0462
Enhanced Real-Time iCMR Device Visualization Using GRAPPA and DnCNN Denoising at Low Field1The Ohio State University, Columbus, OH, United States, 2Siemens Medical Solutions USA, Inc., Columbus, OH, United States, 3Siemens Healthcare, Erlangen, Germany, 4Nationwide Childrens Hospital, Columbus, OH, United States
Synopsis
Keywords: MR-Guided Interventions, Low-Field MRI, Cardiovascular Intevention
Motivation: It is challenging to achieve the spatial and temporal resolutions required for real-time interventional device visualization using low-field scanners with limited gradient performance.
Goal(s): The objective of this study is to develop a novel post-processing method capable of delivering high temporal and spatial resolution images in real-time.
Approach: We developed a method that sequentially combines GRAPPA with a DnCNN denoising network to provide highly accelerated acquisition with low-latency reconstruction. The network was trained using the OCMR dataset and evaluated using pre-clinical data.
Results: The network effectively suppressed noise with minimal latency, while preserving the original features of the image.
Impact: This method could enhance the speed and quality of real-time interventional imaging at low field, making it easier for the interventionalist to visually track devices and deploy stents and other devices.
Introduction
The majority of interventional Cardiovascular Magnetic Resonance (iCMR) work has been performed at 1.5 T, and has largely been limited to diagnostic right heart catheterization1,2. Most commercial catheters and guidewires designed for use with X-ray fluoroscopy are unsafe for iCMR due to RF-induced heating3,4. The lack of safe and effective devices has prevented widespread adoption of iCMR for interventional procedures. The recent introduction of lower field, wide-bore magnets may allow the safe use of many commercially available catheterization devices without modification4; however, reduced signal-to-noise and gradient performance of these scanners limits temporal and spatial resolution.We have performed preliminary, pre-clinical studies in 16 juvenile Yorkshire swine to investigate the feasibility of iCMR on a 0.55T scanner (MAGNETOM Free.Max, Siemens Healthineers AG, Erlangen, Germany) with maximum gradient amplitude and slew rate of 26 mT/m and 45 mT/m/ms, respectively5. In addition to the constraints of low field and slower gradients, the additional equipment needed in the scanner room (Figure 1) can also introduce RF noise. Despite these factors limiting imaging performance, we were able to successfully demonstrate the feasibility of real-time MRI-guided stent deployment with temporal resolution of 231ms and spatial resolution of 3.1 mm. Although these studies were successful5, the combination of low temporal and spatial resolution, and limited signal-to-noise ratio (SNR) made it challenging to visually track devices. While iterative reconstruction methods have proven beneficial for recovering SNR in diagnostic cardiac imaging at low field6, these methods are too slow for MRI-guided interventions. To overcome these challenges, we propose applying a Denoising Convolutional Neural Network (DnCNN)7 to conventional GRAPPA for real time MR guided cardiac interventions at 0.55T.
Methods
Neural Network: We implemented a 20-layer DnCNN (Figure 2), learning from noisy and clean image pairs. For real-time clinical applications, the network is continuously fed with highly accelerated, GRAPPA-reconstructed, noisy images. Given the temporal correlation between frames, the DnCNN was modified to accept four consecutive frames. It then infers the noise distribution and subtracts it from the final frame, producing a denoised version of that frame. For inline use in iCMR, the DnCNN was integrated on the scanner using the Siemens Framework for Image Reconstruction (FIRE) research prototype8 (Figure 3).Training: Training data came from the OCMR dataset9 ,which includes 165 fully sampled, multi-view cardiac cine from 0.55T, 1.5T, and 3T Siemens scanners. Fully sampled cines were resized to 160x128, uniformly downsampled at rate 4, and reconstructed using GRAPPA. The data from 1.5T and 3T scanners were acquired with more receiver coils and had higher SNR compared to 0.55T. To more closely match the SNR of the 0.55T data, only 6 coil elements, chosen based on SNR, were used to reconstruct the 1.5T and 3T data. During the training process, batch size 64, learning rate 1e-5, and epoch 1000 using a combination of L1 and SSIM losses with ADAM optimizer were used. The network was implemented with PyTorch and trained using an Nvidia RTX3090 GPU.
Testing: Network performance was evaluated using a series of 12 multi-frame MRI series (89-563 frames each) acquired during interventional procedures in six pigs. Data acquisition utilized an interactive spoiled gradient echo research sequence, designed for real-time visualization and guidance. The sequence parameters were as follows: temporal resolution 120-180 ms; TE/TR 1.9-2.4 ms/3.8-5.3 ms; flip angles 15-30° at GRAPPA rate 3; spatial resolution 2.13-2.78 mm; slice thickness 10 mm. The real time acquisition was simulated to send data from the MRI scanner to the remote reconstruction server to evaluate latency. SNR in the input and output images were quantified across 24 frames in 12 series and averaged with the methods described in reference10,11. Average processing time for each frame was recorded. For clinical relevance, both the denoised and original raw images were presented to a cardiologist to compare the visibility and clarity of the interventional devices.
Results
Figure 4 shows the direct GRAPPA reconstruction and the corresponding image processed by DnCNN. The denoising network improved SNR by 131±31 %. The interventional cardiologist rated 83% (10 out of 12) of the denoised series as having improved device visibility over the original images. The average processing time per frame using DnCNN was 2.6±0.7 ms, with an additional 50 ms per frame for GRAPPA, meeting the criteria for real-time reconstruction.Discussion and Conclusion
Our proposed DnCNN technique demonstrated a significant reduction of noise in offline MRI-guided intervention simulations. Notably, the visibility of interventional devices and MR-visible markers was enhanced without altering contrast. In future work, we will push the GRAPPA acceleration rate to further improve spatial and temporal resolution.Acknowledgements
No acknowledgement found.References
1. Rogers T, Ratnayaka K, Khan JM, et al. CMR fluoroscopy right heart catheterization for cardiac output and pulmonary vascular resistance: results in 102 patients. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2017;19(1):54. doi:10.1186/s12968-017-0366-2
2. Ratnayaka K, Kanter JP, Faranesh AZ, et al. Radiation-free CMR diagnostic heart catheterization in children. J Cardiovasc Magn Reson Off J Soc Cardiovasc Magn Reson. 2017;19(1):65. doi:10.1186/s12968-017-0374-2
3. Strach K, Naehle CP, Mühlsteffen A, et al. Low-field magnetic resonance imaging: increased safety for pacemaker patients? Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. 2010;12(7):952-960. doi:10.1093/europace/euq081
4. Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
5. Armstrong A, Krishnamurthy R, Swinning J, Liu Y, Joseph M, Simonetti OP. Feasibility of MRI-Guided Cardiac Catheterization, Angioplasty, and Stenting in a 0.55 T Scanner with Limited Gradient Performance. Pediatr Cardiol. 2022;43(8):1934-2029. doi:10.1007/s00246-022-02969-y
6. Simonetti OP, Ahmad R. Low-Field Cardiac Magnetic Resonance Imaging. Circ Cardiovasc Imaging. 2017;10(6):e005446. doi:10.1161/CIRCIMAGING.117.005446
7. Murali V, Sudeep PV. Image Denoising Using DnCNN: An Exploration Study. In: Jayakumari J, Karagiannidis GK, Ma M, Hossain SA, eds. Advances in Communication Systems and Networks. Lecture Notes in Electrical Engineering. Springer; 2020:847-859. doi:10.1007/978-981-15-3992-3_72
8. Veldmann M, Ehses P, Chow K, Nielsen JF, Zaitsev M, Stöcker T. Open-source MR imaging and reconstruction workflow. Magn Reson Med. 2022;88(6):2395-2407. doi:10.1002/mrm.29384
9. Chen C, Liu Y, Schniter P, et al. OCMR (v1.0)--Open-Access Multi-Coil k-Space Dataset for Cardiovascular Magnetic Resonance Imaging. Published online August 12, 2020. Accessed September 3, 2023. http://arxiv.org/abs/2008.03410
10. Ding Y, Chung YC, Simonetti OP. A method to assess spatially variant noise in dynamic MR image series. Magn Reson Med. 2010;63(3):782-789. doi:10.1002/mrm.22258
11. Veraart J, Fieremans E, Novikov DS. Diffusion MRI noise mapping using random matrix theory. Magn Reson Med. 2016;76(5):1582-1593. doi:10.1002/mrm.26059
Figures

Figure 1: Equipment available for iCMR in Free.Max scanner room. 1. Free.Max 0.55T MR scanner 2. NNL MR conditional monitor 3. Philips patient monitor 4. IRADIMED patient monitor 5. IRADIMED infusion pump
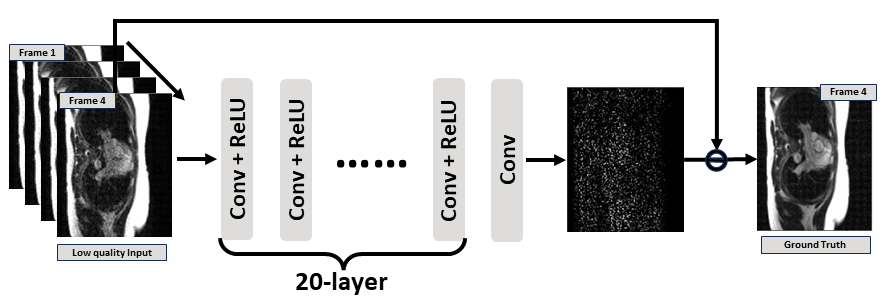
Figure 2: the architecture of the 20-layer DnCNN network and how the input and output data were arranged. The network was adapted to learn the noise by residual training. The 4-frame dimension of the input was treated as separate channels.
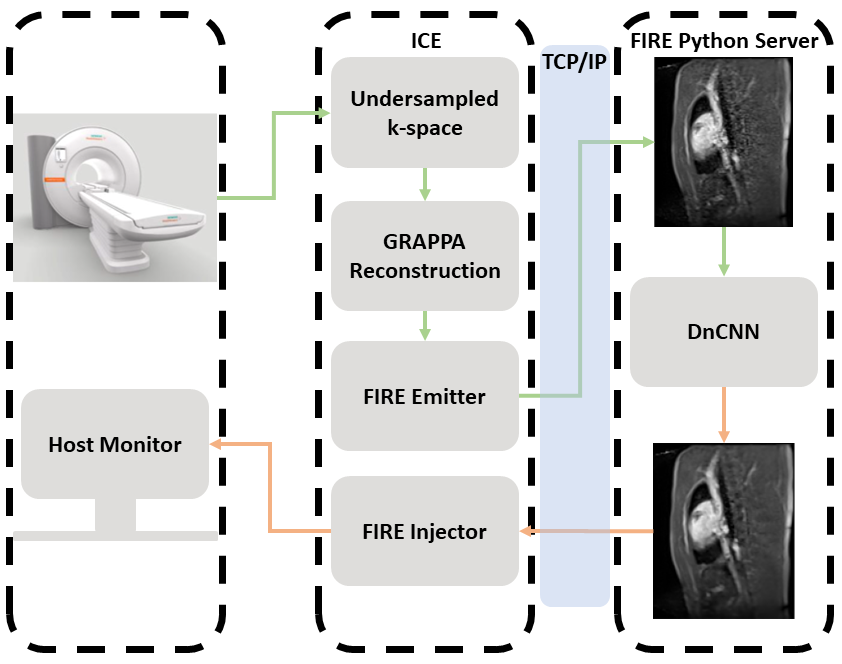
Figure 3: The schematic shows how the DNCNN network is integrated to the scanner with Siemens FIRE. After the undersampled image is reconstructed, it is sent to remote Python server via TCP/IP connection. After the image is denoised by DnCNN, it is reinjected into the ICE pipeline and fed to the scanner host monitor for real-time display.
Figure 4: a) image before processing by DnCNN b) image after processing by DnCNN. Both figures are displayed with the same window/center settings