0483
Advances in Musculoskeletal Imaging: The Potential of Wireless Metasurface Coils.1Institute of Diagnostics and Interventional Radiology, Hannover, Germany, 2Research Campus STIMULATE, Otto-von-Guericke University, Magdeburg, Germany, 3Chair of Microwave and Communication Engineering, Otto-von-Guericke University, Magdeburg, Germany, 4Biomedical Magnetic Resonance, Otto-von-Guericke University, Magdeburg, Germany
Synopsis
Keywords: Other Musculoskeletal, MSK
Motivation: Musculoskeletal imaging (MSK) traditionally employs specific coil designs for distinct anatomical areas. Metasurface coils (MC) are innovative, light-weighted, and wireless coils promising for MSK imaging.
Goal(s): Primary objective of the MC was similar image quality but better patient comfort compared to standard coils.
Approach: Signal-to-noise ratios (SNRs) in elbow, knee, foot and hand imaging of conventional coils were compared with the MC.
Results: The MC showed improvement in SNR values for hand and foot. Imaging of knee and elbow was improved as well, but with less SNR near the spine coil. The MC's design streamlined positioning, maneuverability and can improve patient comfort.
Impact: Metasurface coils promise transformative benefits for future musculoskeletal imaging, matching the image quality of standard coils with increased flexibility and patient comfort. Their versatility allows compatibility across MRI vendors, only depending on the field strength of the designated coil.
Introduction
Musculoskeletal (MSK) imaging plays a pivotal role in everyday clinical practice. However, current techniques are often constrained by specialized coil designs, which are optimized for one anatomical region and field strength, respectively. Consequently, due to economic considerations, clinicians sometimes improvise with suboptimal setups — like using a head/neck coil for foot imaging. The introduction of Metasurface coils (MC) offers a promising solution. These coils are known for their ultra-lightweight, flexible designs and the capability for wireless imaging [1]. This study aims to compare the performance of a MC with conventional coil setups commonly found in clinical settings for MSK applications at 1.5 Tesla (T).Methods
One healthy volunteer gave informed consent to participate in this review after IRB approval (No. 11019_B0_S_2023). All scans were performed at a 1.5T MRI (Aera, Siemens Healthineers, Germany).Metasurface coil:
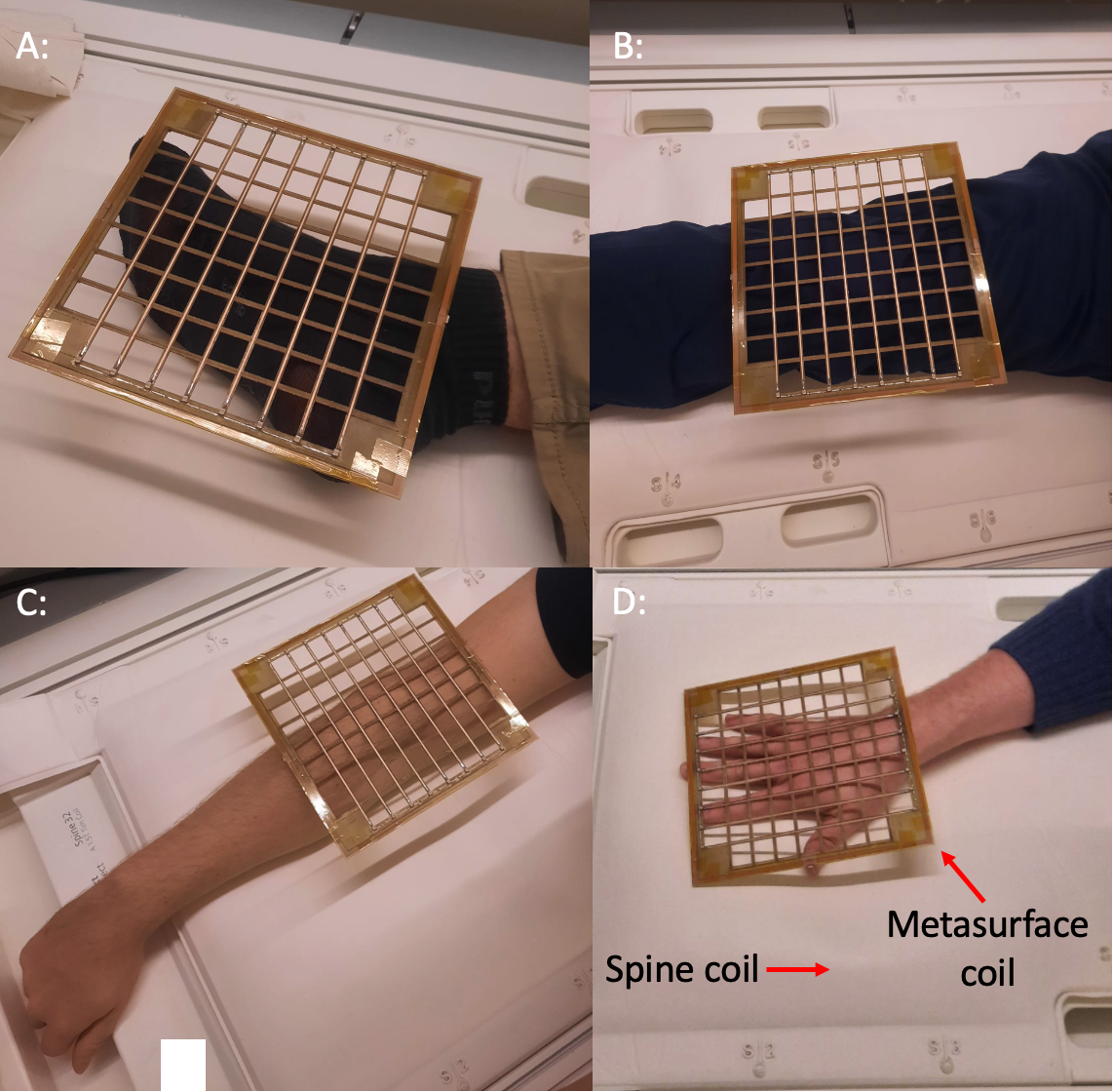
A MC (19x19 cm) with an 8x8 grid of resonant unit cells tuned to the Larmor frequency of ~64 MHz was used (Preview Figure).
Positioning:
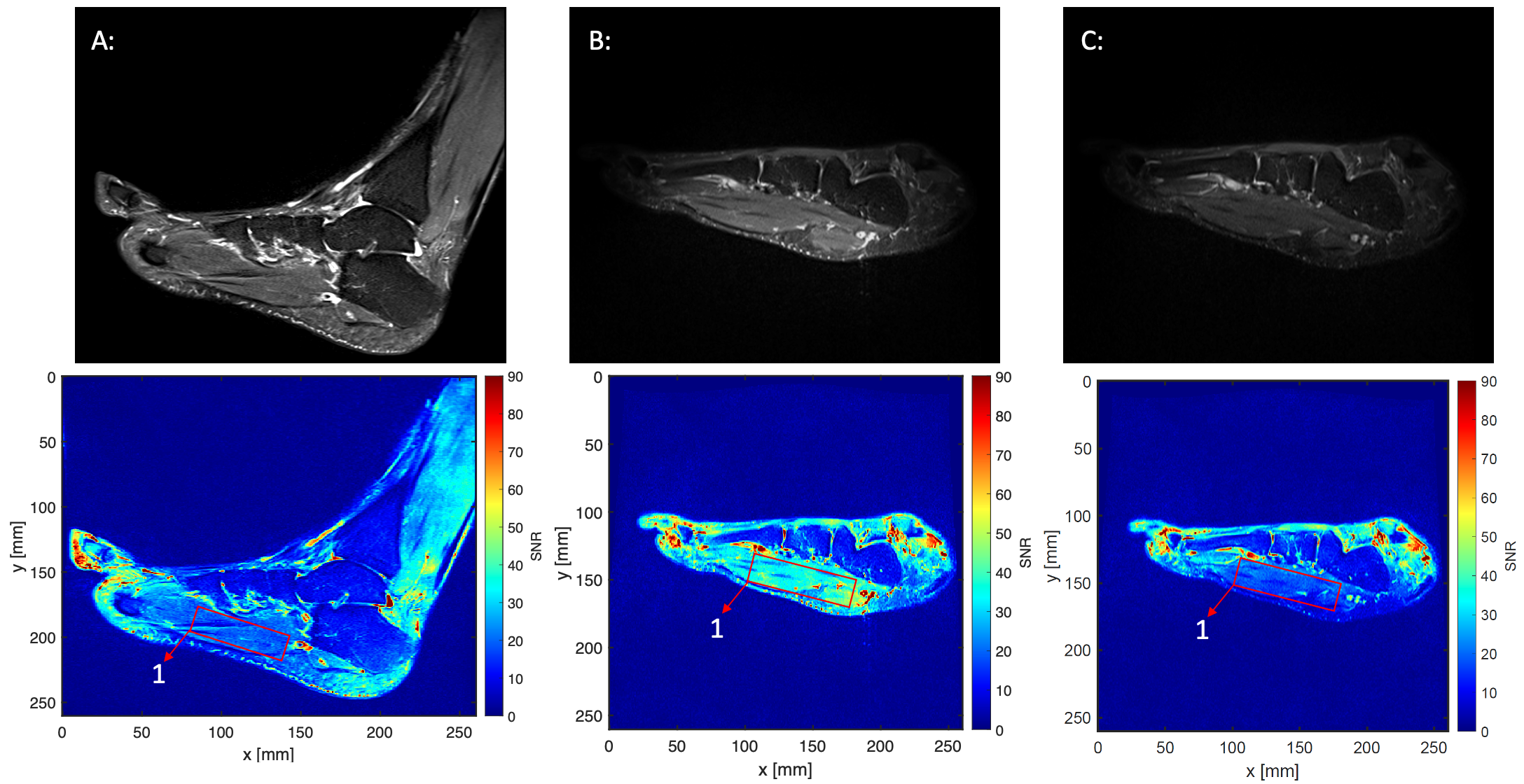
The MC was used in conjunction with the table-integrated spine coil (Spine 32, Siemens Healthineers, Germany) for imaging elbow, knee, foot, and hand (Figure 1). All scans were then repeated with the spine coil only. A clinical setup with state-of-the-art coils was also performed: for elbow and hand a multipurpose coil (Flex Large 4, Siemens Healthineers, Germany) was used with the volunteer in superman position, for the knee a dedicated knee coil (Tx/Rx 15-Channel Knee Coil, Siemens Healthineers, Germany), and for the foot a head coil (Head/Neck 20, Siemens Healthineers, Germany) was used with the volunteer in supine position. The positioning was consistent between all setups, except for the foot, in which a slight outward rotation was introduced when using the spine coil with/without the MC.
Data Collection and Analysis:
The following scan parameters were used for all three setups:
- Elbow: PD TSE fs ax (TR 3310ms, TE 39ms, slice thickness 3mm, matrix 300x384)
- Hand: PD TSE fs sag (TR 3530ms, TE 37ms, slice thickness 2mm, matrix 384x312, R=2)
- Knee: PD TSE fs ax (TR 3110ms, TE 21ms, slice thickness 3mm, matrix 448x448)
- Foot: T2 TIRM sag (TR 5110ms, TE 28ms, slice thickness 2mm, matrix 384x384, R=2)
For the knee scan, imaging with the spine coil with/without the MC was oversampled by 150% to prevent wrap around artifacts. To compensate for the resulting signal-to-noise ratio (SNR) increase, the SNR for the state-of-the-art setup was adjusted by a factor of 1.58. SNR maps were generated based on local noise estimations from a noise-only acquisition for each setup and evaluated at dedicated regions of interest.
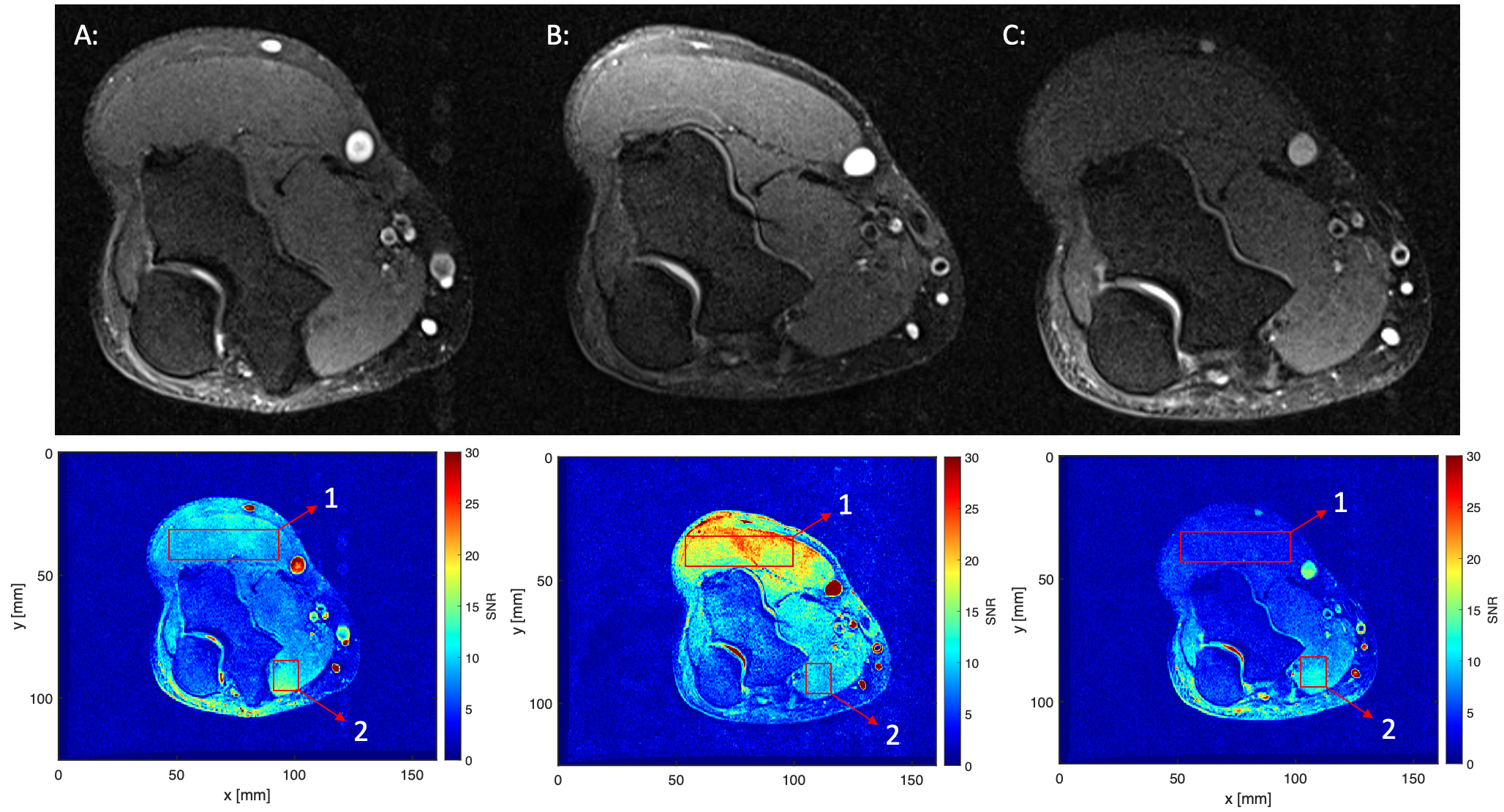
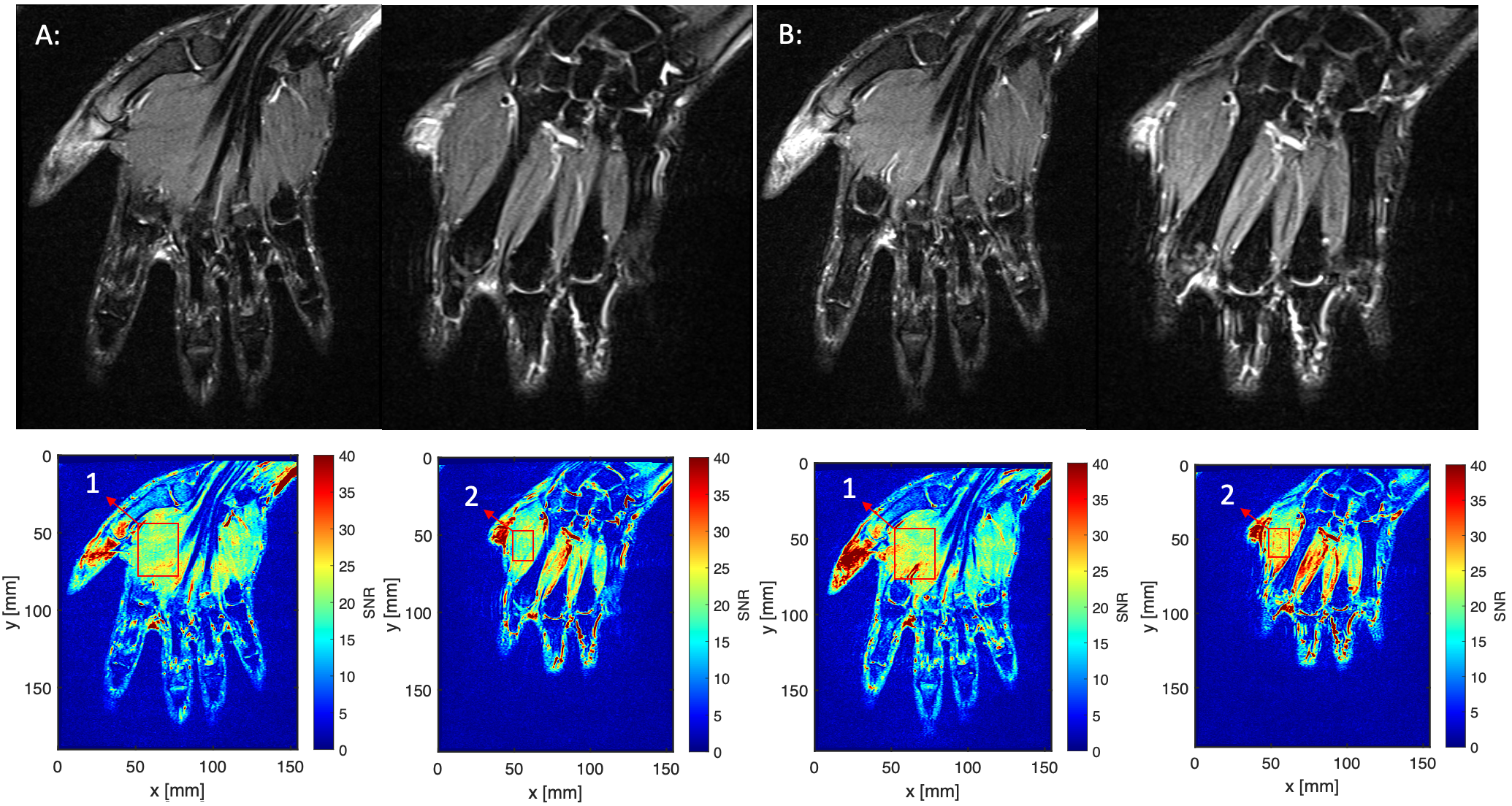
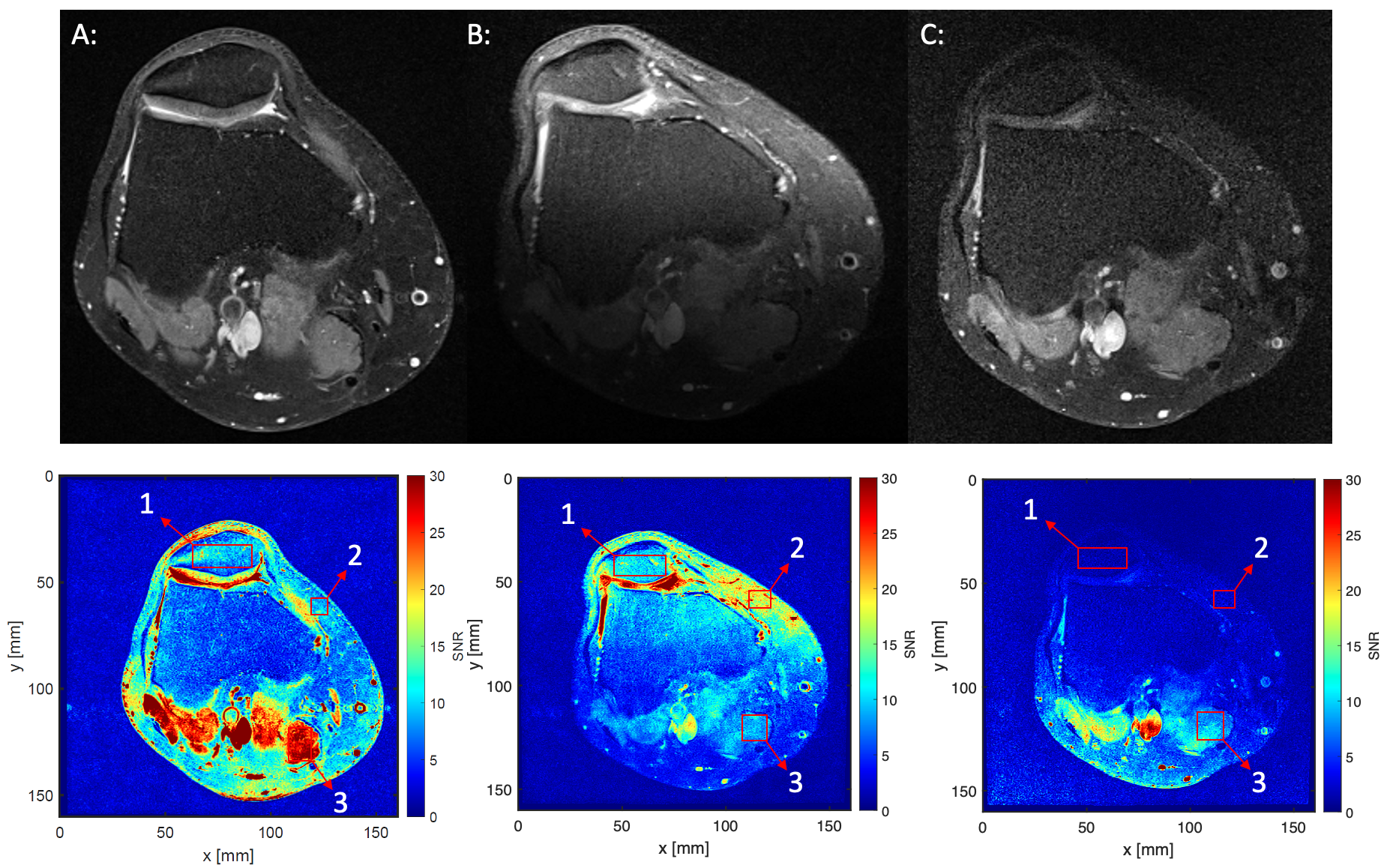
Results
Positioning with the MC was straightforward and fast. Imaging results of all anatomical regions and corresponding SNR-maps are shown in Figure 2-5. The MC resulted in higher or equal SNR across the entire image of the hand and foot compared to the state-of-the-art setup. In the hand scan the SNR in the evaluated regions of interest (ROI) were 11 or 24% higher, and in the foot scan 93% higher than with the state-of-the-art setup, respectively. In the knee and elbow scans, SNR values were comparable to the state-of-the-art setup with a coverage of 6.7cm and 6.4cm in depth (approximately 77% and 52% of the anatomy), respectively. Close to the MC, SNR differences were 102% (ROI1) and 90% (ROI2) higher for elbow and knee, respectively. Less SNR was seen posterior near the spine coil.Discussion
MCs modulate the sensitivity of other coils and consecutively allow extended coverage and enhanced SNR [2, 3]. A notable advancement of MCs is the potential for wireless imaging by combining them with scanner-integrated MR-coils (e.g. spine coil). Future dedicated MC designs may achieve further depth. Although SNR with the MC was increased in many examined regions, further sequence adaptation might be necessary to counteract inhomogeneous illumination, e.g. by normalization.Primary limitation of this study is the small sample size, which restricts the generalizability of our findings and will be addressed by future evaluations. Moreover, the MC's generic design was not tailored to specific anatomical regions yet, which changed the positioning of the foot scan compared to the standard setup. This underestimates potential benefits of region-specific design optimizations of MCs regarding imaging quality. SNR maps were adapted for the knee by assuming the relative SNR change at the MRI.Conclusion
MCs exhibit great potential for MSK imaging in the studied anatomical regions. More extensive research is needed for a comprehensive evaluation, which may include larger regions like hip and shoulder.Acknowledgements
This work was funded by the Federal Ministry of Education and Research within the Research Campus STIMULATE under the number ‘13GW0473A’ and ‘13GW0473B’.References
[1] R. Kowal et al., “Metamaterial Inspired Surface Resonators as Wireless Coil”. In: Proceedings of the 13th Interventional MRI Symposium, p. 106 (2022), Leipzig.
[2] Freire et al., “Experimental demonstration of a μ=−1 metamaterial lens for magnetic resonance imaging”. Applied Physics Letters. 2008. 93. 10.1063/1.3043725.
[3] Schmidt et al., “Flexible and compact hybrid metasurfaces for enhanced ultra high field in vivo magnetic resonance imaging”, Scientific Reports 2017.
Figures