0454
Capturing Internal Target Motion with Breathing Variability Using 3D Dynamic Lung MRI1Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 2Siemens Medical Solutions USA Inc, Baltimore, MD, United States, 3Robin Medical Inc., Baltimore, MD, United States, 4Radiation Oncology, University of Maryland School of Medicine, Baltimore, MD, United States
Synopsis
Keywords: MR-Guided Radiotherapy, Hybrid & Novel Systems Technology, Breathing variability
Motivation: To develop an MRI technique that captures cycle-to-cycle variability and differential motion between inhalation and exhalation to enable more accurate treatment planning and real-time beam adaptation.
Goal(s): To address the challenge of acquiring sufficient volumetric data for reconstruction of 3D dynamic lung MRI while maintaining adequate spatiotemporal resolution for radiation therapy guidance.
Approach: We utilized golden angle stack-of-star acquisition and labeled each view with the breathing state captured by a surface tracking system for sharing views with similar breathing states.
Results: 3D dynamic lung imaging captured cycle-to-cycle variability and respiratory hysteresis with a nominal temporal resolution of 60.6ms per volume.
Impact: The 3D dynamic lung imaging captured cycle-to-cycle variability and respiratory hysteresis with a nominal temporal resolution of 60.6ms. It can provide more accurate motion information than 4D-MRI for radiotherapy guidance, avoiding interplay between the tumor target and organs at risk.
INTRODUCTION
Radiation therapy (RT) aims to deliver a lethal dose of ionizing radiation to the tumor while minimizing dose to surrounding healthy tissues and organs at risk (OARs). Achieving this goal is especially challenging in the treatment of thoracic tumors with respiratory motion-induced geometric uncertainties in dose delivery. 4D-MRI has been investigated in MRI-guided RT to inform treatment planning and online treatment adaptation in thoracic RT. A common limitation of current 4D-MRI techniques is that they do not address cycle-to-cycle variability1 or respiratory hysteresis, i.e., differential motion between inhalation and exhalation2, causing interplay between the tumor target and OARs.3D dynamic imaging of the lungs can address both issues to enable more accurate treatment planning and real-time beam adaptation. To address the challenge of acquiring sufficient volumetric data while maintaining adequate spatiotemporal resolution for RT guidance, we utilize golden angle stack-of-star acquisition and label each view with the breathing state captured by a research MR-compatible surface tracking system, EndoScout II (Robin Medical Inc.). This approach allows for reconstruction at any time point with view sharing of k-space data acquired within similar breathing states.
METHODS
MR acquisitionSiemens product 3D volumetric stack-of-stars GRE (starVIBE) sequence was modified to enable radial acquisition with golden angle views. The scan parameters were TE/TR=1.27/2.92ms, FOV=320mm, matrix size 192x192, 8 sagittal slices, slice thickness 3mm, 4000 views, and acquisition time of 2min. A tracking-activation module (2.2ms) was inserted to produce one tracking data point every two views (60.6ms).
For comparison, the same volume was also imaged with a Siemens prototype 4D-MRI sequence with 5 bins (acquisition time of 1min41sec and similar parameters as above). A dynamic 2D single-slice FLASH was acquired at the center slice of the 3D volume (TE/TR=2.2/4.5ms, FOV=320mm, matrix size 128x128, slice thickness 6mm, 3x GRAPPA, 300 dynamics and total acquisition time of 58sec).
MRI was acquired on four healthy volunteers (3M/1F, age: 30±2.3 years) in the right lung using a Siemens PrismaFIT 3T scanner with two 18-channel body array coils. Subjects were instructed to breathe regularly during acquisition. Sensors for surface motion tracking were placed diagonally across the thoraco-abdominal surface (Fig. 1).
Image reconstruction
Principal component analysis (PCA) was performed on measurements from the four sensors. The breathing state of a radial view was represented by the scores corresponding to the first three principal components. Views acquired with similar breathing states were used to fill the k-space. Under-sampled reconstruction was performed with The Berkeley Advanced Reconstruction Toolbox (BART)3 using sensitivity maps estimated from the entire acquisition with ESPIRiT4. For a target volume during breath-in/breath-out, view sharing was limited to k-space data acquired within the breath-in/breath-out phase.
RESULTS
Figure 2 shows an example breathing motion for one volunteer in the anterior-posterior (AP) direction captured by the four surface tracking sensors (Fig. 1). The maximum AP motion captured by sensor 1 to 4 increased from less than 2mm to 10mm, showing larger surface motion in the abdominal region that in the thoracic region. The cycle-to-cycle variability was evident. Measurements were divided into breath-in (green) and breath-out (red) phases for subsequent view sharing.Figure 3 shows dynamic 3D volumes at four phases: end-of-exhalation (EOE), end-of-inhalation (EOI), and midway during breath-in and breath-out. The target points for breath-in and breath-out volumes were selected to have the same AP location measured by sensor 3 (Fig. 3A) but different as measured by the other three sensors. The diaphragm in the breath-out volume was slightly higher than in the breath-in volume showing a single measurement is not sufficient to describe the breathing state. The sharpness of the diaphragm in the dynamic 3D images was comparable to the 5-bin 4D (center column) and the FLASH (right column) images.
Five EOI and EOE time points were selected based on the AP location measured by sensor 3 (Fig. 4A). EOI 1 to 5 showed increasingly lower diaphragm positions (Fig. 4B, C), matching increasingly anterior surface locations captured by sensor 3. EOE 1 to 5 showed increasingly higher diaphragm positions (Fig. 4D, E), matching increasingly posterior surface locations captured by sensor 3.
DISCUSSION
3D dynamic lung imaging in this work demonstrated its ability to capture the anatomical difference between breath-in and breath-out as well as cycle-to-cycle variability. A volume can be reconstructed centered at any given tracking point with a nominal temporal resolution of 60.6ms, or 66 volumes per breathing cycle.CONCLUSION
We demonstrate the feasibility of capturing internal motion using dynamic 3D lung MR imaging with an MR-compatible surface tracking system. This method can provide more accurate motion information than single-cycle 4D-MRI for lung cancer radiotherapy.Acknowledgements
The study was conducted at University of Maryland School of Medicine Center for Innovative Biomedical Resources, Translational Research in Imaging @ Maryland (CTRIM) – Baltimore, Maryland. The study is supported by NIH under grant 5R01CA262017.
References
1. Lockwood MD, Degenhardt BF. Cycle-to-cycle variability attributed to the primary respiratory mechanism [published correction appears in J Am Osteopath Assoc. 1998 Mar;98(3):137]. J Am Osteopath Assoc. 1998;98(1):35-43.
2. White B, Zhao T, Lamb J, et al. Distribution of lung tissue hysteresis during free breathing. Med Phys. 2013;40(4):043501. doi:10.1118/1.4794504
3. BART Toolbox for Computational Magnetic Resonance Imaging, DOI: 10.5281/zenodo.592960
4. Uecker M, Lai P, Murphy MJ, et al. ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med. 2014;71(3):990-1001. doi:10.1002/mrm.24751
Figures
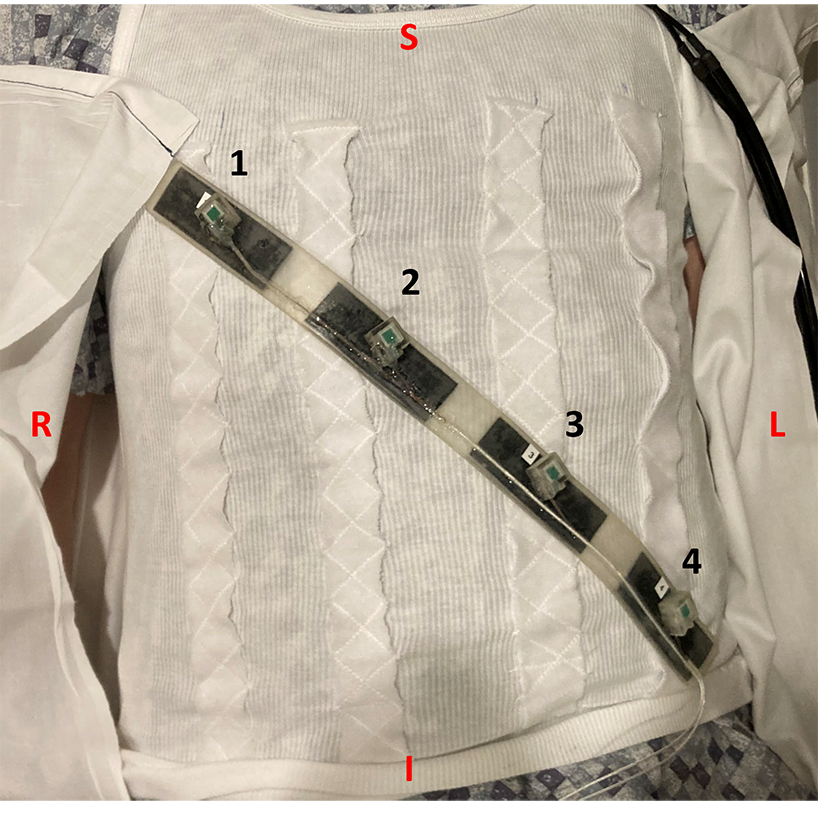
Figure 1. Placement of four tracking sensors (1, 2, 3, 4) that cover both the chest and the abdomen. The coverage ensures the breathing motion can be captured whether the subject uses chest breathing or abdominal breathing. S: superior, I: inferior, R: right, L: left.
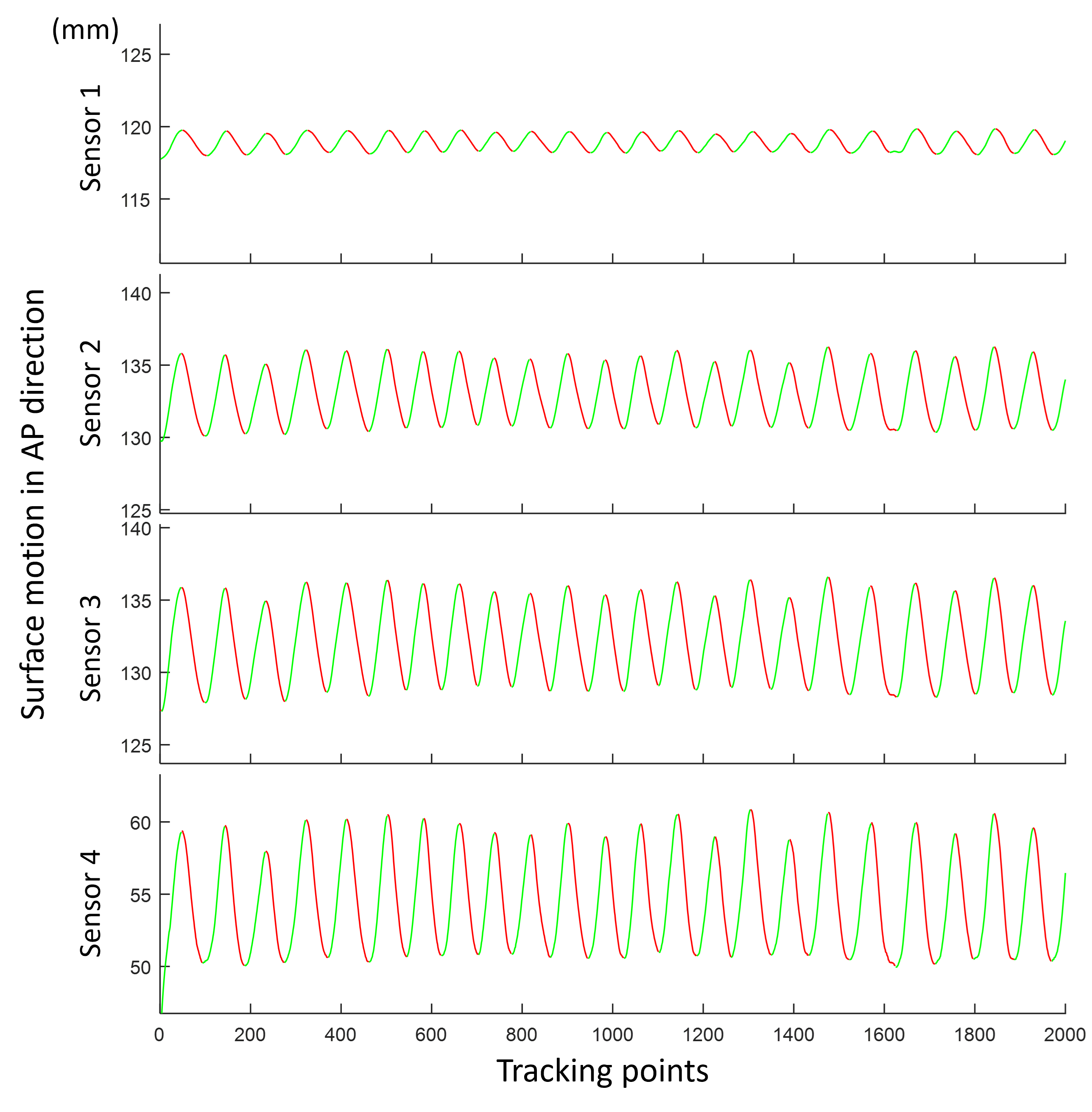
Figure 2. Breathing motion in the AP direction from four surface tracking sensors for the example case. Sensors 1 to 4 were placed diagonally from the right chest to the left lateral abdomen as shown in Fig. 1. Each measurement was divided into breath-in (green) and breath-out (red).
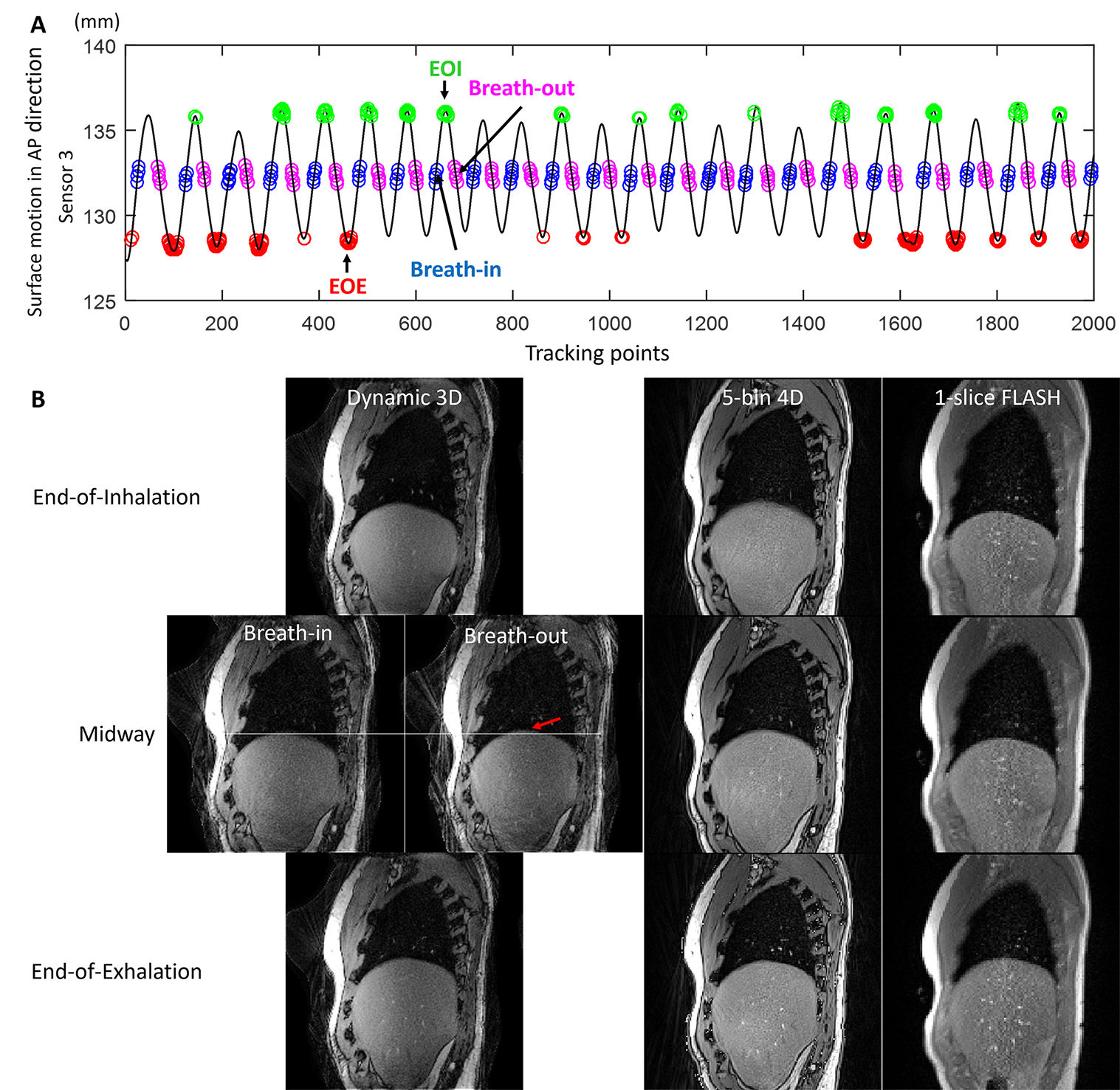
Figure 3. A. Target time points for four volumes, End-of-Exhalation (EOE), Breath-in, Breath-out, and End-of-Inhalation (EOI) (pointed to by arrows) and the tracking points from which k-space lines were shared for the four volumes, EOE (red), Breath-in (blue), Breath-out (magenta), and EOI (green) B. EOI, midway, and EOE volumes from dynamic 3D (left), 5-bin 4D (middle), and single-slice FLASH (right). Breath-in and Breath-out volumes were reconstructed from a breath-in and a breath-out tracking point with the same surface location in the AP direction as measured by sensor 3.
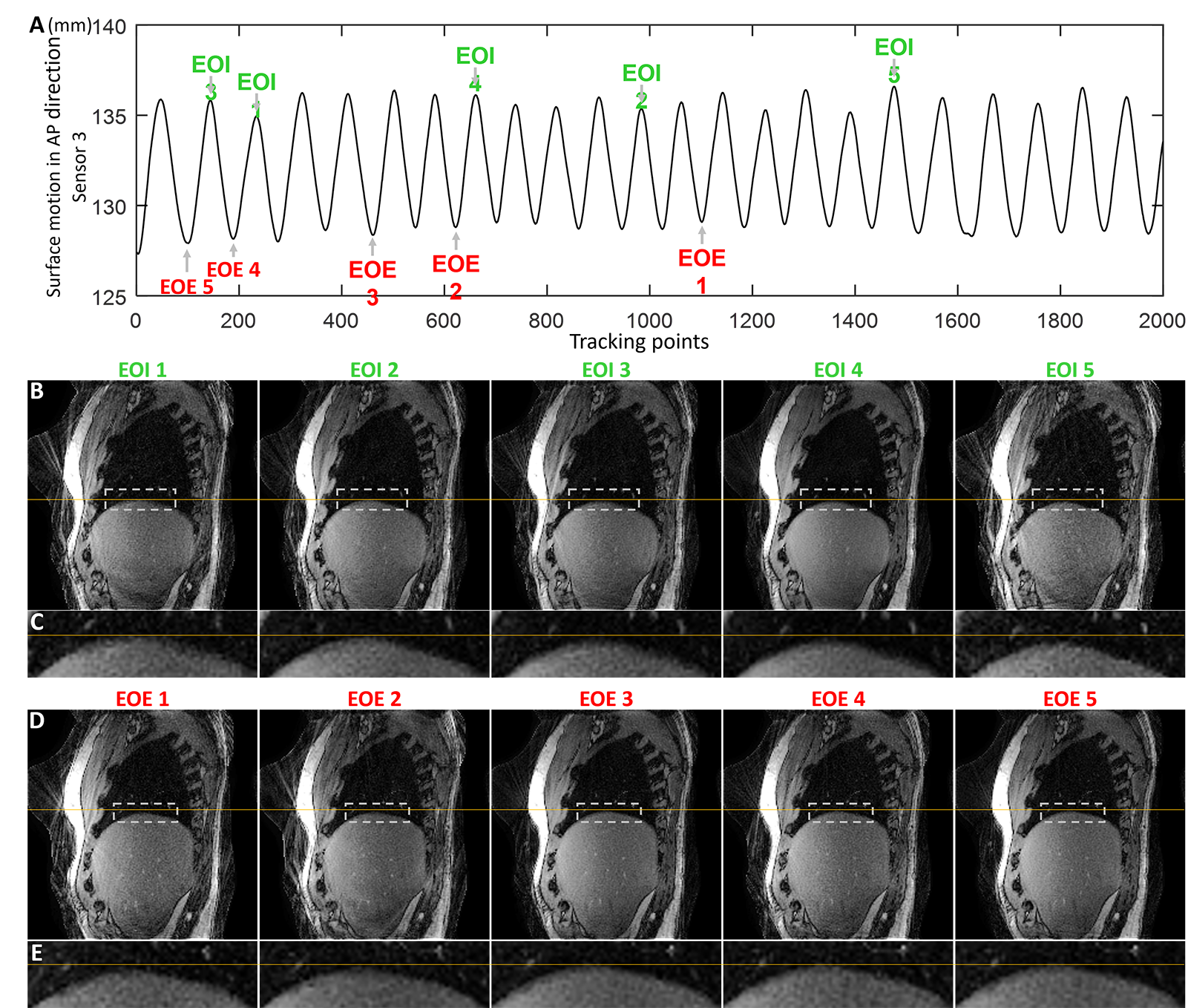
Figure 4. End-of-Inhalation (EOI) (B, C) and End-of-Exhalation (EOE) (D, E) volumes in multiple breathing cycles with different breathing states (illustrated by AP measurement from sensor 3 in A). EOI 1 to 5 have increasingly anterior surface positions as measured by sensor 3, and EOE 1 to 5 have increasingly posterior surface positions as measured by sensor 3 (A). The zoomed-in figures C and E show the areas marked by gray dashed rectangles in B and D, respectively. Yellow horizontal lines in B, C and D, E are aligned with the top of the diaphragm in EOI 1 and EOE 5, respectively.