0452
4D Lung MRI with Isotropic Resolution on a 1.5T MR-Linac using a Self-Navigated 3D Radial Kooshball Acquisition and Sparse Motion Reconstruction1Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
Keywords: Lung, Lung, 4D MRI, MR-Linac, Motion, Radiotherapy, Radial
Motivation: Current 4D MRI methodology on the MR-Linac is based on stack-of-stars acquisition, which has limited resolution along the slice dimension and can compromise the performance of motion assessment.
Goal(s): To develop 4D lung MRI with isotropic-resolution on a 1.5T MR-Linac using 3D radial kooshball acquisition with respiratory self-navigation.
Approach: Stack-of-stars and kooshball acquisitions were performed on a healthy volunteer. Motion-resolved 4D MRI was reconstructed using XD-GRASP and then compared in terms of image quality and motion characteristics.
Results: Stack-of-stars acquisition underestimated motion due to limited resolution in the slice dimension. Kooshball acquisition provided isotropic-resolution that allows for improved visualization of smaller pulmonary structures.
Impact: 4D MRI with isotropic spatial resolution has the potential to enhance treatment planning and adaptation for lung cancer patients receiving radiation therapy on the MR-Linac system.
INTRODUCTION
4D MRI is a powerful alternative to 4D CT for radiotherapy planning of tumors affected by respiratory motion, removing exposure to ionizing radiation and enabling longer scans for improved characterization of motion1. Moreover, 4D MRI can be implemented on MR-Linac systems for treatment adaptation during each fraction2. Current 4D MRI technology on the MR-Linac is based on the stack-of-stars acquisition (radial kx-ky and Cartesian kz)2,3, which limits resolution along the z dimension and results in anisotropic resolution, particularly for regions that require a large coverage such as the lungs. To address this issue, combinations of 3D radial kooshball acquisition and compressed sensing reconstruction have been demonstrated for 4D lung MRI with high isotropic spatial resolution on 3T MRI scanners4,5. This work develops a 4D lung MRI with isotropic spatial resolution on the 1.5T MR-Linac system using a self-navigated 3D radial kooshball acquisition and compressed sensing reconstruction for radiotherapy planning and adaptation.METHODS
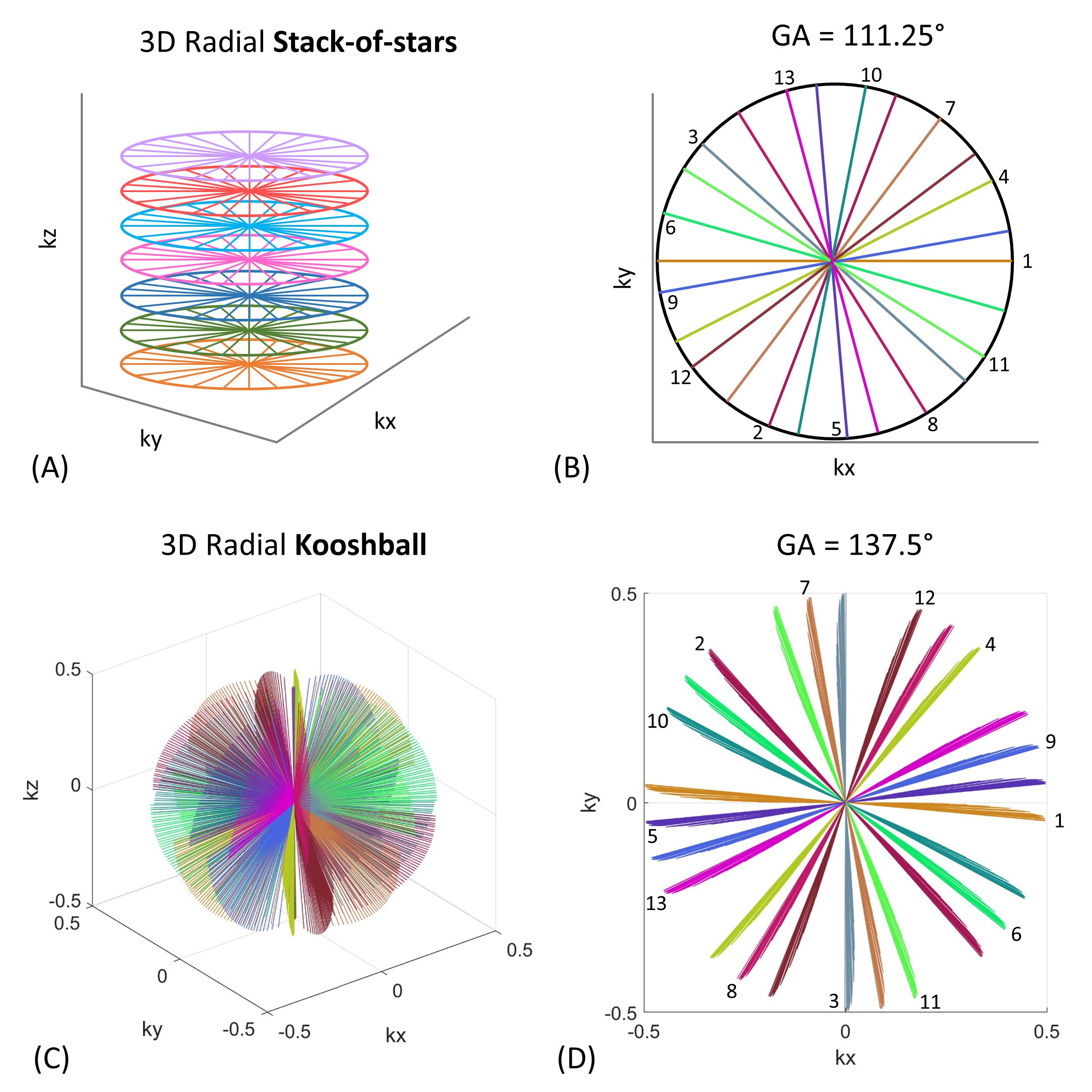
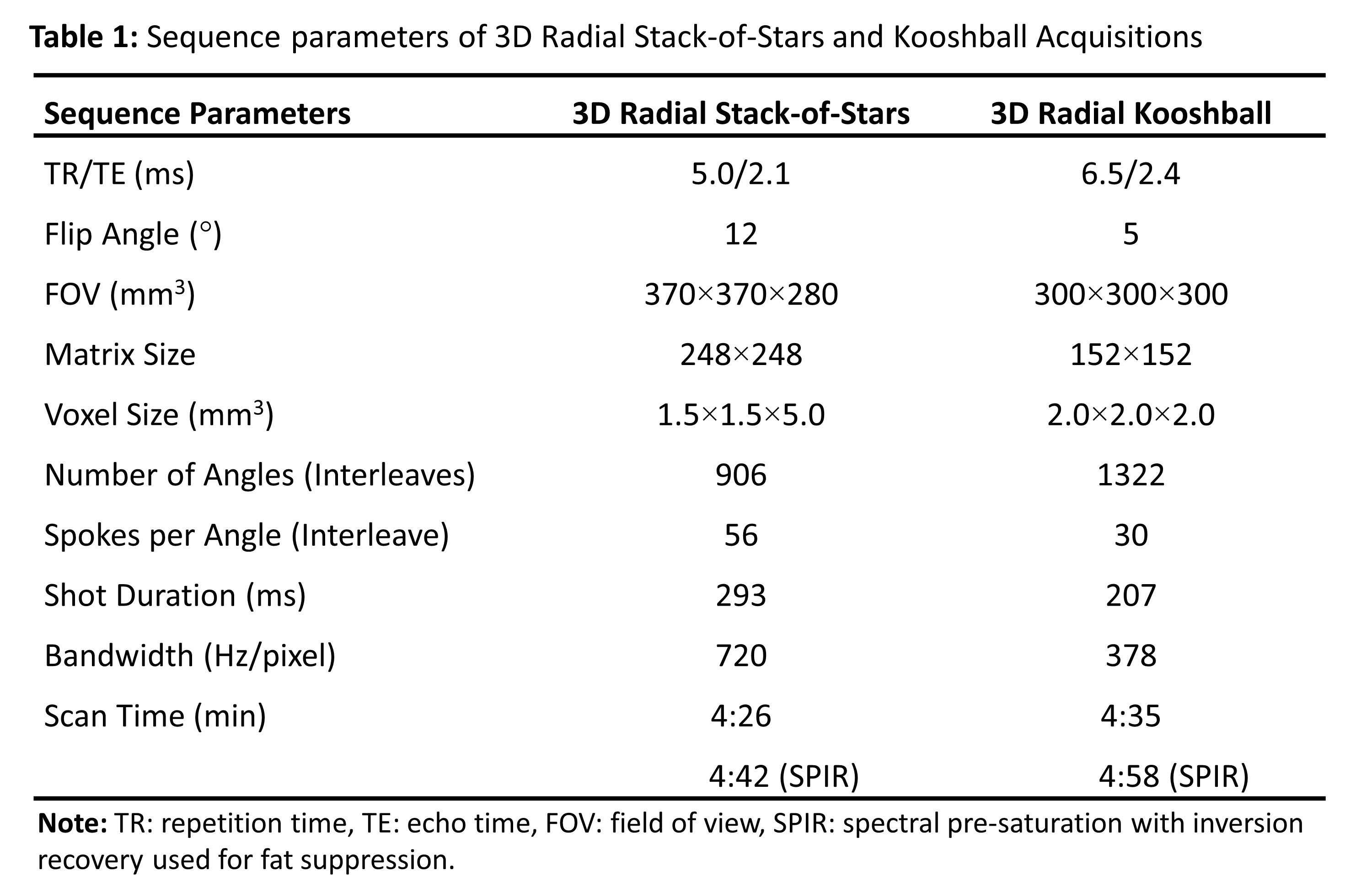
k-space trajectories: Figure 1 illustrates the k-space trajectories of 3D radial stack-of-stars and kooshball acquisitions. The latter was implemented based on the VASP sequence6. The radial spokes between two consecutive stacks or interleaves are ordered by the golden-angle, i.e., 111.25° for stack-of-stars and 137.5° for kooshball acquisitions, respectively.Data acquisition: This feasibility study included a healthy volunteer (male, 40 years). Free-breathing lung imaging with stack-of-stars and kooshball acquisitions were performed on a 1.5T Unity MR-Linac (Elekta AB, Stockholm, Sweden). Table 1 shows the detailed sequence parameters used for data acquisitions. Additionally, two extra acquisitions were performed using spectral pre-saturation with inversion recovery (SPIR) to assess the effect of fat suppression on image quality.
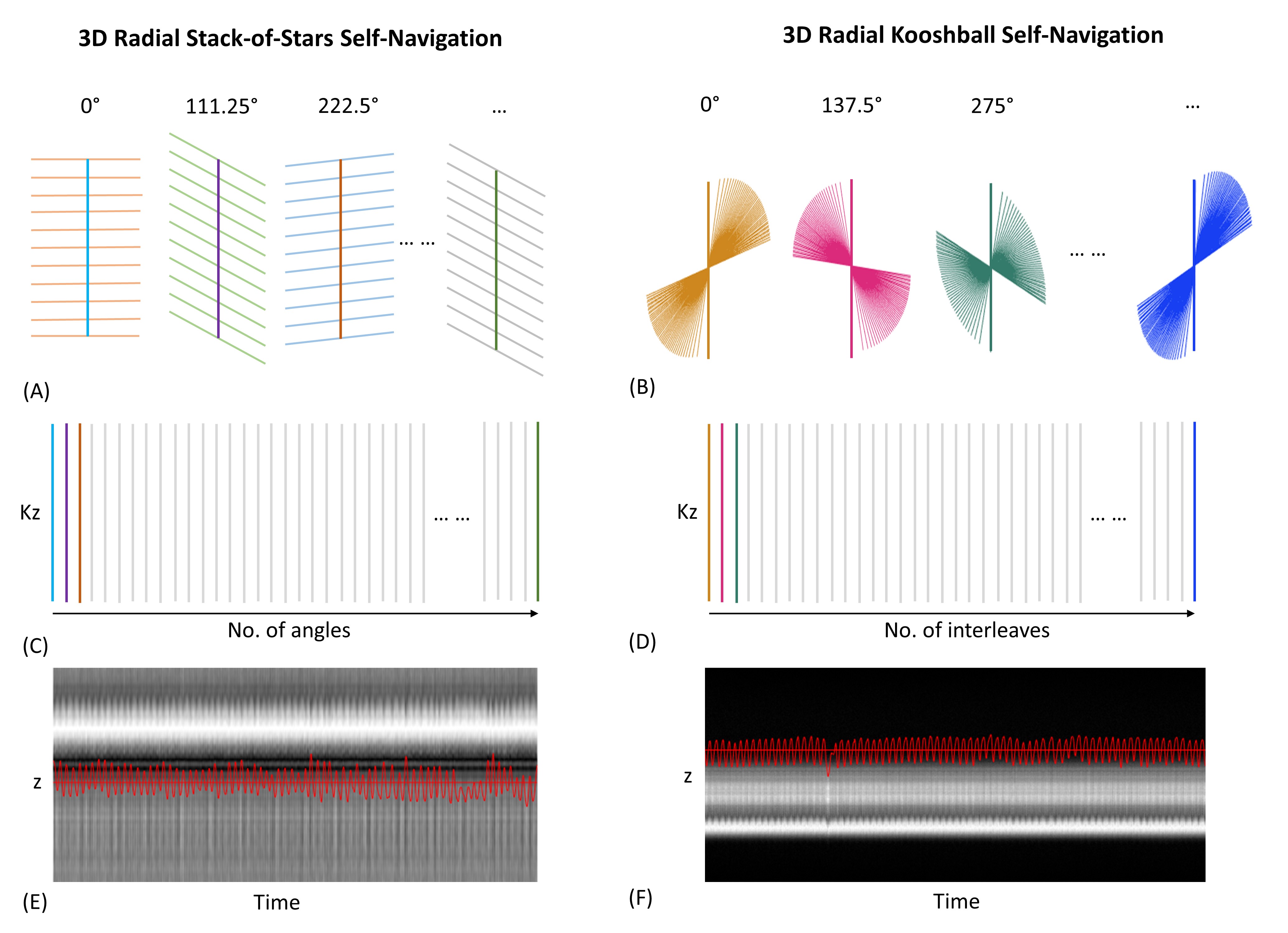
Self-navigation: The center line (kx=ky=0) of each stack along kz (stack-of-stars) or the first line along kz for each interleave (kooshball) are stacked sequentially. This provides self-navigation of diaphragm motion, which serves as a surrogate for respiratory motion. Figure 2 illustrates that the respiratory motion signals are computed from the stacked kz lines using a motion detection algorithm which combines principal component analysis (PCA), lowpass filtering, and coil clustering4,7.
4D MRI reconstruction: The k-space data was sorted and binned into 10 motion states using the respiratory motion signals calculated from self-navigation. Motion-resolved 4D MRI was reconstructed using XD-GRASP7, which exploits temporal sparsity along the motion states.
Motion evaluation: The motion was estimated by measuring the maximum displacement (mm) of the diaphragm from the end-expiration to the end-inspiration.
RESULTS
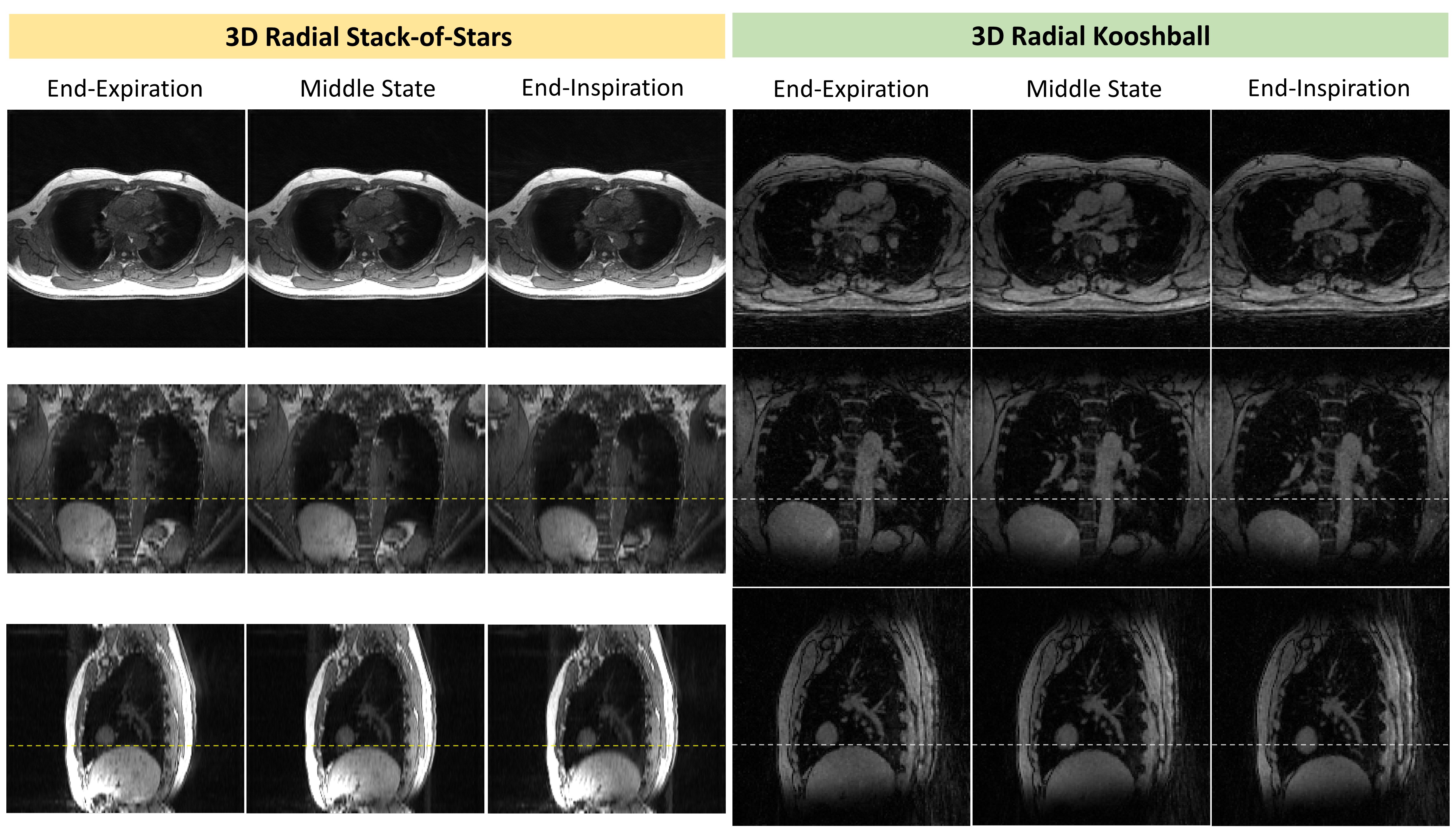
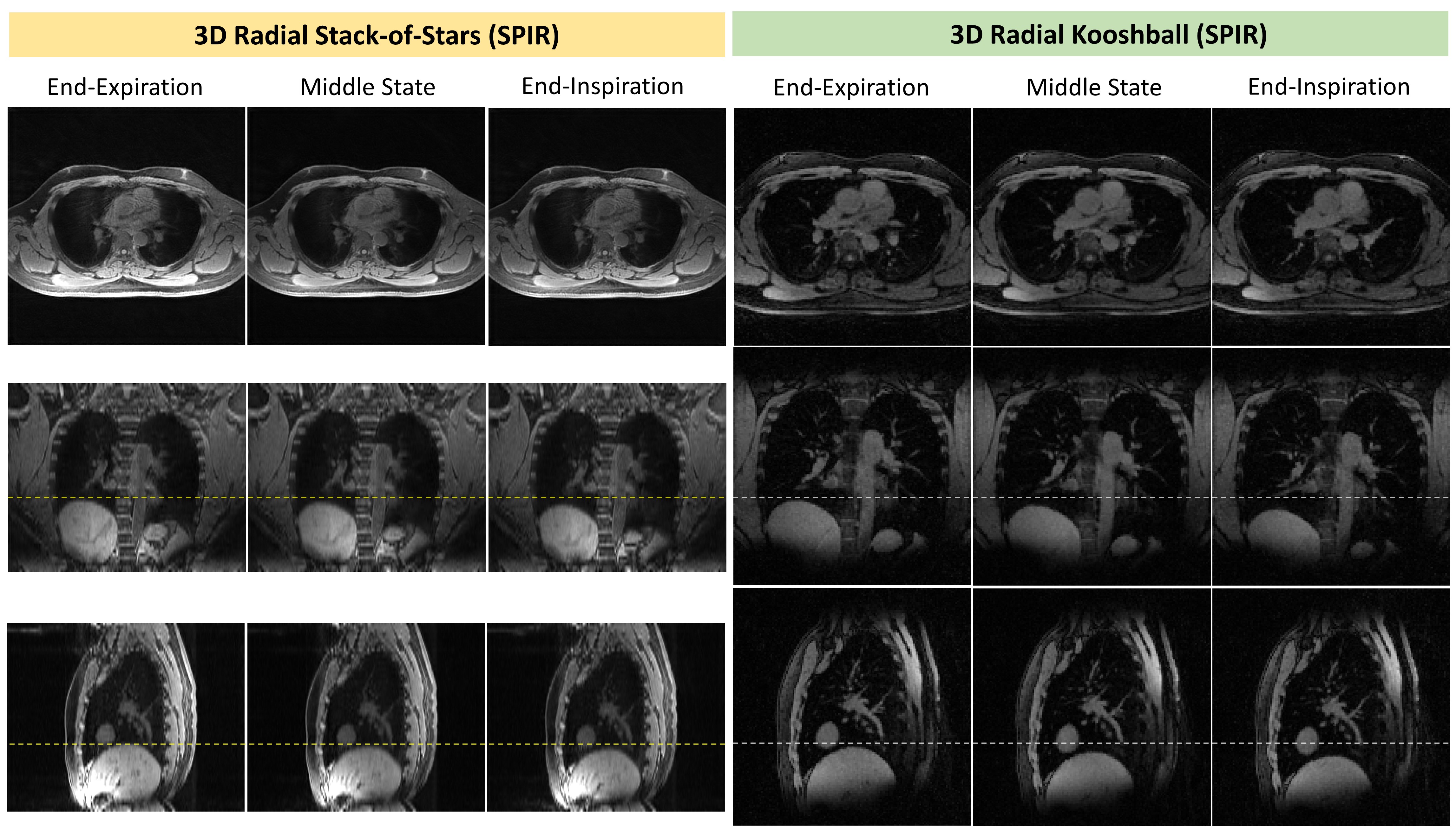
4D images for stack-of-stars and kooshball acquisitions are shown in Figure 3 (without fat suppression) and Figure 4 (with fat suppression). Both cases clearly show the motion of the diaphragm, but the kooshball acquisition provides more detailed visualization of smaller pulmonary structures compared to the stack-of-stars acquisition. This is primarily because the kooshball acquisition has a higher resolution along the z direction (2mm versus 5mm). The pulmonary structures appear similar between the 4D MRI images with and without using fat suppression. However, when SPIR was used, the subcutaneous fat signal was significantly suppressed (Figure 4). This suppression contributed to a cleaner background with fewer streaking artifacts. In addition, the motion of the diaphragm was measured to be 8.8mm and 9.6mm for 4D MRI with stack-of-stars and kooshball acquisitions, respectively. This measurement remained consistent whether fat suppression was used or not.DISCUSSION
The motion measured with stack-of-stars acquisitions tended to be underestimated, partially because of insufficient spatial resolution in the z direction. In addition, kooshball acquisitions provide isotropic resolution and thus improve visualization of smaller pulmonary structures compared to stack-of-stars acquisitions. Fat suppression is effective in reducing subcutaneous fat signals and minimizing streaking artifacts with only a minor increase of the total scan time. By using SPIR instead of SPAIR for fat suppression, the acquisition time for each stack (stack-of-stars) or interleave (kooshball) is reduced, making data acquisition more efficient. To further improve the speed of 4D lung MRI, a deep learning-based model can be used to simultaneously accelerate data acquisition and image reconstruction. For instance, Movienet provides 2-fold acquisition acceleration and sub-second 4D MRI reconstruction8.CONCLUSION
This work demonstrates the feasibility of conducting isotropic-resolution 4D MRI using 3D radial kooshball acquisition and respiratory self-navigation on a 1.5T MR-Linac system. The motion information acquired from 4D lung MRI has significant potential to enhance the precision of treatment planning and monitoring for lung cancer patients receiving treatment on the MR-Linac system.Acknowledgements
The work was supported by NIH Grant R01-CA255661.References
1. Perkins T, Lee D, Simpson J, et al. Experimental evaluation of four-dimensional magnetic resonance imaging for radiotherapy planning of lung cancer. Phys Imaging Radiat Oncol 2021; 17:32-35.
2. Paulson E, Ahunbay E, Chen X, et al. 4D-MRI driven MR-guided online adaptive radiotherapy for abdominal stereotactic body radiation therapy on a high field MR-Linac: Implementation and initial clinical experience. Clin Transl Radiat Oncol 2020; 23:72-79.
3. den Boer D, Veldman J, van Tienhoven G, et al. Evaluating differences in respiratory motion estimates during radiotherapy: a single planning 4DMRI versus daily 4DMRI. Radiat Oncol 2021; 16(1):188.
4. Feng L, Delacoste J, Smith D, et al. Simultaneous evaluation of lung anatomy and ventilation using 4D respiratory-motion-resolved ultrashort echo time sparse MRI. J Magn Reson Imaging 2019; 49(2):411-422.
5. Wu C, Krishnamoorthy G, Yu V, et al. 4D lung MRI with high-isotropic-resolution using half-spoke (UTE) and full-spoke 3D radial acquisition and temporal compressed sensing reconstruction. Phys Med Biol 2023; 68(3):035017.
6. Krishnamoorthy G, Smink J, Tourais J et al. Variable anisotropic FOV for 3D radial imaging with spiral phyllotaxis (VASP). Magn Reson Med 2021; 85(1):68-77.
7. Feng L, Axel L, Chandarana H, et al. XD-GRASP: golden-angle radial MRI with reconstruction of extra- motion-state dimensions using compressed sensing. Magn Reson Med 2016; 75(2):775-788.
8. Murray V, Siddiq S, Crane C, et al. Movienet: Deep space-time-coil reconstruction network without k-space data consistency for fast motion-resolved 4D MRI. Magn Reson Med 2023; DOI: 10.1002/mrm.29892; Online ahead of print.
Figures