0456
Model-Based Rapid 3D Passive Needle Localization for Automatic Slice Positioning in MR-Guided Interventions1Siemens Healthcare GmbH, Erlangen, Germany, 2Faculty of Physics and Astronomy, Ruprecht-Karls-Universität Heidelberg, Heidelberg, Germany, 3Cook Advanced Technologies, West Lafayette, IN, United States, 4Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany, 5Faculty of Medicine, Ruprecht-Karls-Universität Heidelberg, Heidelberg, Germany
Synopsis
Keywords: MR-Guided Interventions, MR-Guided Interventions, needle intervention, percutaneous intervention, needle tracking, needle localization, device tracking, passive tracking, modelling
Motivation: For MR-guided needle interventions, rapid 3D needle localization enables automatic realignment of 2D real-time imaging slices with the device during the procedure.
Goal(s): To investigate a model-based approach for rapid 3D needle localization that does not require prepositioned tracking slices.
Approach: 3D k-space data was radially acquired before and after needle placement. Two algorithms to extract position and orientation of the needle were introduced and compared (artifact model fit to undersampled subtraction k-space/image).
Results: Model-based rapid 3D needle localization was successfully demonstrated in-vivo (k-space-based offline localization error 4.3mm for FOV of (256cm)3 in 1.1s combined acquisition and localization time using 64 k-space spokes).
Impact: Model-based rapid 3D passive needle localization shows potential to improve the workflow of MR-guided needle interventions, allowing for automatic alignment of 2D real-time imaging slices with the needle trajectory.
Introduction
In MR-guided in-bore needle interventions, typically 2D real-time imaging is used to monitor the advancement of the needle.1,2 If the needle is out-of-plane, imaging slice realignment becomes necessary. To provide an Automatic Slice Positioning (ASP) functionality to the interventionalist without interrupting the procedure workflow, rapid needle localization is required. Approaches to ASP often localize the needle in multiple 2D tracking slices which must be positioned a priori.3-6 Recently, a Convolutional Neural Network-based method was introduced to rapidly localize a needle from undersampled 3D images.7 In this work, we propose a model-based approach to rapid 3D needle tracking as an alternative that does not require training of a neural network.Methods
Two different algorithms for model-based needle localization (Fig. 1) were implemented and compared which operate on subtraction datasets obtained from radially sampled k-space acquisitions before and after needle placement. These subtraction data contain a distinct signature of the isolated needle artifact in image and k-space domain.8-10 Algorithm A1 (image-based) transforms the subtraction k-space data to image-space, using a NUFFT11. After thresholding the image to reduce streaking artifacts, an ellipsoid model is fitted to the data by performing a Principal Component Analysis (PCA). Algorithm A2 (k-space-based) models the k-space signature of the needle artifact as a 3D sinc function (corresponds to a cuboid in image-space, following Kochavi et al. who used a 2D sinc function for 2D k-space-based needle tracking in a phantom12). The model (Eq. 1) is fitted to the subtraction k-space using a downhill-simplex-method13.$$\begin{align}S(\vec{k},(X_0,Y_0,Z_0,\theta,\phi,l,w))&=\text{sinc}\left(\frac{w}{2\pi}\left(k_x*\hat{v}^\perp_{1,x}(\theta,\phi)+k_y*\hat{v}^\perp_{1,y}(\theta,\phi)+k_z*\hat{v}^\perp_{1,z}(\theta,\phi)\right)\right)\\&*\text{sinc}\left(\frac{w}{2\pi}\left(k_x*\hat{v}^\perp_{2,x}(\theta,\phi)+k_y*\hat{v}^\perp_{2,y}(\theta,\phi)+k_z*\hat{v}^\perp_{2,z}(\theta,\phi)\right)\right)\\&*\text{sinc}\left(\frac{l}{2\pi}\left(k_x*\hat{v}_{x}(\theta,\phi)+k_y*\hat{v}_{y}(\theta,\phi)+k_z*\hat{v}_{z}(\theta,\phi)\right)\right)\\&*\exp{\left(-i*(k_xX_0+k_yY_0+k_zZ_0)\right)}\end{align}$$
with S:k-space signal; (kx,ky,kz):k-space coordinates; (X0,Y0,Z0,θ,ϕ):needle center and angles as defined in Fig. 2b; (l,w):needle artifact width (fixed at 2px to simplify optimization) and length; v:unit vector along needle; v⊥1,2:unit vectors orthogonal to needle.
To evaluate the proposed localization algorithms, we simulated 3D radial subtraction k-space data of 300 needle artifacts by approximating them as cylinders in image space10 and applying a subsequent NUFFT (FOV=(256 cm)3,res=(4mm)3),(θ∈[-45°,45°],ϕ∈[-90°,90°),l∈[4 cm,8 cm]),radius $$$r=r_0*\sqrt[3]{\sin^2{\theta}}$$$ with r0=1px). Localization accuracy was evaluated for 5 (minimum spoke number to encode all degrees of freedom of the needle), 16 and 64 k-space spokes using metrics defined in Fig. 2c.
In a proof-of-principle experiment, k-space data of 4 example needle trajectories in an ex-vivo porcine phantom and a needle placed in a porcine in-vivo animal model was acquired with a 3D radial Golden-Angle14 FLASH sequence at B0=0.55T (MANGETOM Free.Max, Siemens Healthineers, Erlangen, Germany) using a head and surface coil (nspokes=6434 (fully-sampled and retrospectively cropped to 5, 16 and 64 spokes),TE=10ms,TR=12.5,flip angle=10°,bandwith=900Hz/px,FOV=(256cm)3,res=(4mm)3). A 22- and prototype 20-gauge aspiration needle (Cook Advanced Technologies, West Lafayette, IN, USA) were used. To determine ground truth position and orientation, the needle artifact was manually annotated in reconstructed 3D GRE images as shown in Fig. 2a (ex-vivo;in-vivo:TE=2.31ms;10ms,TR=13ms;12.5ms,flip angle=10°,bandwidth=1300Hz/px;900Hz/px,FOV=(256mm)3,res=(2mm)3;(4mm)3).
Results
Fig. 3 shows results of the simulation study. For localization using 64 spokes, image-based localization was outperformed by the k-space-based method (medians $$$\widetilde{{\Delta}s}$$$=3.6mm vs. $$$\widetilde{{\Delta}s}$$$=0.5mm). Using only 5 spokes, the image-based localization was more stable than the k-space-based method (medians $$$\widetilde{{\Delta}s}$$$=9.9mm vs. $$$\widetilde{{\Delta}s}$$$=39.1mm).Fig. 4 shows localization results for the sampled needle trajectories in the ex-vivo phantom and Fig. 5 for the in-vivo experiment. As for the simulation, localization generally improved for an increased number of spokes. For 64 spokes, ex-vivo localization accuracy was between Δs=2.6mm and Δs=9.2mm. In-vivo localization accuracy of Δs=4.3mm was achieved in (tacq+tloc)=1.1s.
Discussion
Using 64 k-space spokes, image- and k-space-based localization delivered fast and stable localization results in the simulation study and the in-vivo and ex-vivo experiments (compare CNN-based localization7: ex-vivo accuracy 10.8mm in ~1s), which enabled ASP as retrospectively demonstrated. Imperfect suppression of streaking artifacts in reconstructed images, which are not accounted for by the image-based (ellipsoid) model, might be the reason for the better performance of the k-space-model for localization using 64 spokes in the simulation study. High median localization errors for fewer spokes (5 and 16), however, also indicate a higher optimization failure rate of the k-space-based localization, possibly due to local minima in the optimization surface. A possible dependency of the optimization success on the needle orientation must be investigated in future work.Motion during localization or between acquisition of baseline and needle localization, e.g., due to breathing, poses a limitation as it could possibly result in a corrupted subtraction k-space. This might be mitigated by using motion compensated imaging strategies (e.g., breath hold, multi baseline imaging).
Conclusion
Model-based rapid 3D needle localization was successfully demonstrated in simulations, ex-vivo phantoms, and a porcine in-vivo model. The proposed methods could be used to improve the workflow of MR-guided needle interventions by enabling fast automatic slice alignment.Acknowledgements
We thank Sean Chambers (Cook Advanced Technologies) for his support in the abstract release process.References
- Veltri et al. CIRSE Guidelines on Percutaneous Needle Biopsy (PNB). Cardiovasc Intervent Radiol. 2017;40(10):1501-1513.
- Weiss et al. MR-guided biopsy: A review of current techniques and applications. J Magn Reson Imaging. 2008;27(2):311-325.
- De Oliveira et al. Automatic passive tracking of an endorectal prostate biopsy device using phase-only cross-correlation. Magn Reson Med. 2008;59(5):1043-1050.
- Reichert et al. Passive needle guide tracking with radial acquisition and phase‐only cross‐correlation. Magn Reson Med. 2021;85(2):1039-1046.
- Zijlstra et al. SMART tracking: Simultaneous anatomical imaging and real-time passive device tracking for MR-guided interventions. Phys Med. 2019;64:252-260.
- Li et al. Physics-Driven Mask R-CNN for Physical Needle Localization in MRI-Guided Percutaneous Interventions. IEEE Access. 2021;9:161055-161068.
- Faust et al. Fast 3D Passive Needle Localization for MR-Guided Interventions using Radial White Marker Acquisitions and CNN Postprocessing. In: Proceedings of the 31st Annual Meeting of ISMRM. 2022. p 1196.
- Ladd et al. Biopsy needle susceptibility artifacts. Magn Reson Med. 1996;36(4):646-651.
- Posse and Aue. Susceptibility Artifacts in Spin-Echo and Gradient-Echo Imaging. J Magn Reson. 1990;88(3):473-492.
- Faust et al. Analytical estimation of artifact radius for an MR-compatible aspiration biopsy needle. In: 6th Conference on Image-Guided Interventions. 2023. p 65-67.
- Ong and Lustig. SigPy: a python package for high performance iterative reconstruction. In: Proceedings of the 27th Annual Meeting of ISMRM. 2019. p 4819.
- Kochavi et al. Method for rapid MRI needle tracking. Magn Reson Med. 2004;51(5):1083-1087.
- Virtanen et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nature Methods. 2020;17(3):261-272.
- Chan et al. Temporal stability of adaptive 3D radial MRI using multidimensional golden means. Magn Reson Med. 2009;61(2):354-363.
Figures
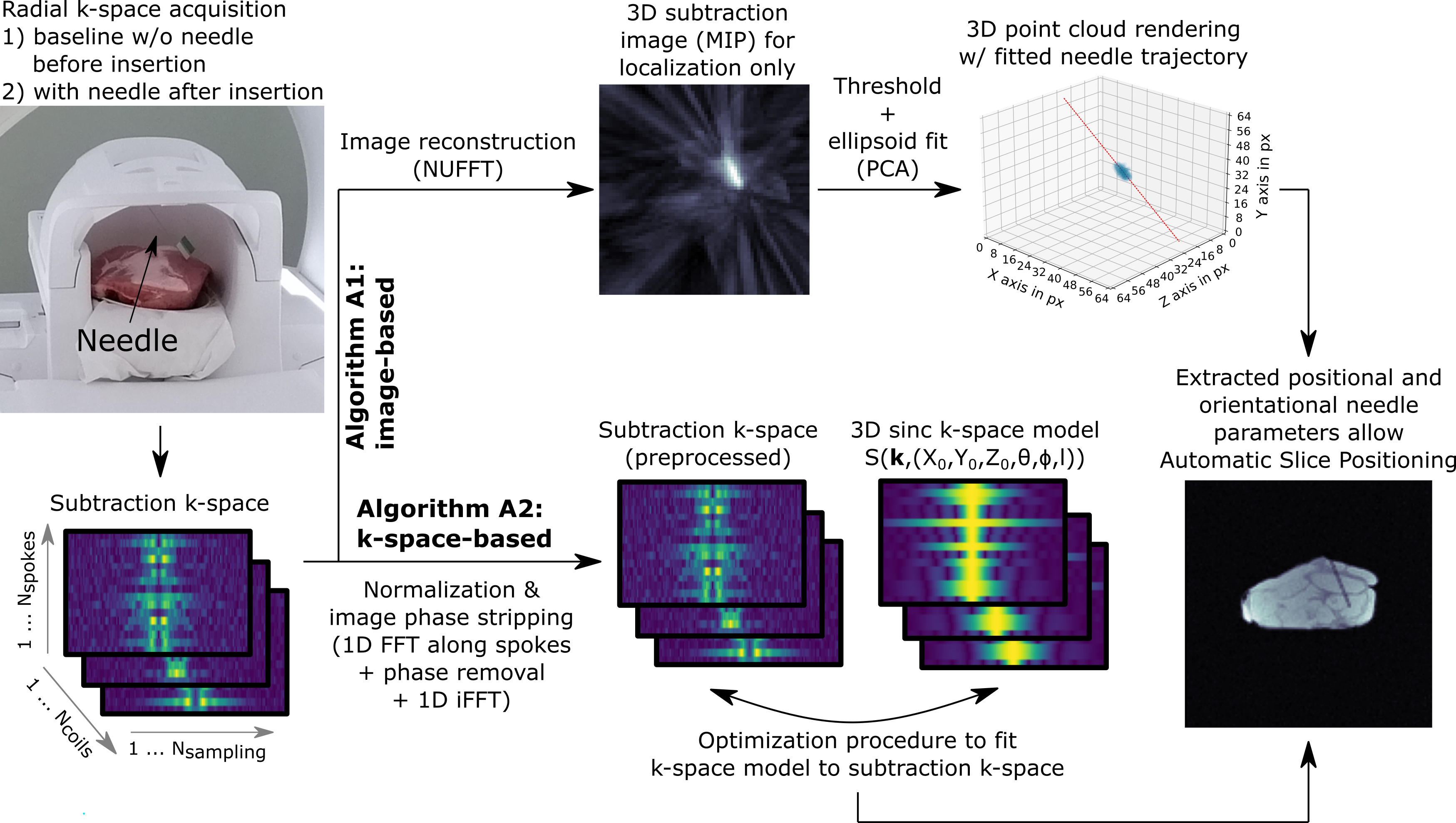
Figure 1: Two algorithms for model-based needle localization. Algorithm A1 (image-based): image is reconstructed from the subtraction k-space and thresholded (>70% of maximum image intensity), and an ellipsoid model (PCA) is fitted to the data. Algorithm A2 (k-space-based): k-space is directly modeled with a 3D sinc function following Eq. 1 and the model is fitted to the normalized and image phase-stripped data. Successful needle localization allows to automatically align a 2D imaging slice with the needle.
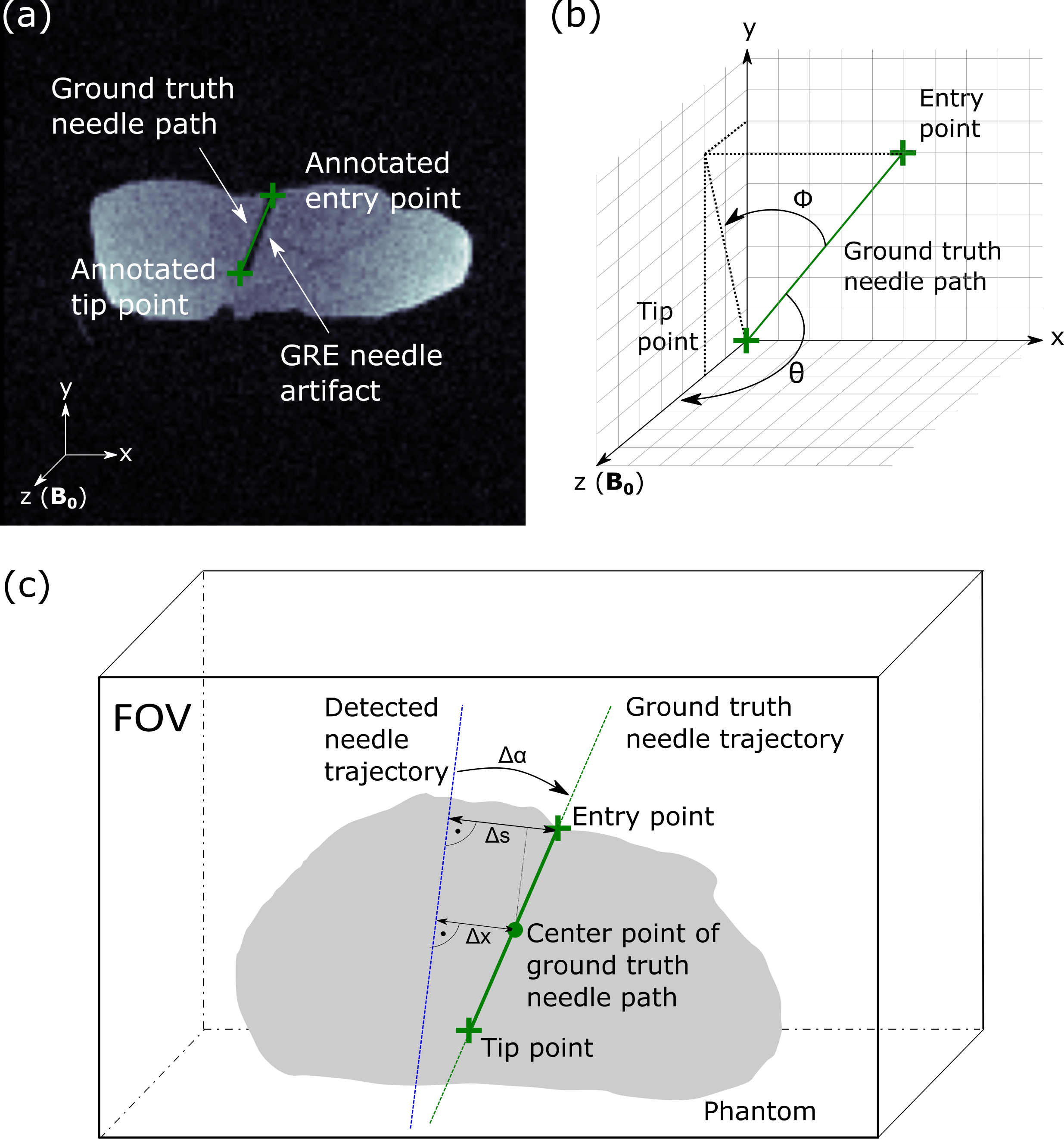
Figure 2: (a) 2D slice from 3D GRE reference image of (example) ex-vivo phantom with needle placement. Needle tip and entry point were annotated manually in 3D for ground truth needle path extraction. (b) Needle orientation characterized by angle θ to B0 and angle ϕ to zy/sagittal plane. (c) Measures for evaluation of localization: Δx is center distance, Δα is angular deviation, and Δs is maximum distance between ground truth needle path and detected needle trajectory.
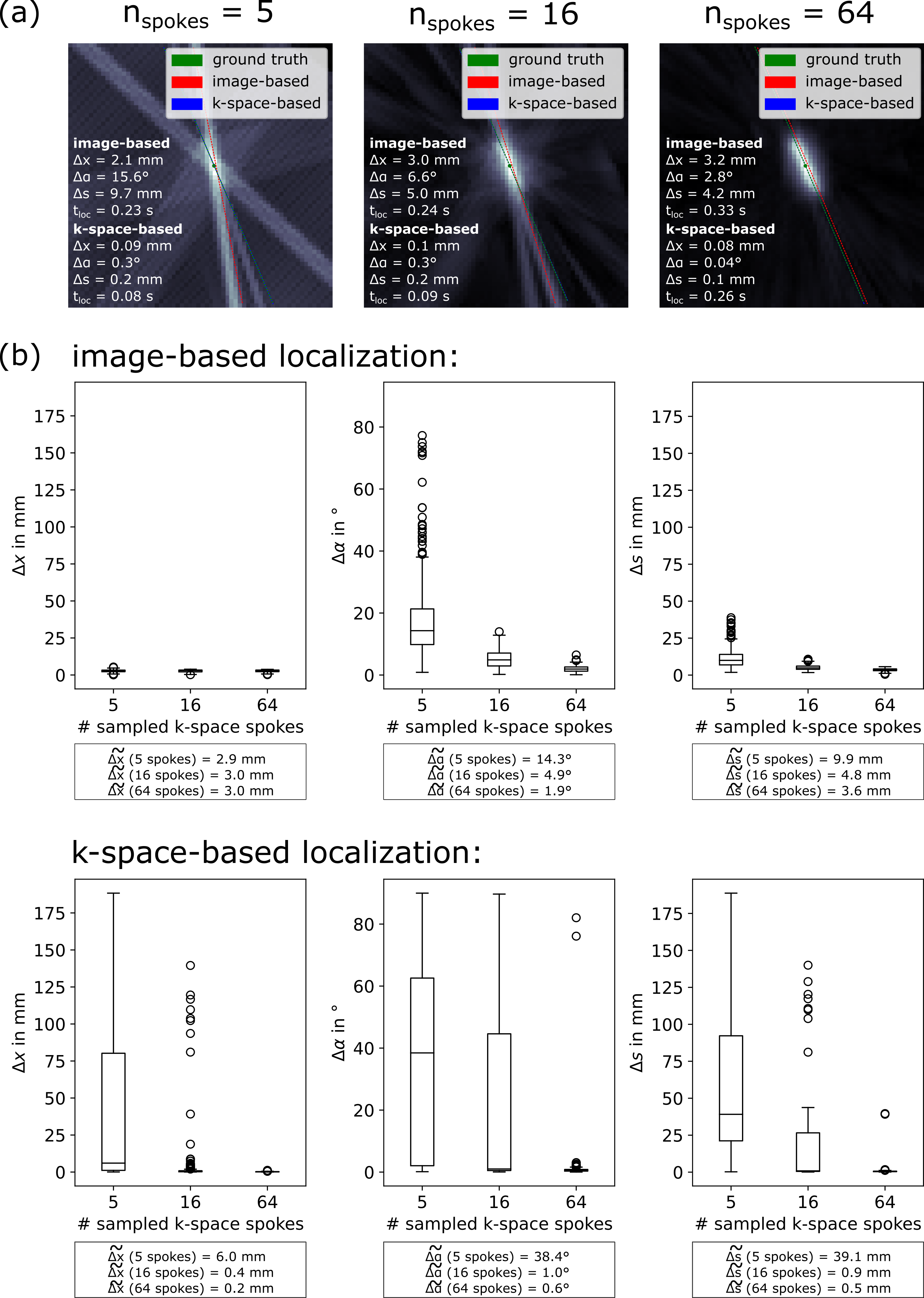
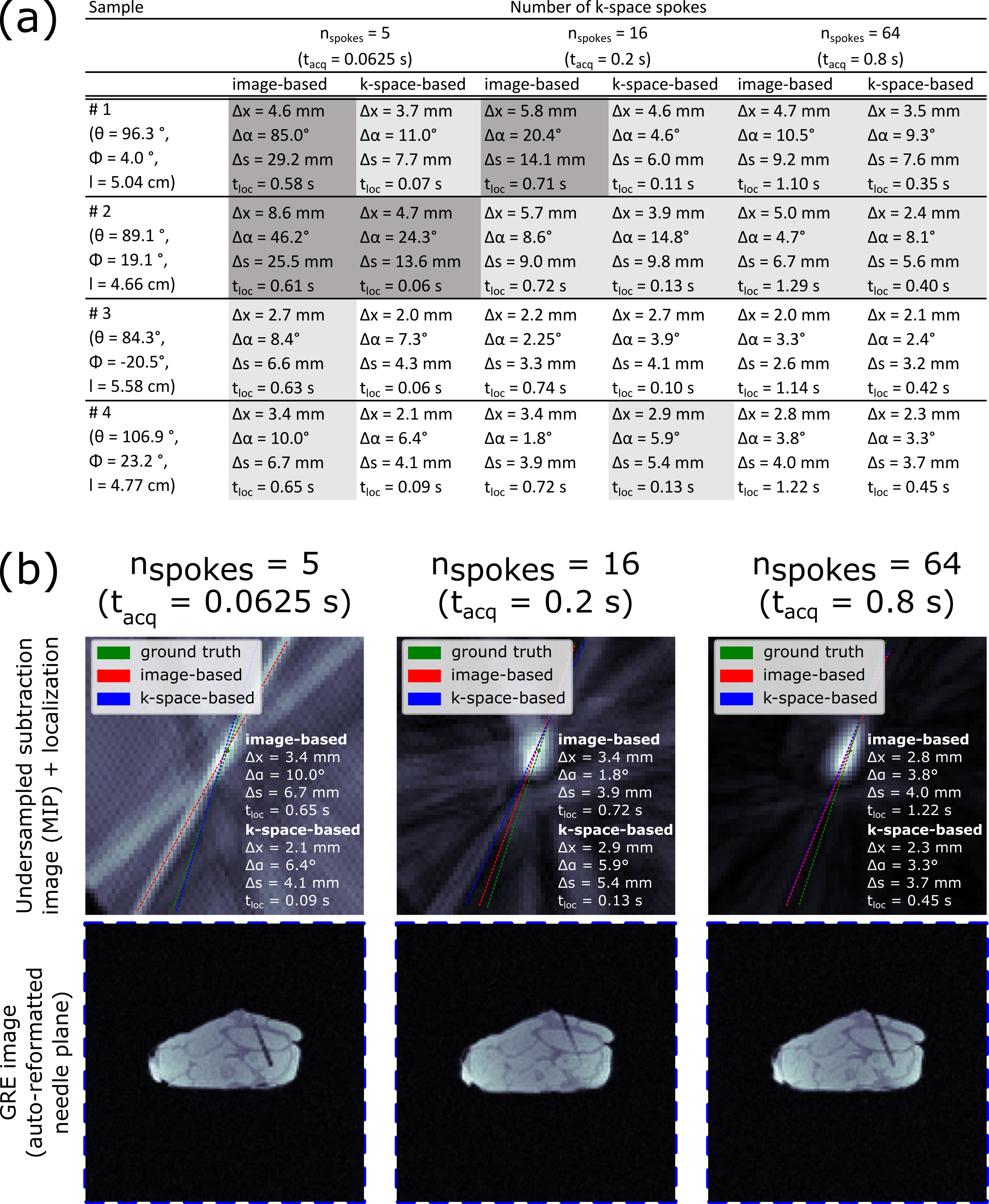
Figure 4: (a) Localization accuracy for 4 example needle trajectories in ex-vivo phantom. Table is color-coded for Δs: white ≙ (5 mm > Δs); light grey ≙ (10 mm > Δs ≥ 5 mm); dark grey ≙ (Δs ≥ 10 mm). (b) For trajectory #4, images were reconstructed from 5, 8, and 64 spokes (acquisition time: tacq). Dashed lines display determined needle trajectory. Based on k-space-based localization, a 2D slice (thickness: 4 mm) was retrospectively positioned in an acquired 3D GRE image of the needle placement.
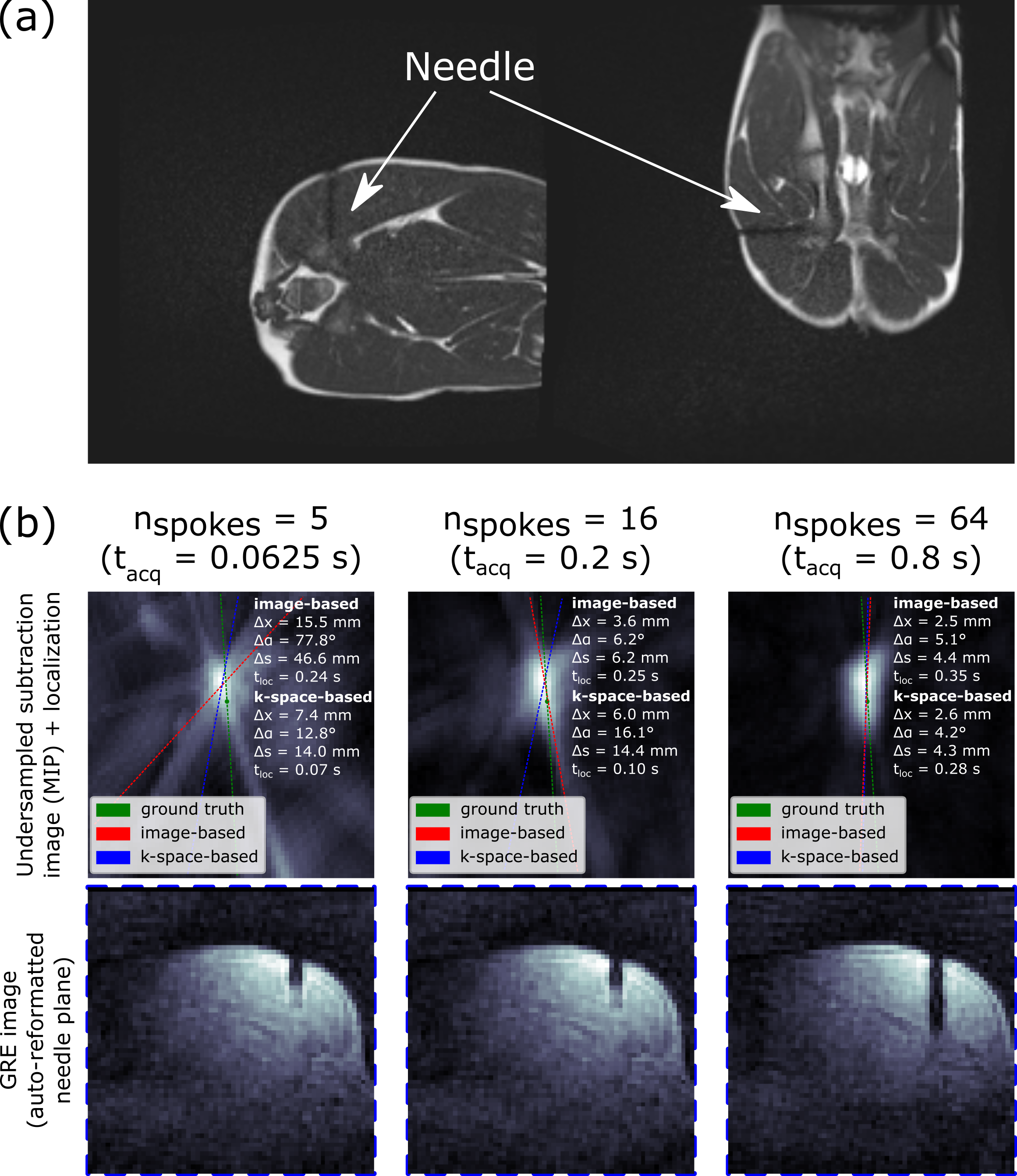
Figure 5: In-vivo needle placement in porcine thigh. (a) Overview bSSFP images, manually aligned with needle. (b) Automatic rapid 3D needle localization. Columns show reconstructed images from 5, 8, and 64 spokes with ground truth and determined needle trajectories from the two investigated algorithms (dashed lines). Based on the k-space-based localization, a slice (thickness: 4 mm) containing the needle artifact was retrospectively positioned in an acquired 3D GRE image of the biopsy.