0461
Clinical Application of Semi-Automatic Device Guidance in MR-Guided Transperineal Prostate Interventions: Biopsy and Cryoablation1Medical Physics, University of Wisconsin at Madison, Madison, WI, United States, 2Biomedical Engineering, University of Wisconsin at Madison, Madison, WI, United States, 3Radiology, University of Wisconsin at Madison, Madison, WI, United States
Synopsis
Keywords: MR-Guided Interventions, Interventional Devices, Cryoablation
Motivation: In the prostate, transperineal needle placement is often assisted with trajectory guides and imaging. Improper placement necessitates needle reinsertion, increasing procedure time and complication risk. Presented here is a straightforward platform tested in multiple biopsy and cryoablation procedures. Previous work demonstrated feasibility in a single MR-guided focal biopsy.
Goal(s): To demonstrate the platform’s technical feasibility across greater procedural types and numbers.
Approach: The proposed techniques were performed on consented patients. These procedures included prostate cryoablations, biopsies, and fluid aspirations.
Results: 12 procedures were performed- 6 cryoablations, 5 biopsies, and 1 fluid aspiration. Technical success was achieved in every procedure.
Impact: Using the proposed methodology, all 12 prostate procedures achieved technical success. With the platform’s support, a median procedure saw satisfactory needle placement in 83.7% of initial insertions, requiring no further adjustment. This can reduce procedure times and complication risks.
Introduction
In minimally invasive prostate interventions, MR-imaging guidance is often used in conjunction with external trajectory guides to percutaneously drive needles into tissues. Therapeutic and/or diagnostic efficacy require precise placement in deep tissues. Needles with unsatisfactory placement are reinserted, which prolongs procedures and can increase complication risk from additional skin punctures. Robotic guided prostate biopsy systems1 require significant capital investment and additionally trained while their utility is narrow in the scope of interventional procedures. Previous work proposed a simple grid-and-software system for using prescriptive imaging to target and guide needles into specific regions in the prostate, providing clinicians with accurate initial trajectories and in-built procedure monitoring2. The system was made to prioritize minimal capital investment and maintenance, ease of use, and mechanical simplicity. We previously demonstrated the efficacy of this methodology in a single biopsy procedure3.Cryoablations, a more complex procedure, require additional guidance with real-time monitoring to track the ablating iceball’s growth and extent4. Here, we present the progression and further application of our earlier work, reporting 12 image guided prostate interventions, including cryoablations, biopsies, and a fluid aspiration.
Materials and Methods
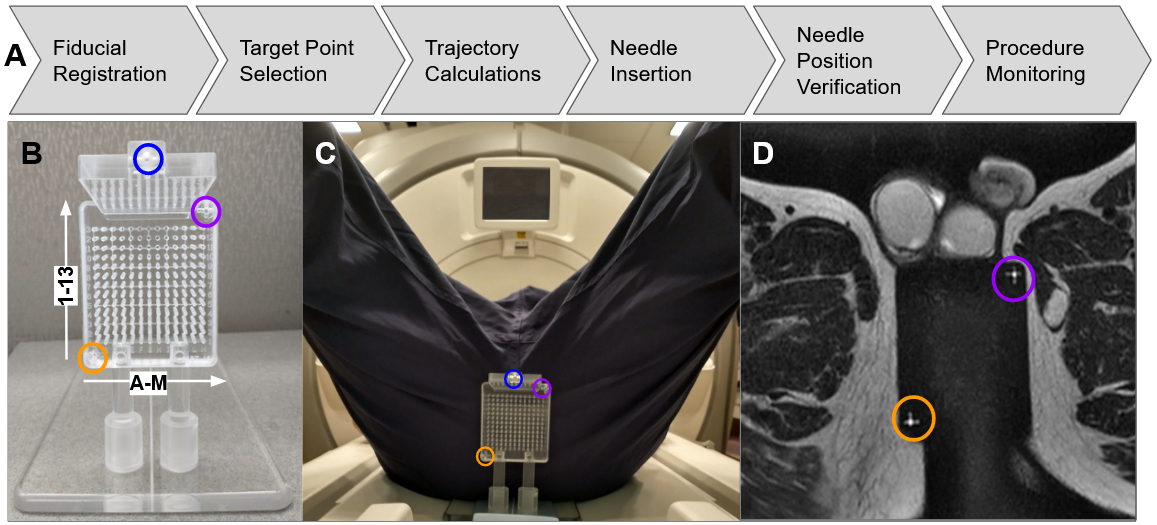
All procedures were performed under IRB approval on consented patients at the University of Wisconsin Hospital and Clinics on a GE450W scanner using an external pelvic coil. The generalized workflow utilized in these procedures is outlined in Figure 1.Targeting Methodology:
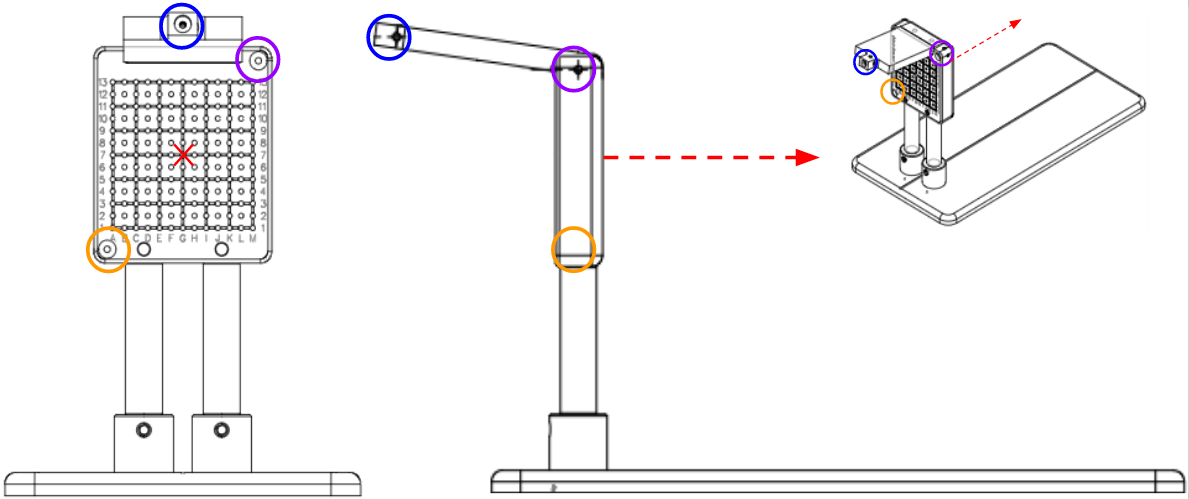
The targeting grid, detailed in Figure 2, features 169 uniquely-labeled parallel channels through which needles may be inserted. It has three fiducials for registration when imaged via MRI. A single scan containing all three fiducials and the prostate enables a series of geometric calculations through which an optimal grid channel and depth can be determined in order to guide a needle to a specifically-targeted location in the prostate. Associated software, as explained in prior works2,3, helps achieve this. For targeting validation, a successful trial is indicated by satisfactory placement in a needle’s first insertion. If a needle’s positioning was deemed unsatisfactory by clinicians, it would be removed and reinserted. Biopsies normally require multiple needle insertions to acquire sufficient tissue samples. Cryoablations, performed using the Boston Scientific VISUAL ICE system (Boston, MA), use up to 5 needles to sculpt asymmetric freeze zones around targeted regions. Unsatisfactory positioning is frequently attributed to needle deflection, which is elaborated upon in the Discussion. For each procedure, we report the percentage of needles that were correctly positioned in a single attempt, with no further adjustments.
Patient Demographics:
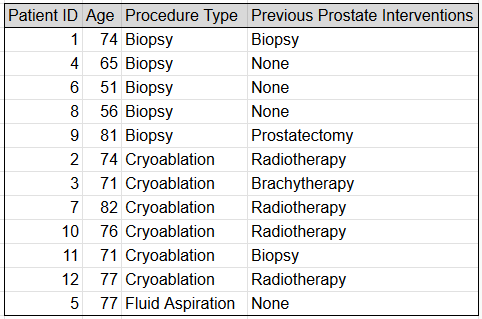
All patients were over the age of 50 (range 51-82, mean 71). Most cryoablation patients had previously received other prostate cancer treatments, including surgical resections, brachytherapy, and external beam radiotherapy. These demographics are collated in Figure 3.
Procedures:
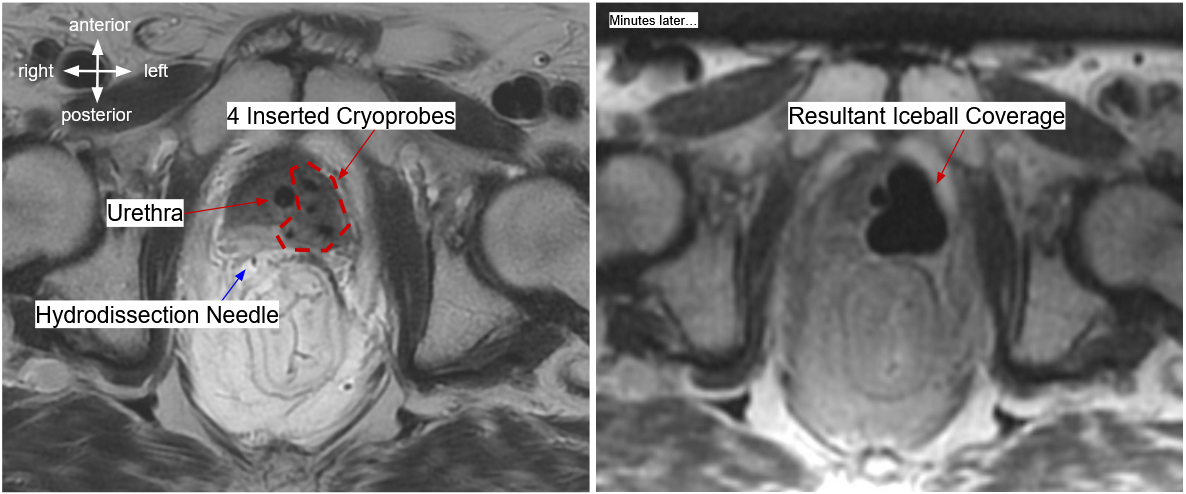
The reported procedures include 6 cryoablations, 5 biopsies, and 1 fluid aspiration. Each used the same needle placement methodology (Figure 1). During cryoablation, these cryoneedles induce sub-freezing temperatures via the Joule-Thompson effect, freezing malignant tissues and killing off cancerous cells. The frozen volume of tissue expands gradually around the probes. Iceball growth is monitored with real-time imaging to ensure the ice ball does not encroach on any sensitive organs while still attaining sufficient coverage of the intended tissues. Hydrodissection needles may be used to shift tissues in the patient, enabling better therapeutic coverage. For biopsies, it is sufficient to maneuver the needles into an adequate position for acquiring samples from targeted tissues. Fluid aspirations pierce an abscess to allow its drainage.
Results
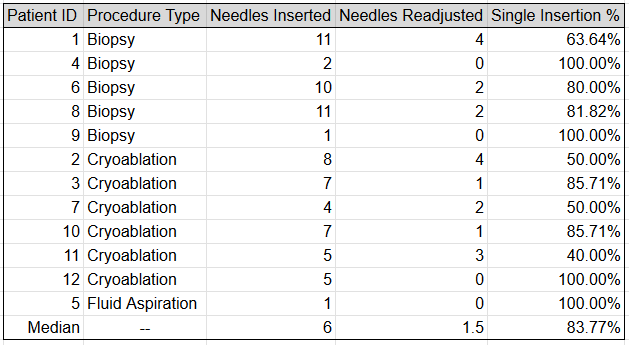
We report 12 patient trials across multiple procedure types. All procedures achieved technical success, with reports of clinical success awaiting 12-month followup measurements of prostate-specific antigen (PSA). Our primary reported metric is the number of inserted needles, per procedure, which required no readjustment after insertion. In an average (median) procedure, 83.7% of needles required no adjustment. Figure 4 collates these results. No patients experienced serious post-procedural complications.Discussion
Needles do not always attain the idealized trajectories proposed by the algorithm. This is due primarily to deflection, a common occurrence in such interventions5. Inhomogeneities and tissue interfaces can apply resistive forces on advancing needles, causing them to deflect off-trajectory. This is difficult to predict. Deflection may be minimized through real-time imaging, informing clinicians when deflection begins to occur and allowing them to adjust their approach by applying torque or twisting.Conclusion
The proposed methods demonstrated technical success in 12 patient trials. In a median procedure, needles were successfully guided into targeted prostate tissues with no further adjustments required 83.7% of the time, per procedure.Acknowledgements
We acknowledge GE-Healthcare and UW-Madison for research support.
This work was completed with funding from the University of Wisconsin School of Medicine and Public Health and the UW Department of Radiology.
We thank the Mayo Clinic Interventional MRI Program and Mayo Clinic Department of Engineering for their collaboration on this project.
References
[1] Hata, N; Moreira, P; Fischer, G. Robotics in MRI-Guided Interventions. Topics in Magnetic Resonance Imaging 27(1):p 19-23, February 2018. | DOI: 10.1097/RMR.0000000000000159
[2] Lilieholm T, Moskwa R, Ozhinsky E, Woodrum D, Block WF, Knavel Koepsel E, Platform for Real-Time Multiplane Targeting and Monitoring of Minimally-Invasive Image-Guided Prostate Cryoablation Procedures, Proc. of International Society of Magnetic Resonance in Medicine, 2022.
[3] Lilieholm T, Woodrum D, Block WF, Knavel Koepsel E, Implementation of Proposed Methods for MR-Guided Transperineal Prostate Interventions: Real Time Trajectory Calculation and Monitoring, Proc. of International Society of Magnetic Resonance in Medicine, 2023.
[4] Woodrum DA, Kawashima A, Karnes RJ, Davis BJ, Frank I, Engen DE, Gorny KR, Felmlee JP, Callstrom MR, Mynderse LA. Magnetic resonance imaging-guided cryoablation of recurrent prostate cancer after radical prostatectomy: initial single institution experience. Urology. 2013 Oct;82(4):870-5. doi: 10.1016/j.urology.2013.06.011. Epub 2013 Aug 1. PMID: 23910089.
[5] Abolhassani N, Patel RV. Deflection of a flexible needle during insertion into soft tissue. Conf Proc IEEE Eng Med Biol Soc. 2006;2006:3858-61. doi: 10.1109/IEMBS.2006.259519. PMID: 17946584.
Figures