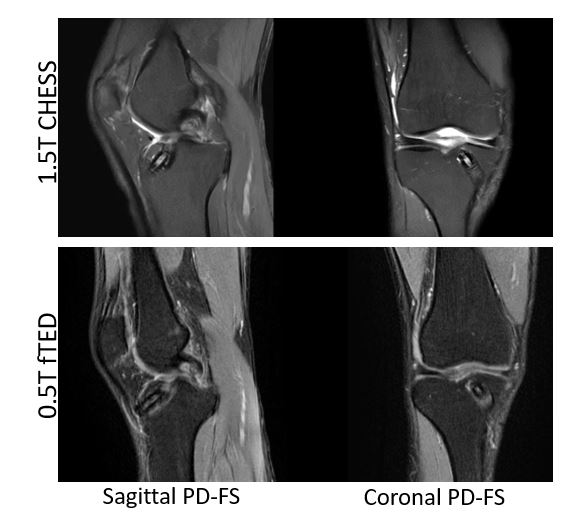
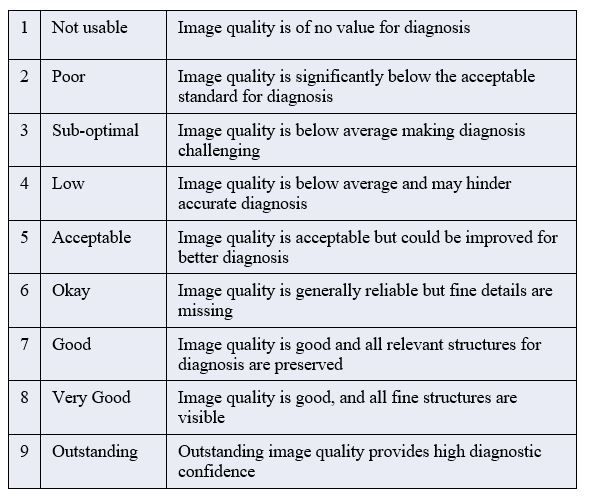
Figure 2-4 show proton density images with fat suppression using CHESS method at 1.5T clinical scanner in comparison with fTED proton density weighted imaging acquired using 0.5T for the three patients. Susceptibility artifacts from implants caused inadequate fat sat with CHESS method at 1.5T. fTED showed less artifacts and improved fat suppression at 0.5T. These images were rated based on a Likert scale (Table1) by a senior radiologist with more than 30 years of experience. fTED images from 0.5T were rated 7 indicating all the relevant structured for diagnosis can be accessed for all three patient’s data.DISCUSSION AND CONCLUSION
fTED had been developed and commercialized by various vendors for scan time efficient fat suppression/separation. However, its clinical uptake is limited due to the high receiver bandwidth requirement at typical 1.5T and 3.0T. In this abstract we have demonstrated that the receiver bandwidth requirement at 0.5T for fTED can be utilized to acquire scan time efficient data acquisition for Dixon based fat separation/suppression. The robust fat suppression of fTED was demonstrated to acquire an essential PD-FS contrast in knee MRI even in the presence of the metal implants. When compared to 1.5T, fTED at 0.5T was shown to be diagnostically useful with uniform fat suppression and less artifacts near the metal implants. Further research is warranted to explore the use of fTED MRI for fat separation/suppression in various anatomies and various use case due to the longer echo spacing requirement of fTED MRI among neighboring echoes at 0.5T.Acknowledgements
No acknowledgement found.References
- ACR–SPR–SSR practice parameter for the performance and interpretation of magnetic resonance imaging (MRI) of the Knee.Res 6-2015
- Farahani K, Sinha U, Sinha S, Chiu LC, Lufkin RB. Effect of field strength on susceptibility artifacts in magnetic resonance imaging. Comput Med Imaging Graph. 1990 Nov-Dec;14(6):409-13. doi: 10.1016/0895-6111(90)90040
- Hu, H.H., Börnert, P., Hernando, D., Kellman, P., Ma, J., Reeder, S. and Sirlin, C., 2012. ISMRM workshop on fat–water separation: insights, applications and progress in MRI. Magnetic resonance in medicine, 68(2), pp.378-388.
- Ma J, Son JB, Zhou Y, Le-Petross H, Choi H. Fast spin-echo triple-echo dixon (fTED) technique for efficient T2-weighted water and fat imaging. Magn Reson Med. 2007 Jul;58(1):103-109. doi: 10.1002/mrm.21268.
Figures