0470
Tissue detail of pregnant body models needed to estimate SAR for fetal MRI1Fetal-Neonatal Neuroimaging Developmental Science Center, Boston Children's Hospital, Boston, MA, United States, 2Harvard Medical School, Boston, MA, United States, 3Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Keywords: Safety, Fetus, Electromagnetic simulations
Motivation: Due to the large variation of the body shape and size in the pregnant population, several pregnant body models are needed in fetal MRI safety studies. However, creating detailed pregnant body models is challenging.
Goal(s): Our goal is to investigate the effect of reducing maternal tissue detail on maternal and fetal SAR.
Approach: We simplified >18 maternal tissues into 3 (muscle, lung and fat) in 7 pregnant body models and quantified the change in maternal and fetal SAR.
Results: The value and location of maternal and fetal SAR changes by up to 13% and 34 mm with maternal tissue detail reduction.
Impact: Simplification of maternal tissues into muscle, lung and fat changes maternal and fetal SAR (<14%) significantly less than the variation of SAR between pregnant subjects (>x2) and might provide a good trade-off between accuracy and practicality in RF safety studies.
Introduction
RF safety of fetal MRI is understudied.1,2 One of the main reasons for this is the difficulty of creating realistic numerical pregnant body models. Fetal and maternal motion as well as maternal comfort makes it challenging to collect high quality data for body model generation. In addition, to the best of our knowledge, there are no automatic segmentation algorithms for pregnant abdomens and manual segmentation is time consuming. For these reasons, most of the previous RF safety studies for fetal MRI used artificially generated body models.3–9 A few studies used body models generated from MRI or CT data of pregnant women10,11, however they only used one model. We previously created 5 body models from MRI data of 4 pregnant women, with 19-20 maternal tissues and 6 uterine tissues and found more than a factor of 2 variation in the simulated fetal and maternal specific absorption rate (SAR) values.12 Although these models had different maternal positions, BMIs, and gestational ages; many more models are needed to sufficiently represent the pregnant population in RF safety studies. The number of tissues needed for accurate SAR estimations have been investigated for body13 and head imaging14,15 to be able to generate body models faster. Homann et al. simplified a male and a nonpregnant female body model with 36 and 33 tissues into 3 (muscle, lung and fat) and found <8% difference in the resulting SAR values for 3T body imaging.13 In this study, we investigate the impact of maternal tissue detail on the resulting maternal and fetal SAR values at 3T.Methods
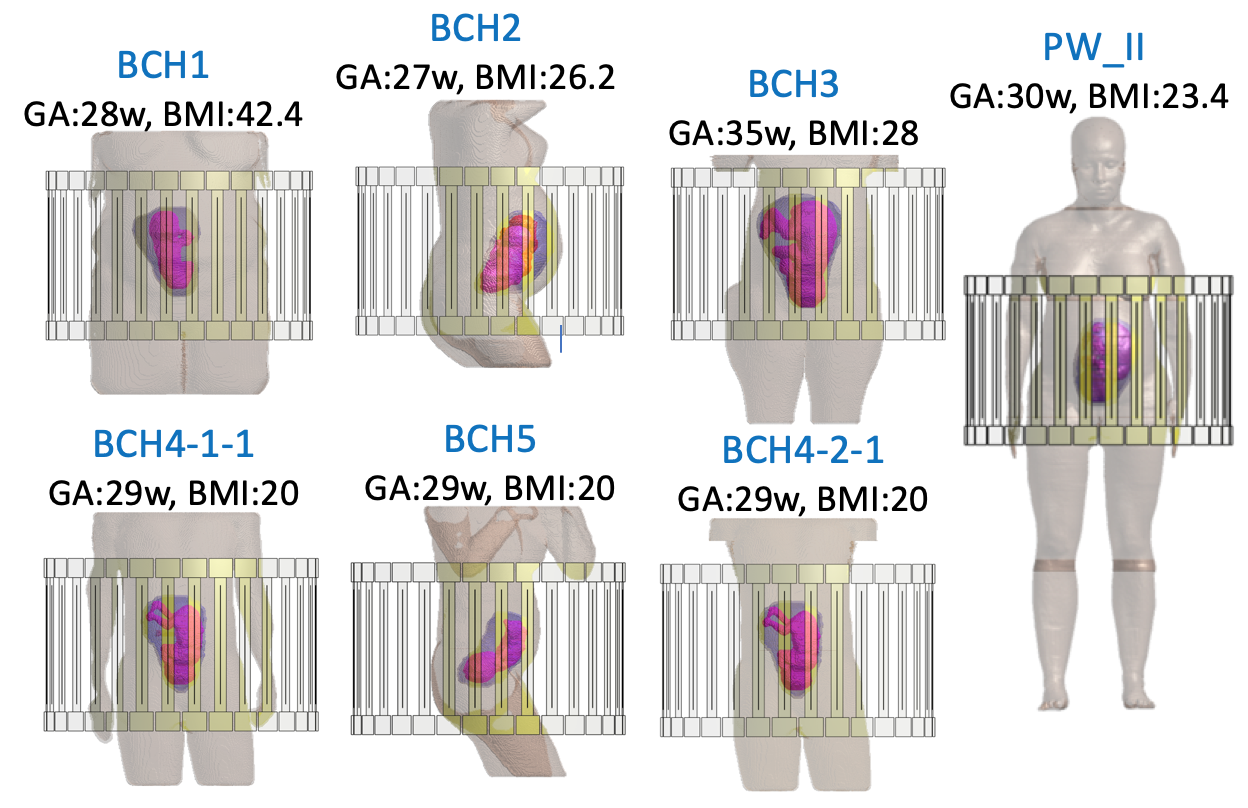
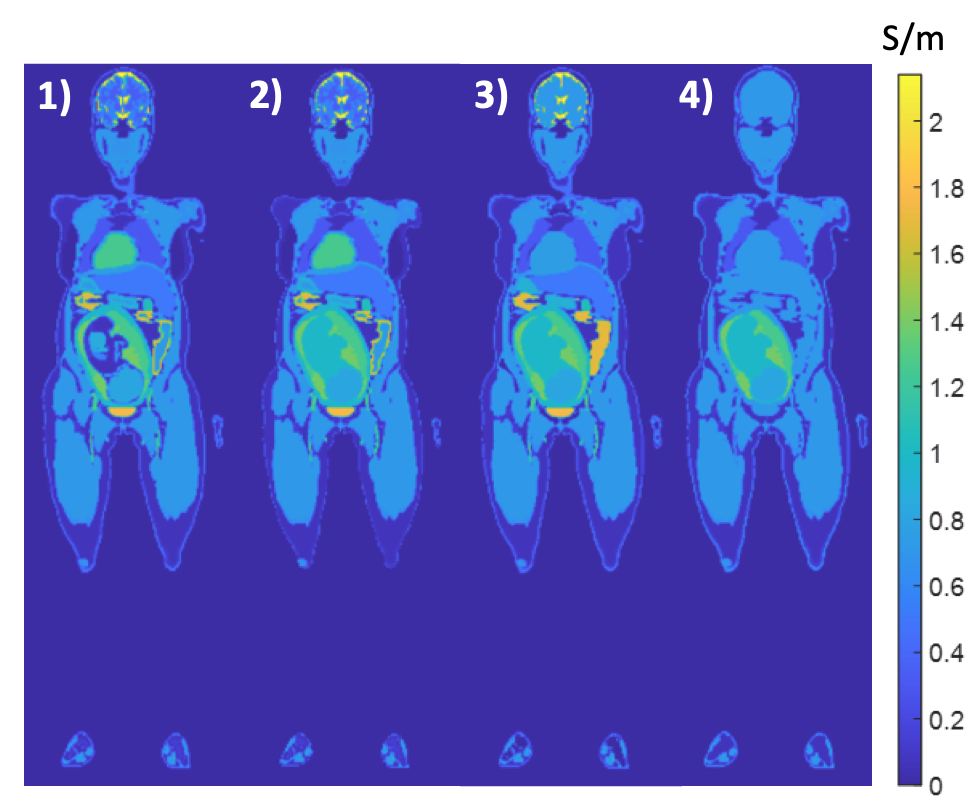
We utilized 6 previously described pregnant body models,12 with 19-20 maternal tissues, and 6 uterine tissues (uterus, placenta, amniotic fluid, umbilical cord, fetus and fetal brain). We simplified maternal tissues of each model into muscle, lung and fat. These body models were loaded into a 2-port 32-rung high-pass birdcage body coil tuned to 128 MHz (Fig.1). Electromagnetic and thermal simulations were carried out using Sim4Life (Zurich MedTech, Zurich, Switzerland). Tissue dielectric properties were assigned according to the IT’IS database16 except fetal tissues10 and amniotic fluid.17 In addition, we simplified a commercial, artificially generated pregnant body model from the IT’IS foundation (Zurich, Switzerland), called in short PW_II, with >45 maternal tissues into first, 20 maternal tissues, and then to muscle, lung and fat (Fig.2). We also simplified the 17 fetal tissues of PW_II, into fetal brain and remaining fetal body for comparability with the in-house models. We calculated maternal and fetal 10g-averaged peak local SAR (pSAR10g) and fetal average SAR (aveSAR) normalized to 2 W/kg maternal whole-body averaged SAR (wbSAR) for all models.Results
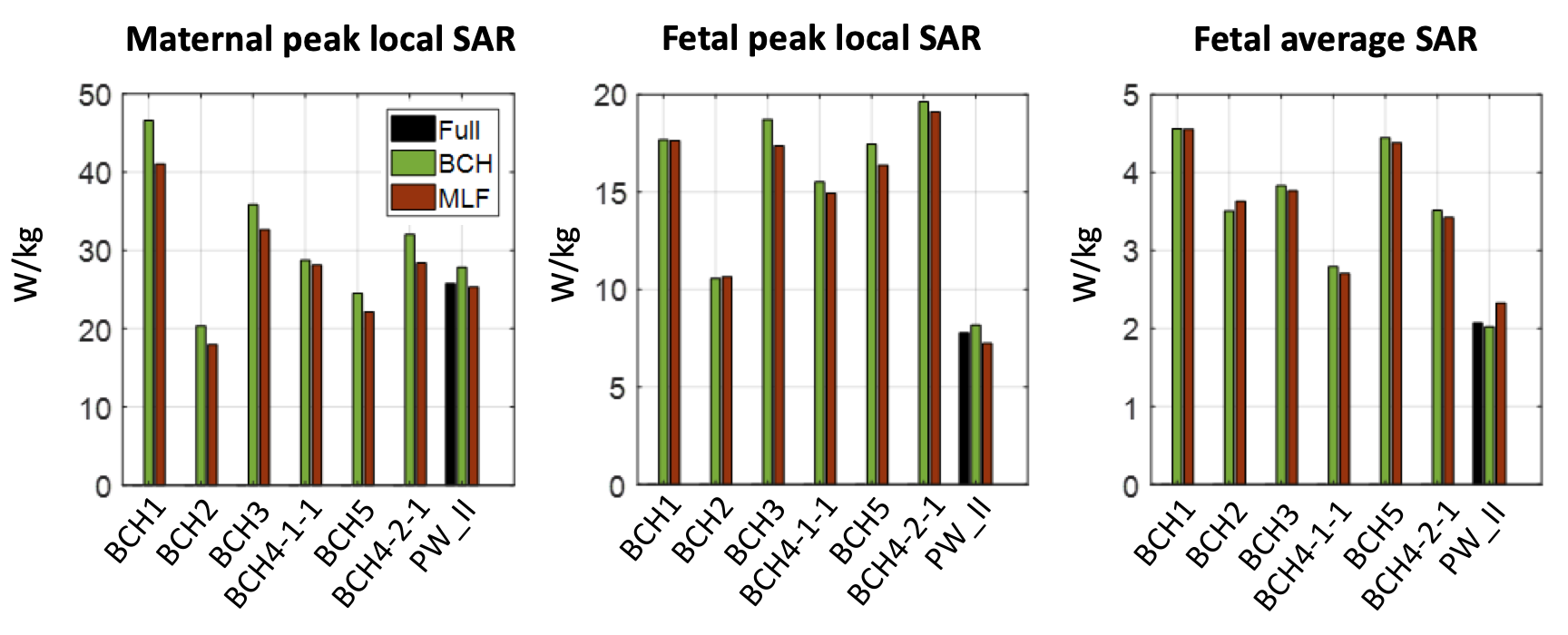
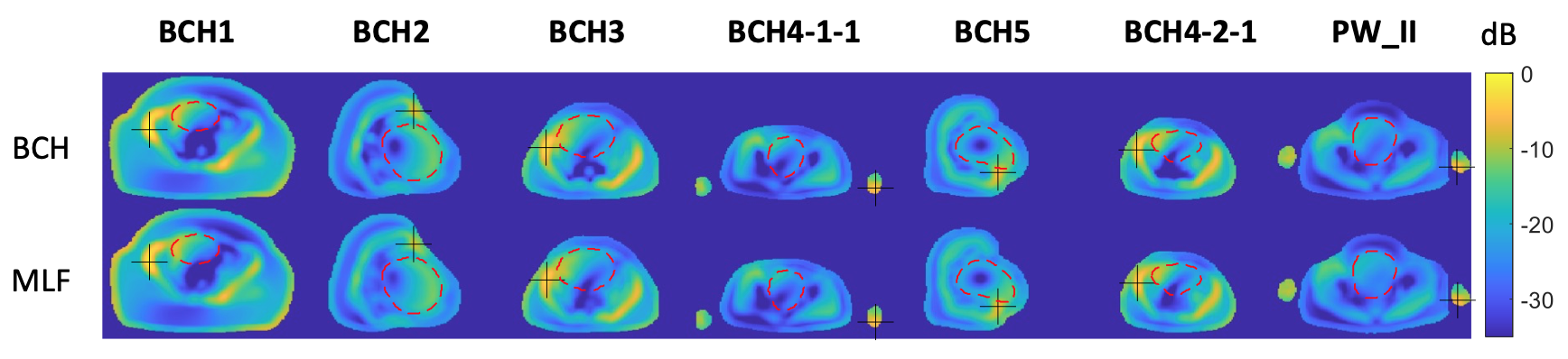
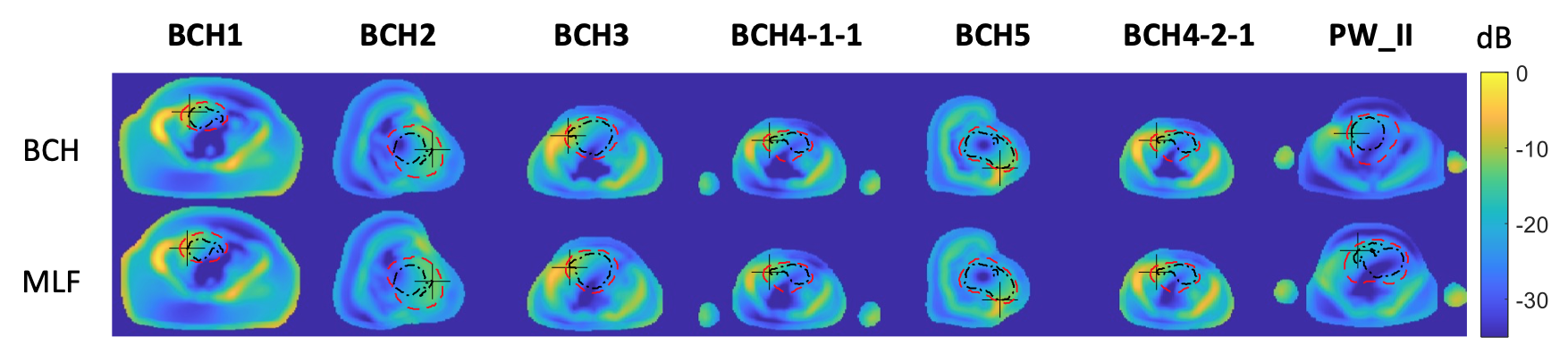
For PW_II, maternal pSAR10g and fetal pSAR10g increased by 8% and 5% and fetal aveSAR decreased by 2% when maternal tissues were reduced from >45 to 20. Maternal pSAR10g and fetal pSAR10g decreased by 2% and 7% and fetal aveSAR increased by 13% when maternal tissues were reduced from >45 to muscle, lung and fat (Fig.3). For BCH models, simplifying maternal tissues into muscle, lung and fat changed maternal pSAR10g by -2% to -12%, fetal pSAR10g by -6% to 1% and fetal aveSAR by -3% to 4% (Fig.3). The location of maternal pSAR10g did not change significantly (<5 mm) with the change in maternal tissue detail (Fig.4). The location of fetal pSAR10g changed by <15 mm when maternal tissues are simplified from 20 tissues into muscle, lung and fat for BCH models, and it changed by 34 mm for PW_II (Fig.5). Although fetal pSAR10g seems to move considerably in PW_II with tissue detail reduction, between the two locations that are 34 mm apart, the fetal SAR values in the muscle-lung-fat version of PW_II differ by only 2%. Finally, simplifying >45 maternal tissues into 20 for PW_II did not change the maternal or fetal pSAR10g location.Discussion and Conclusion
We simplified detailed pregnant body models with >18 maternal tissues into those with 3 maternal tissues (muscle, lung and fat). This simplification changed the maternal and fetal SAR values by up to 13%. In comparison to the large variation of maternal and fetal SAR in the pregnant population (by more than a factor of 2), the change in maternal and fetal SAR due to tissue detail reduction is relatively small. Considering the need to generate several pregnant body models to sufficiently represent the pregnant population in safety studies and the difficulty of generating detailed pregnant body models, simplification of maternal tissues into muscle, lung and fat might be acceptable. Future work includes investigation of the effect of tissue detail in thermal simulations.Acknowledgements
This work was supported by R01HD100009 and R01EB032708.References
1. International Electrotechnical Commission. IEC 60601-2-33:2022 Medical electrical equipment-Particular requirements for the basic safety and essential performance of magnetic resonance equipment for medical diagnosis. https://webstore.iec.ch/publication/67211. Published 2022. Accessed September 29, 2022.
2. Mervak BM, Altun E, McGinty KA, Hyslop WB, Semelka RC, Burke LM. MRI in pregnancy: Indications and practical considerations. J Magn Reson Imaging. 2019;49(3):621-631. doi:10.1002/jmri.26317
3. Wu D, Shamsi S, Chen J, Kainz W. Evaluations of Specific Absorption Rate and Temperature Increase Within Pregnant Female Models in Magnetic Resonance Imaging Birdcage Coils. IEEE Trans Microw Theory Tech. 2006;54(12):4472-4478. doi:10.1109/TMTT.2006.884655
4. Saito K, Kikuchi S, Takahashi M, Ito K, Ikehira H. SAR distributions in the abdomen of a pregnant woman generated in a bird cage coil for the MRI system. In: Proceedings of 2006 First European Conference on Antennas and Propagation. ; 2006:1-4. doi:10.1109/EUCAP.2006.4584515
5. Hand JW, Li Y, Hajnal JV. Numerical study of RF exposure and the resulting temperature rise in the foetus during a magnetic resonance procedure. Phys Med Biol. 2010;55(4):913-930. doi:10.1088/0031-9155/55/4/001
6. Wang Z, Yeo D, Xu G, Jin J, Robb FJ. SAR Evaluation of Whole-body Pregnant Woman Models at Different Gestational Stage and Position in MRI Birdcage Coil. In: Proceedings of the 18th Annual Meeting of ISMRM. Stockholm, Sweden; 2010:3878.
7. Kikuchi S, Saito K, Takahashi M, Ito K. Temperature elevation in the fetus from electromagnetic exposure during magnetic resonance imaging. Phys Med Biol. 2010;55(8):2411-2426. doi:10.1088/0031-9155/55/8/018
8. Murbach M, Neufeld E, Samaras T, et al. Pregnant women models analyzed for RF exposure and temperature increase in 3T RF shimmed birdcages. Magn Reson Med. 2017;77(5):2048-2056. doi:10.1002/mrm.26268
9. Malik SJ, Hand JW, Hajnal JV. The effect of fetal dielectric properties, position and blood-flow in maternal tissues on fetal temperature for fetal MRI at 3T. In: Proceedings of the 26th Annual Meeting of ISMRM. Paris, France; 2018:1460. doi:10.13099/vip21000-03-0
10. Hand JW, Li Y, Thomas EL, Rutherford MA, Hajnal JV. Prediction of specific absorption rate in mother and fetus associated with MRI examinations during pregnancy. Magn Reson Med. 2006;55(4):883-893. doi:10.1002/mrm.20824
11. Pediaditis M, Leitgeb N, Cech R. RF-EMF exposure of fetus and mother during magnetic resonance imaging. Phys Med Biol. 2008;53(24):7187-7195. doi:10.1088/0031-9155/53/24/012
12. Abaci Turk E, Yetisir F, Adalsteinsson E, et al. Individual variation in simulated fetal SAR assessed in multiple body models. Magn Reson Med. 2020;83(4):1418-1428. doi:10.1002/mrm.28006
13. Homann H, Börnert P, Eggers H, Nehrke K, Dössel O, Graesslin I. Toward individualized SAR models and in vivo validation. Magn Reson Med. 2011;66(6):1767-1776. doi:10.1002/mrm.22948
14. Wolf S, Diehl D, Gebhardt M, Mallow J, Speck O. SAR simulations for high-field MRI: How much detail, effort, and accuracy is needed? Magn Reson Med. 2013;69(4):1157-1168. doi:10.1002/mrm.24329
15. Milshteyn E, Guryev G, Torrado‐Carvajal A, et al. Individualized SAR calculations using computer vision-based MR segmentation and a fast electromagnetic solver. Magn Reson Med. 2021;85(1):429-443. doi:https://doi.org/10.1002/mrm.28398
16. Hasgall P, Gennaro F, Baumgartner C, et al. “IT’IS Database for thermal and electromagnetic parameters of biological tissues” Version 4.1, Feb 22, 2022, DOI: 10.13099/VIP21000-04-1. itis.swiss/database.
17. Peyman A, Gabriel C. Dielectric properties of rat embryo and foetus as a function of gestation. Phys Med Biol. 2012;57(8):2103-2116. doi:10.1088/0031-9155/57/8/2103
Figures