0458
SPARTA-3D: 3D Real-time Tracking Solution for Interventional MRI1United Imaging Healthcare, Houston, TX, United States, 2United Imaging Healthcare, Shanghai, China
Synopsis
Keywords: MR-Guided Interventions, MR-Guided Interventions, 3D real-time imaging
Motivation: MRI excels in exceptional soft tissue delineation and its radiation-free nature in interventional contexts. However, achieving effective 3D real-time tracking with MRI poses a significant challenge.
Goal(s): To facilitate 3D real-time monitoring and navigation, achieving a high temporal resolution and enhanced spatial resolution that precisely captures the movement of small interventional instruments.
Approach: We utilized a manually controlled device and employed highly accelerated golden-angle rotated spiral-in/out sequence with randomized variable density kz encoding, along with a specifically tailored iterative reconstruction algorithm.
Results: High temporal (150 ms/phase) and spatial (0.7×0.7×1.5 mm3) resolutions were achieved, smoothly visualizing minute movements in 3D within our phantom setup.
Impact: The SPARTA-3D approach holds the promise of revolutionizing interventional MRI by meeting the crucial demand for 3D real-time tracking and navigation. It could facilitate more rapid and less invasive procedures, opening up novel avenues in the domain of MR-guided interventions.
Introduction
MRI is renowned for its exceptional soft tissue differentiation and the absence of ionizing radiation exposure, thus is suitable for interventional applications.1,2 However, achieving three-dimensional (3D) real-time tracking of the interventional tools and anatomical features is still a formidable task.3 Current methodologies often fall short in providing the requisite precision, agility, and 3D imagery crucial for meticulous intervention applications. To overcome these obstacles, we present an innovative tracking technique, namely SPARTA-3D (SPiral Accelerated Real-Time trAcking-3D), which employs spiral acquisition to refine the speed and guidance precision used in interventional MRI. For demonstration and validation, an in-house gel-based phantom and a slimline probe were used to simulate tool motions in interventional MRI and test the 3D real-time tracking capacity of the proposed method. Our approach marks a significant leap forward, with the promise to improve the efficacy of MR-guided intervention applications.Methods
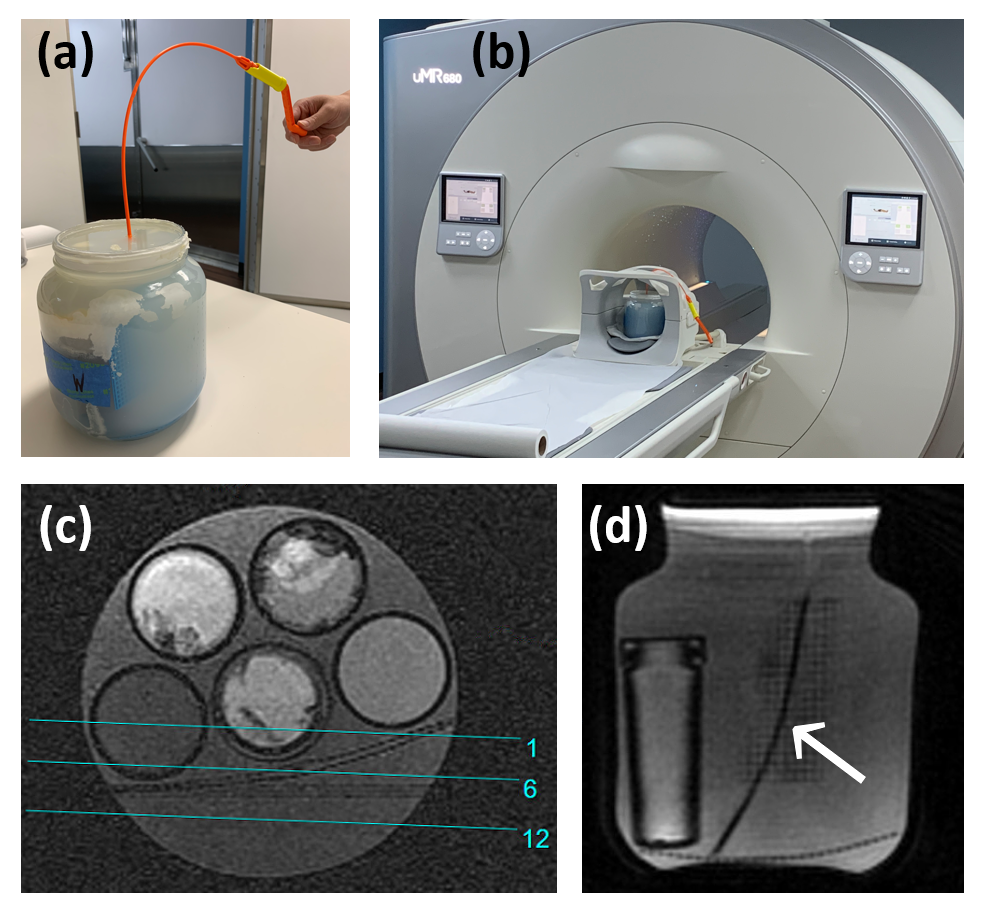
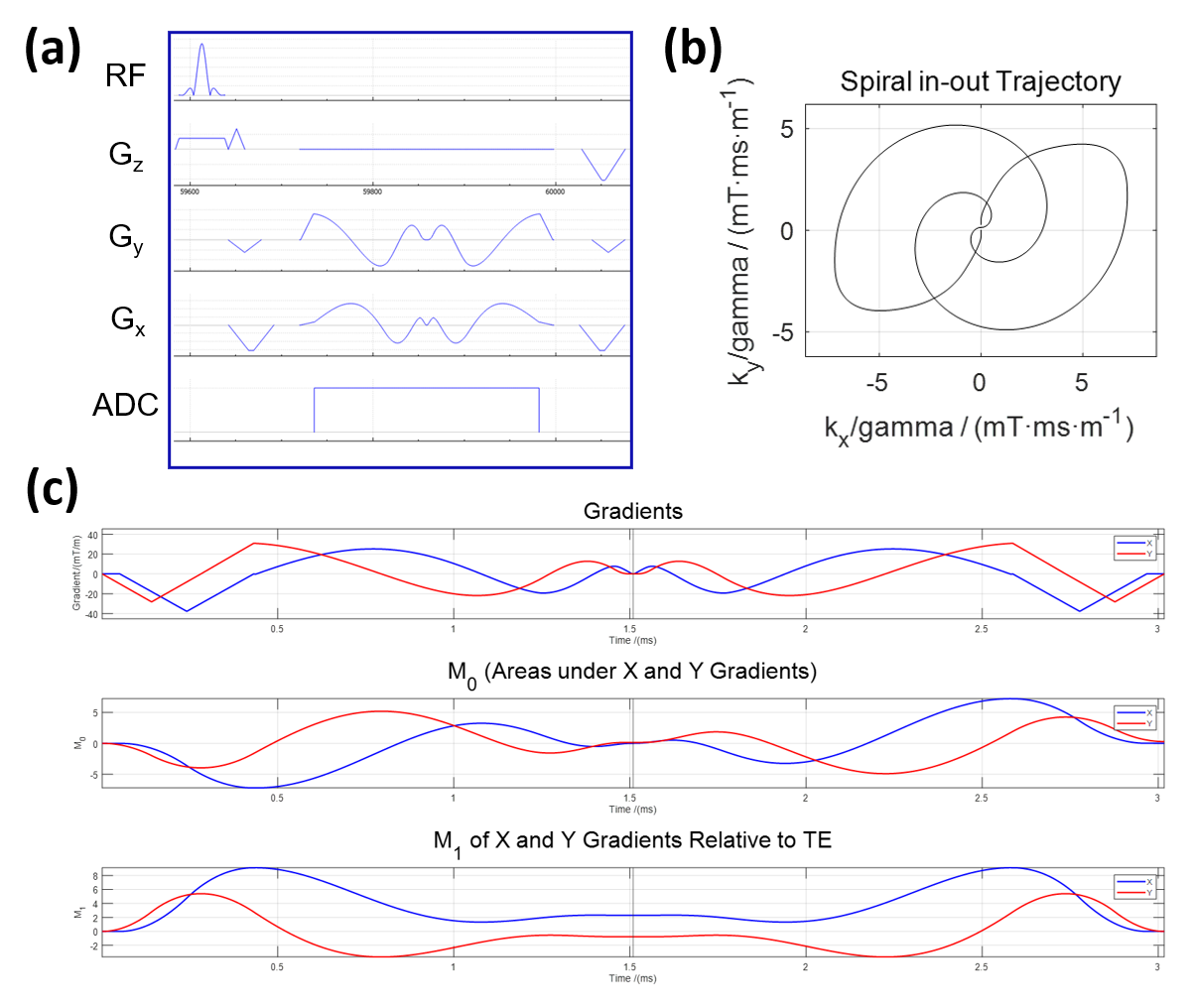
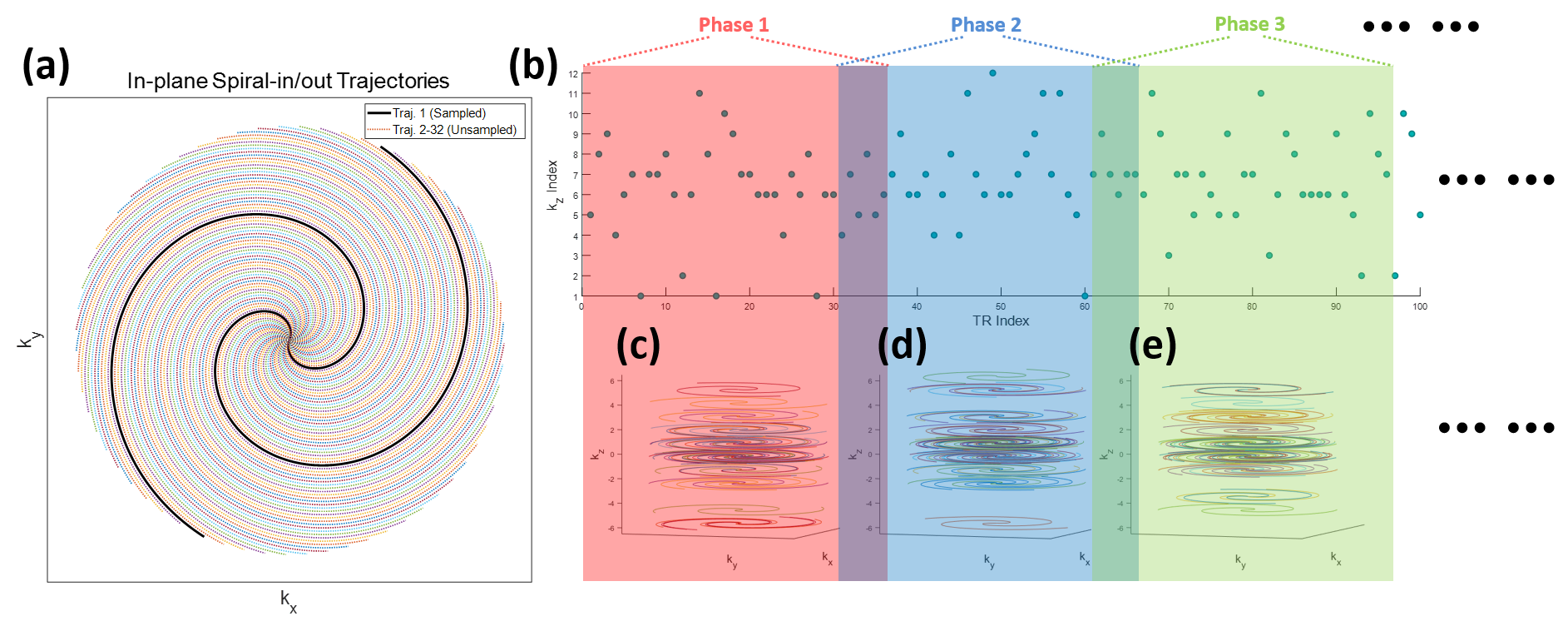
A custom-assembled jar phantom consisting of gel and test tubes imbued with substances to create distinct MR contrasts was used. To mimic an interventional maneuver, akin to the needle insertion into a vessel, a 2.5 mm narrow conduit was manually guided through a descending motion (Figure 1a). The assembly was placed within a 24-channel head coil for the experiment on a 1.5T system (uMR 680, United Imaging Healthcare, Shanghai, China) (Figure 1b). To indicate the commencement and conclusion of our process, a pre-penetration coronal image (Figure 1c) and a post-penetration transverse image of the conduit (Figure 1d) are displayed.For real-time observation, a high-speed 3D spiral-in/out capture method was employed (Figure 2a), with the complete in-plane k-space trajectory shown in Figure 2b. This technique, based on a balanced steady-state free precession (bSSFP) sequence, ensures zeroth order moment nulling at each TR cycle's end (Figure 2c, middle). Additionally, nulling for the first-order moments, a specific advantage of spiral-in/out (Figure 2c, bottom), renders the imaging insensitive to in-plane fluid flows.4 We used a 32-fold in-plane acceleration to capture a single spiral-in/out interleaf out of 32 full-sample interleaves in the kx-ky plane (Figure 3a). In the slice direction, kz phase encoding employed a randomized variable density scheme (Figure 3b), with each subsequent TR involving a 222.5° golden-angle rotation.
Each set of 36 TRs produced a single temporal phase with data-sharing from the preceding 6 TRs, represented by overlapping colored shades in Figure 3. Key parameters included TR=5.0 ms, resulting in a temporal resolution of 150 ms (5.0 ms×(36-6)); TE=2.5 ms. k-space trajectories for the initial three phases are displayed in Figure 3c-e. Other conditions: a flip angle, 23°; FOV, 180×180 mm2; matrix size, 128×128; slice thickness 3 mm; and 12 slices. A two-fold interpolated spatial resolution of 0.7×0.7×1.5 mm3 can be achieved.
The experimental procedure commenced when an operator, positioned beside the scanner, initiated the conduit's descent into the gel phantom. The entire process lasted for 10 seconds once the scanning was initiated. The initial 240 TRs were set for achieving a steady state and not included for reconstruction, and 58 phases of 3D images were subsequently reconstructed. A gradient-impulse response function (GIRF) correction was integrated with the k-space trajectory,5 and the data was processed through an iterative reconstruction incorporating spatio-temporal constraints as specified in the referenced literature.6
Results
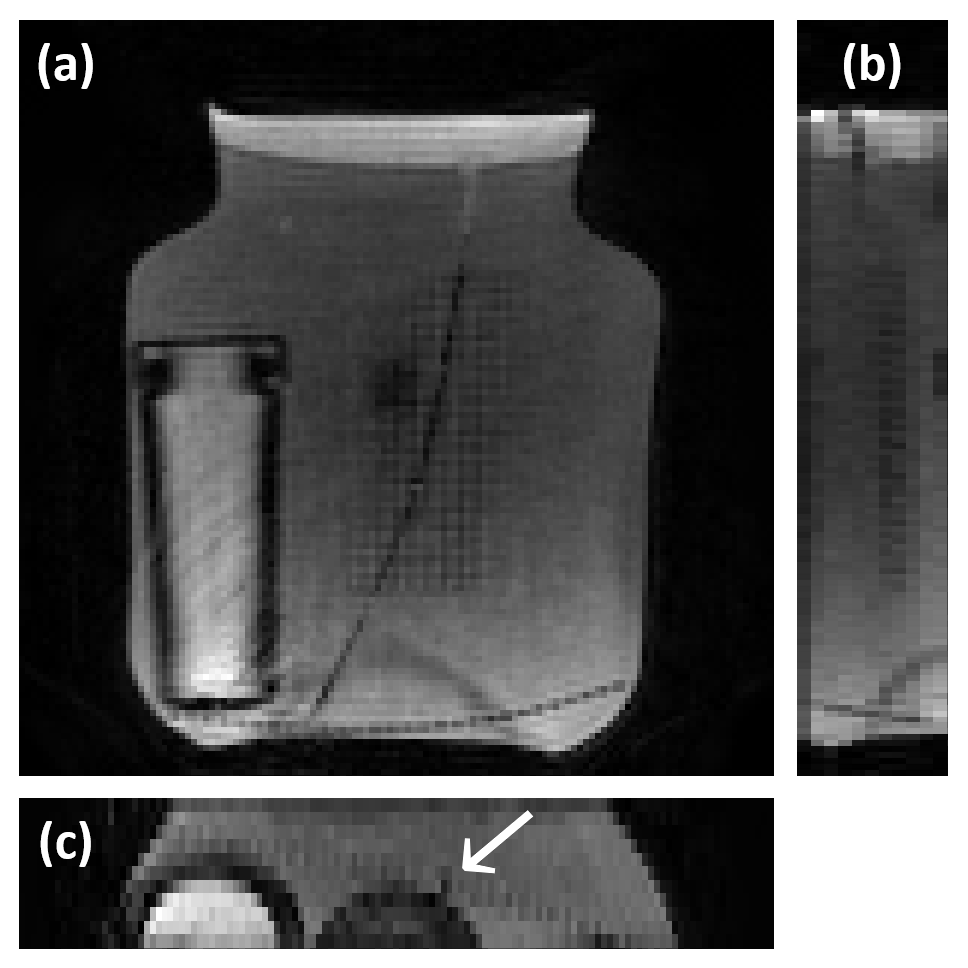
Figure 4 showcases images from three orthogonal planes, which were captured upon the reconstruction of the dynamic sequence following the completion of the penetration activity. The regions where the conduit was inserted appeared dark. In Figure 5, the dynamic process is rendered as a repeating movie, providing an exceptional three-dimensional, multi-slice view that precisely delineates the position and trajectory of the conduit’s penetration within the phantom, as highlighted by the arrows. Before the conduit entered, the bright signal within the conduit's path was attributed to water that had been pre-introduced.Discussion and Conclusion
We unveiled a trailblazing strategy for 3D, real-time data capture in the context of interventional MRI, capitalizing on the sophisticated spiral-in/out acquisition technique. While we have attained an impressive temporal resolution of 150 ms, there is potential for further enhancement to track even swifter movements. This includes the unique advantage of adjusting the number of TRs used for reconstructing a single phase, a distinctive feature of the SPARTA-3D technique. Similarly, the in-plane spatial resolution can be refined to sub-millimeter precision, allowing for meticulous monitoring of intervention dynamics. This technique can be integrated with AI-driven real-time reconstruction in future studies, and can offer a highly promising pathway toward accomplishing live 3D data gathering and image reconstruction in interventional MRI settings. This approach has the potential to dramatically reform interventional MRI procedures and substantially improve clinical outcomes.Acknowledgements
No acknowledgement found.References
1. Brock, K. K., Chen, S. R., Sheth, R. A., & Siewerdsen, J. H. (2023). Imaging in Interventional Radiology: 2043 and Beyond. Radiology, 308(1), e230146.2. Nayak, K. S., Lim, Y., Campbell‐Washburn, A. E., & Steeden, J. (2022). Real‐time magnetic resonance imaging. Journal of Magnetic Resonance Imaging, 55(1), 81-99.
3. Thorwarth, D., & Low, D. A. (2021). Technical challenges of real-time adaptive MR-guided radiotherapy. Frontiers in oncology, 11, 634507.
4. Feng, X., Salerno, M., Kramer, C. M., & Meyer, C. H. (2016). Non‐Cartesian balanced steady‐state free precession pulse sequences for real‐time cardiac MRI. Magnetic Resonance in Medicine, 75(4), 1546-1555.
5. Robison, R. K., Li, Z., Wang, D., Ooi, M. B., & Pipe, J. G. (2019). Correction of B0 eddy current effects in spiral MRI. Magnetic Resonance in Medicine, 81(4), 2501-2513.
6. Zhao, Z., Lim, Y., Byrd, D., Narayanan, S., & Nayak, K. S. (2021). Improved 3D real‐time MRI of speech production. Magnetic Resonance in Medicine, 85(6), 3182-3195.
Figures