0460
Clinical Feasibility of MRI-guided Robotic and Percutaneous In-Bore Prostate Biopsies at 0.55T1Radiology, Univeristy of Michigan, Ann Arbor, MI, United States, 2Radiology, University of Michigan, Ann Arbor, MI, United States, 3University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: MR-Guided Interventions, Prostate, MRI-guided intervention
Motivation: MR-guided prostate biopsies are important for sampling indeterminate lesions and are performed at 1.5 or 3T.There are potential advantages of performing interventions on lower field scanners due to their potential to decrease needle artifact width, larger bores to accommodate hardware, improved imaging in presence of metallic implants, and patient comfort. However, lesion/needle visualization, SNR, and ability to target lesions could be challenging at lower fields.
Goal(s): To assess feasibility of MRI-guided prostate biopsies on a low field scanner.
Approach: We performed 5 in-vivo biopsies and did histopathological correlation.
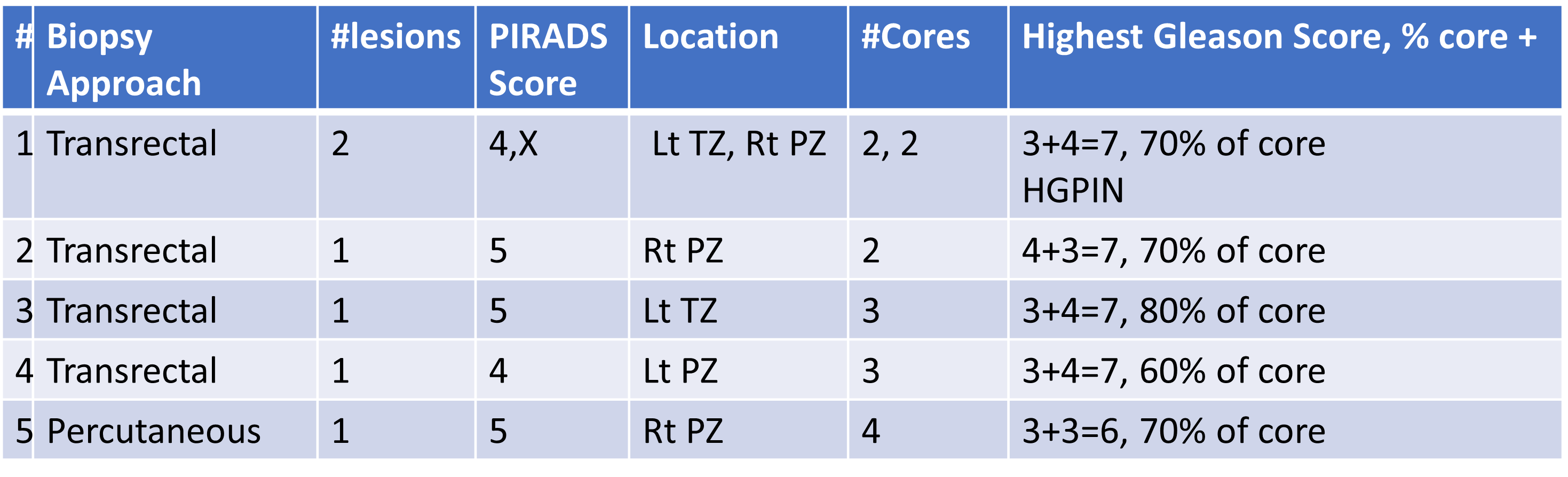
Results: We performed successful biopsies and high volume disease was found in all cases.
Impact: Successful lesion visualization and percutaneous and transrectal prostate biopsies are possible on high access, wide bore 0.55 T scanners, widening the clinical feasibility and utility of in-bore MRI guided intervention.
Introduction
We evaluated the feasibility of targeted MRI-guided prostate biopsies using a 0.55T MRI scanner. The keys to a successful biopsy are precise lesion localization, and needle identification in the lesion. Prostate is challenging due to small lesion sizes and the heterogeneity of the transition zone. Conventionally, the prostate is systematically sampled with 12 cores using transrectal rectal ultrasound (TRUS) guidance. An MRI-TRUS fusion biopsy of MRI suspicious foci is often added.(1) However, difficult to biopsy scenarios still commonly arise, for which direct MR targeting can be desirable. Lower field strengths have advantages for intervention including reduced susceptibility artifacts, wider bores, and lower operational costs.(1–3) There are also potential limitations, such as poor lesion visualization, insufficient needle conspicuity, low SNR. In this work, we explore the ability to identify cancer suspicious foci in the prostate at 0.55T for biopsy, and to target them in-bore using transrectal and percutaneous approaches.Methods
In this IRB-approved work we conducted five in-vivo biopsies with informed consent, in patients with suspicious prostate lesions (size 0.7-2.1cm) using a 0.55T scanner (Siemens Free.Max). Pre-biopsy T2w TSE scans (AT -2.06m, thickness 3mm, TR/TE 3020/95ms, matrix 272x231,FOV 219x219mm) were obtained to determine if the lesion could be identified at 0.55T. Tumor and needle localization was performed at 0.55T with assistance of single-shot T2-weighted (HASTE) (Acquisition time (AT)2.24mins,thickness 3mm, TR/TE 1140/72ms,matrix 250x205,FOV 256x256mm), conventional TSE (AT 2.18mins, thickness 3.5mm, TR/TE 3650/126ms, 250x205,matrix 256x192,FOV 256x256mm) or bSSFP (TrueFISP) (AT 2.19mins thickness 4.5mm, TR/TE 1484/3.22ms, matrix 224x158,FOV 250x250mm) sequences. Four biopsies were carried out under local anesthesia using a transrectal approach, employing a robot-controlled manipulator to aid targeting via an intrarectal directing device (Soteria Medical, Arnhem, Netherlands). Patients were positioned prone and headfirst. A needle introducer system was inserted into the rectum and the needle advanced after robotic targeting. 2-3 cores per lesion were collected. For the percutaneous approach, the patient had a PIRADS-5 lesion but no rectum. A 16-gauge introducer was inserted into the prostate under moderate sedation and local anesthesia, and four 18-gauge core specimens were obtained. All collected samples were sent for histopathological analysis.Results
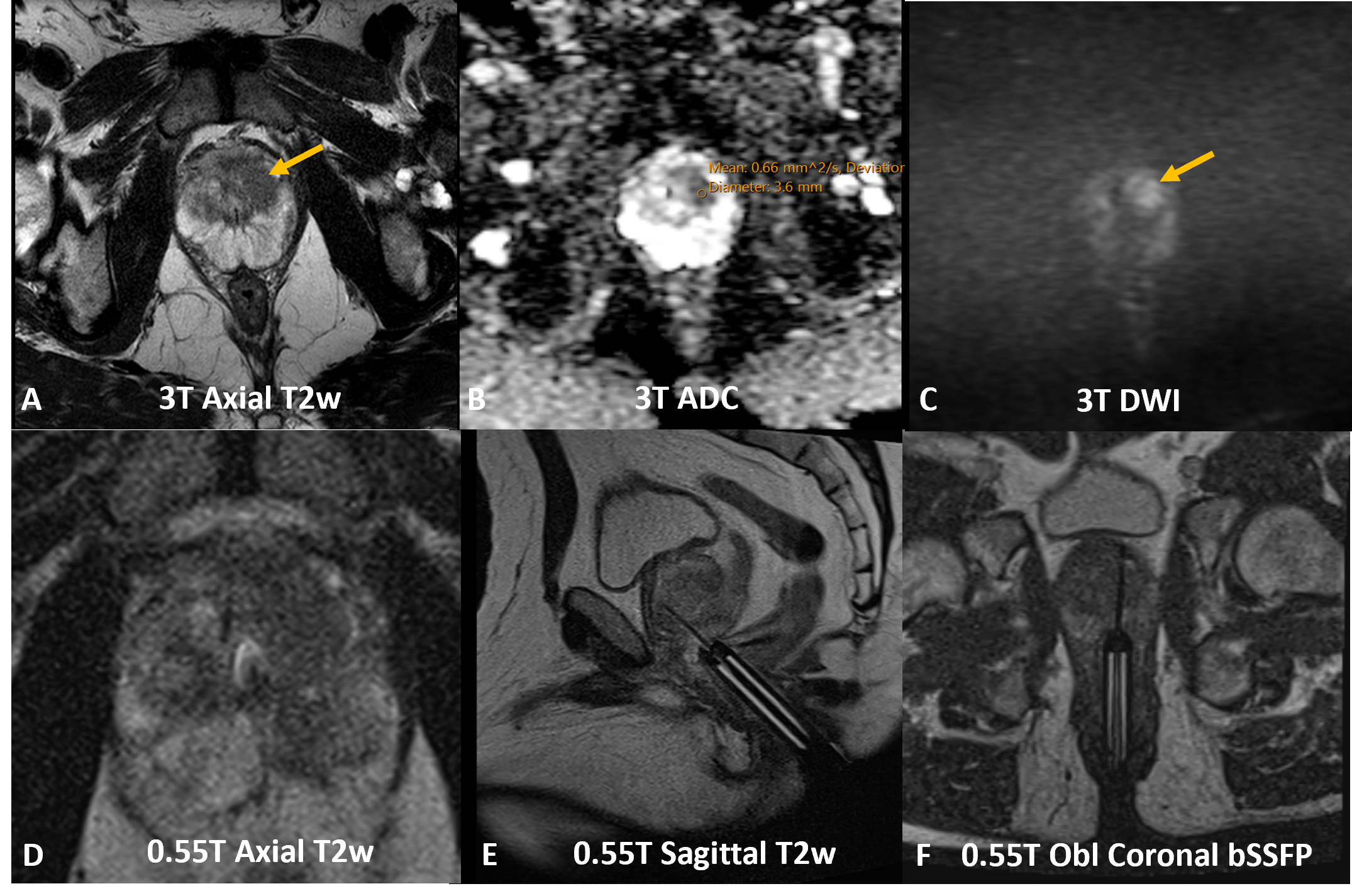
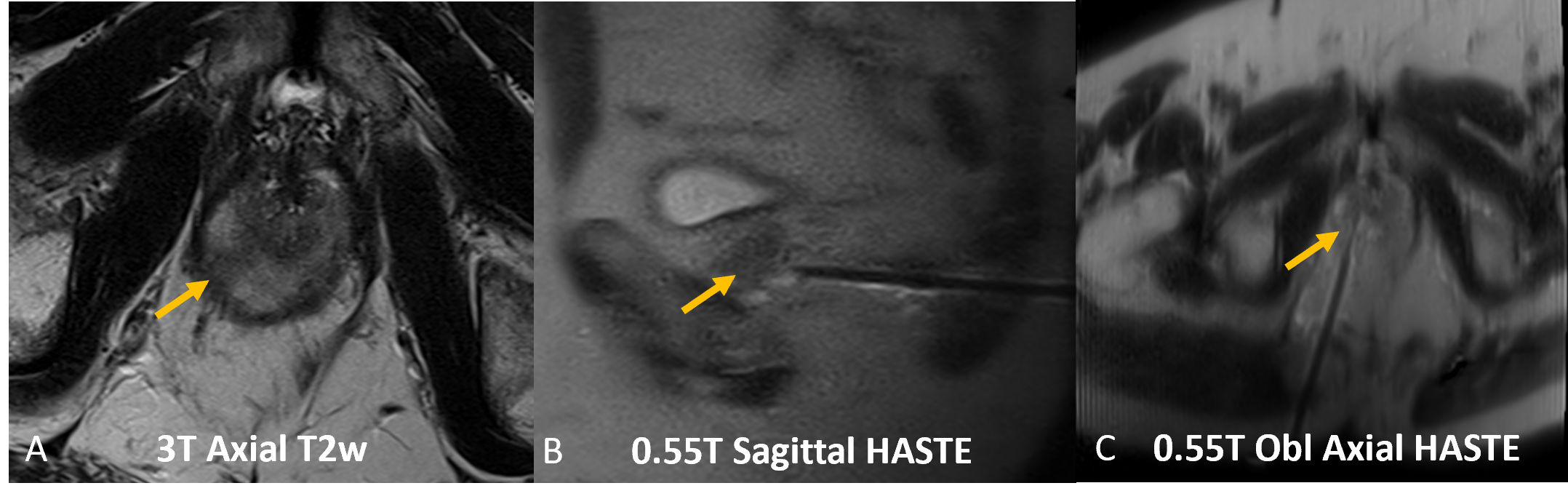
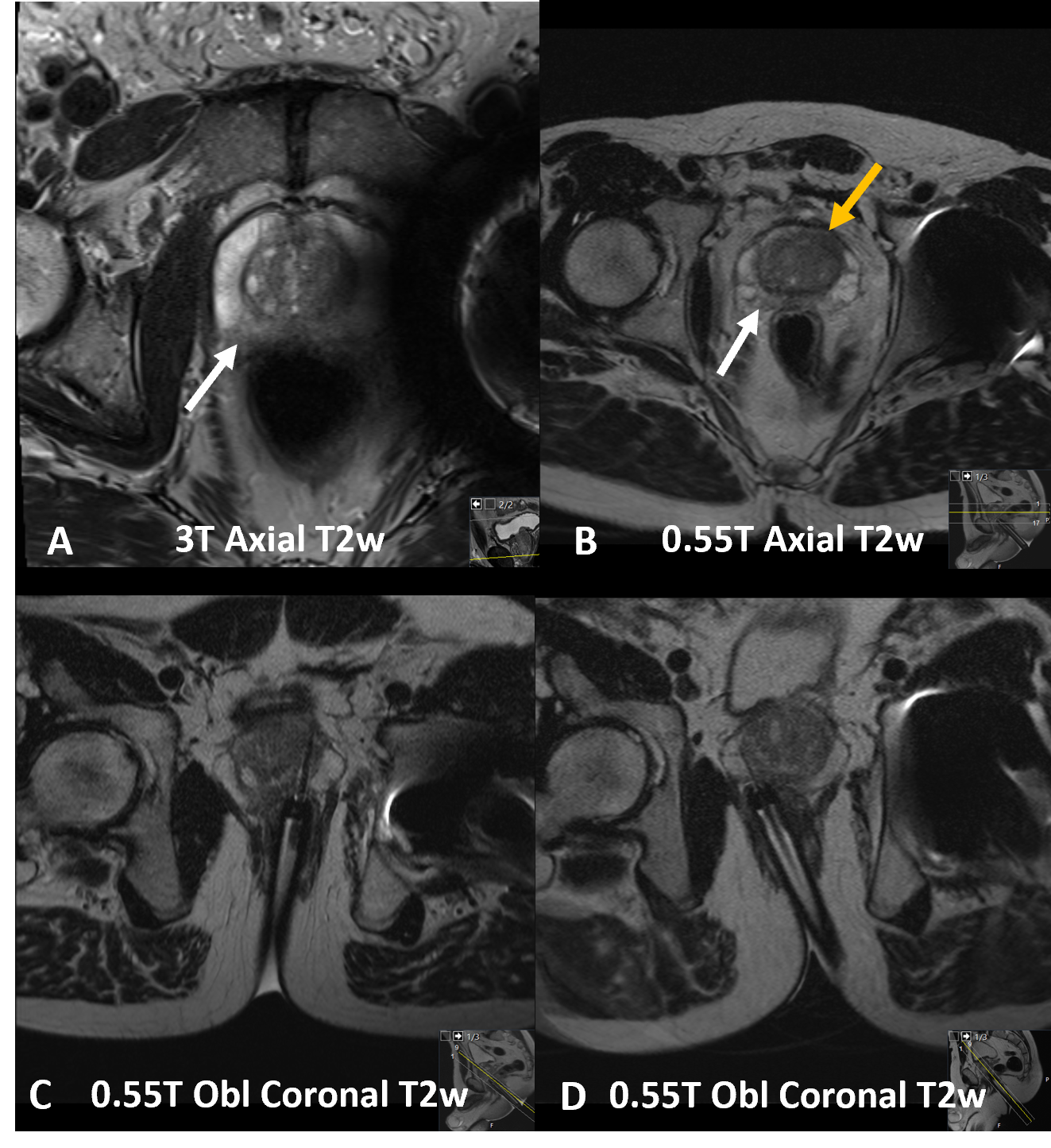
Figure 1 shows diagnostic 3T images (A-C) from a patient with a left anterior TZ lesion, the ability to visualize the lesion (D) and target it (E-F). In all 5 patients, the histopathological results (Table 1) were positive for high volume cancer (largest positive cores ranged from 60-80% cancer). Figure 1(A-F) depicts successful identification and transrectal targeting of a PIRADS 5 lesion. Figure 2(A-C) shows percutaneous targeting of a right apical lesion in a patient lacking a rectum. 4 of 5 patients had intermediate grade (Grade Group 2) or higher cancer. Figure 3(A-D) shows transrectal biopsy in a patient with a hip implant, known to have a R PZ PIRADS 4 lesion, rising PSA (25.2ng/mL), and four prior negative biopsies over 6 years. An additional L TZ lesion was identified at 0.55T, which yielded clinically significant (GG2) cancer.Discussion and Conclusions:
The work shows that lesion identification is possible at low field prior to biopsy, even on lower resolution scans. It also shows that SNR considerations do not preclude successful biopsy; high volume disease was found in all patients, and in 5/6 lesions biopsied. Both percutaneous and transrectal routes are clinically feasible, for lesions as small as 7mm. Figure 3 (biopsy in a patient with a hip arthroplasty) shows a lesion that was uncovered because of lower field scanning, ending a 6 year period of uncertainty, and highlighting the utility of low field imaging/biopsy in patients with implanted devices. In the case in which a percutaneous route (Figure 2) was used because the patient does not have a rectum, we again show successful tissue sampling. An introducer-biopsy combination device was successfully guided to the mass and used for biopsy. This case demonstrates the utility of low field intervention for percutaneous biopsy, even for small foci such as those encountered in prostate. In all cases, the biopsy results contributed to a change in patient management. The work shows the utility of low field MRI-guided interventions as a problem-solving tool in difficult circumstances such as high suspicion lesions or rising PSA but negative biopsy, or patients lacking a rectum and who cannot get transrectal biopsy. Enabled by availability of targeting equipment and MRI compatible biopsy needles and other hardware, MRI guided in-bore biopsy is an accurate alternative in these situations, offering tissue sampling with direct verification of needle location within the suspicious focus.Acknowledgements
Support for this study was provided by NIH grants R37CA263583 and R01CA208236, and Siemens Healthcare.References
1.Seetharam Bhat KR, Samavedi S, Moschovas MC, et al. Magnetic resonance imaging-guided prostate biopsy—A review of literature. Asian Journal of Urology. 2021;8(1):105-116. doi:10.1016/j.ajur.2020.07.001
2.Yacoub JH, Verma S, Moulton JS, Eggener S, Oto A. Imaging-guided Prostate Biopsy: Conventional and Emerging Techniques. RadioGraphics. 2012;32(3):819-837. doi:10.1148/rg.323115053
3.Hori M, Hagiwara A, Goto M, Wada A, Aoki S. Low-Field Magnetic Resonance Imaging. Invest Radiol. 2021;56(11):669-679. doi:10.1097/RLI.0000000000000810
Figures