0451
Longitudinal ADC changes in prostate cancer patients treated with hypofractionated radiotherapy with 1.5T MR-Linac1Research Department, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 2Comprehensive Oncology Center, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 3Department of Radiotherapy, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong, 4Medical Physics Department, Hong Kong Sanatorium and Hospital, Hong Kong, Hong Kong
Synopsis
Keywords: DWI/DTI/DKI, MR-Guided Interventions, MR-Linac
Motivation: Additional functional information from DWI is one of the major advantages of MR-Linac over conventional radiation therapy techniques, and is sparsely studied.
Goal(s): To monitor the ADC change during the course of hypofractionated radiation therapy in prostate cancer using a 1.5T MR-Linac.
Approach: For each patient, a prostate DWI-EPI scan was acquired immediately after each of the 5 hypofractionated radiation therapy sessions. The ADC maps were generated and compared among the fractions using the Kruskal-Wallis test.
Results: No significant ADC change among fractions might indicate that monitoring ADC alone might be insufficient to reflect the early treatment response.
Impact: Biological radiotherapy treatment planning has been proposed for decades, but was hindered by lack of tools that could provide functional information with spatial interpretation. The study results shed light on potential use of DWI for early treatment monitoring using MR-Linac.
Introduction
Diffusion-weighted imaging (DWI) has a well-established role in detecting suspicious lesions. For the purpose of radiotherapy, however, the perfect functional image should provide anatomical information such as lesion location and contour, and functional information for early treatment response assessment. Although the use of DWI in radiotherapy treatment monitoring has been studied, it was often done after the completion of the treatment. With the use of the hybrid MRI-Linac system (MR-Linac), it is now more conventient to monitor the early treatment response in a much shorter time-interval and higher frequency using DWI. In this pilot study, the early treatment response was accessed by measuring the inter-fractional ADC change of localized prostate cancer patients receiving hypofractionated SBRT using a 1.5 T MR-Linac.Methods
Ten patients (aged 71±7 years, with 10 lesions) who had localized prostate cancer were treated with hypo-fractionated SBRT (5-fraction treatment course, total dose = 36.25 - 40 Gy) using a 1.5T MR-Linac. Consent was obtained from each patient. After the completion of each fraction, patients underwent a DWI-EPI scan (TR/TE = 3025/77 ms, FOV = 240 x 240 cm2, slice thickness = 4mm, reconstruction voxel size = 3 x 3 x 4mm3, SENSE factor = 2.3, b-value = 15 (average = 6), 500 (12), 800(12) s/mm2) using a 1.5T MR-Linac in the treatment position and setup. Apparent diffusion coefficient (ADC) maps were generated using the scanner console. Before the first treatment fraction began, an additional high-resolution T2-weighted 3D TSE image was captured for each patient in the treatment position and setup.The contour of the whole prostate and intra-prostatic lesions were delineated on the T2-weighted image by a radiation oncologist with over 10 years of experience. Each of these contours was rigidly registered to the DWI and ADC images by an MR physicist with over 10 years of experience. A nonparametric Kruskal-Wallis test was conducted to compare the ADC and SNR values among the treatment fractions. The significance level was set at 0.05.Results
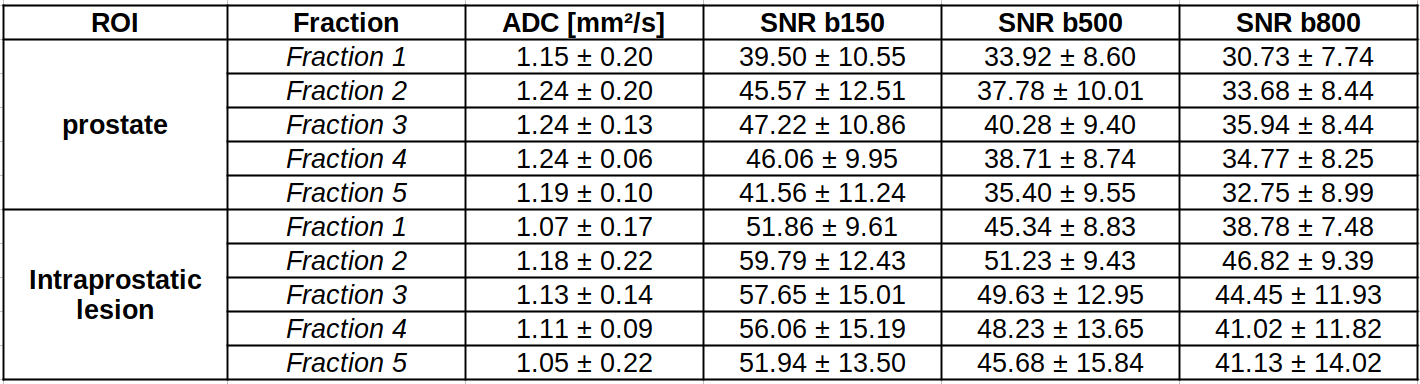
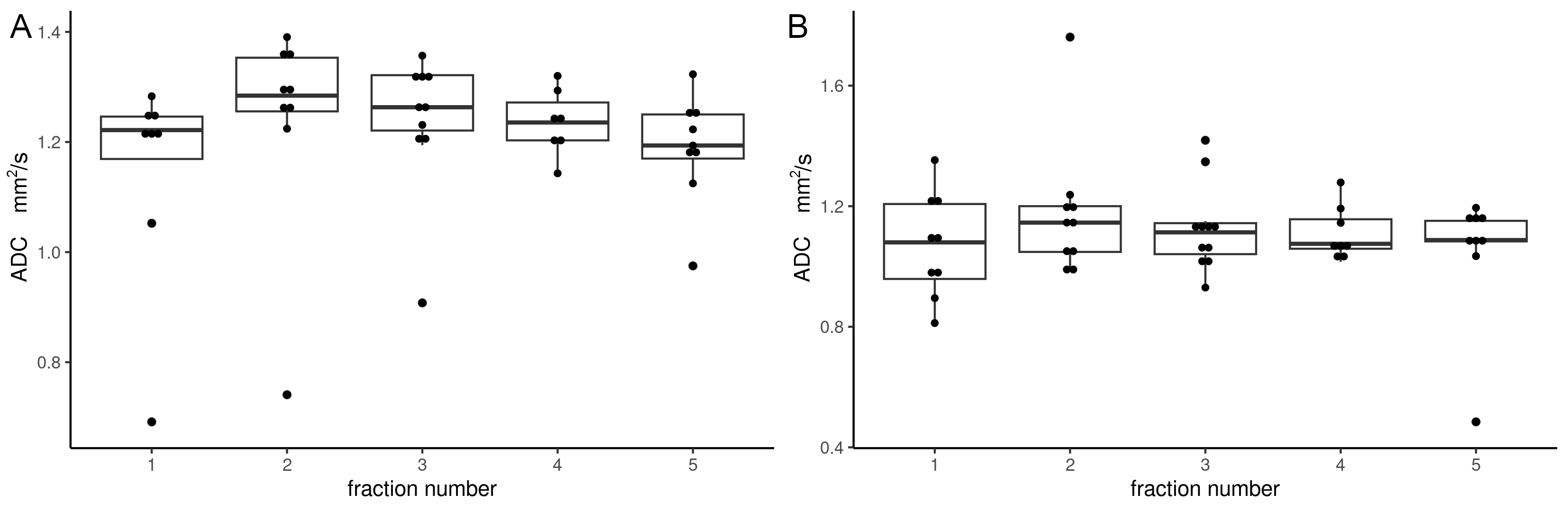
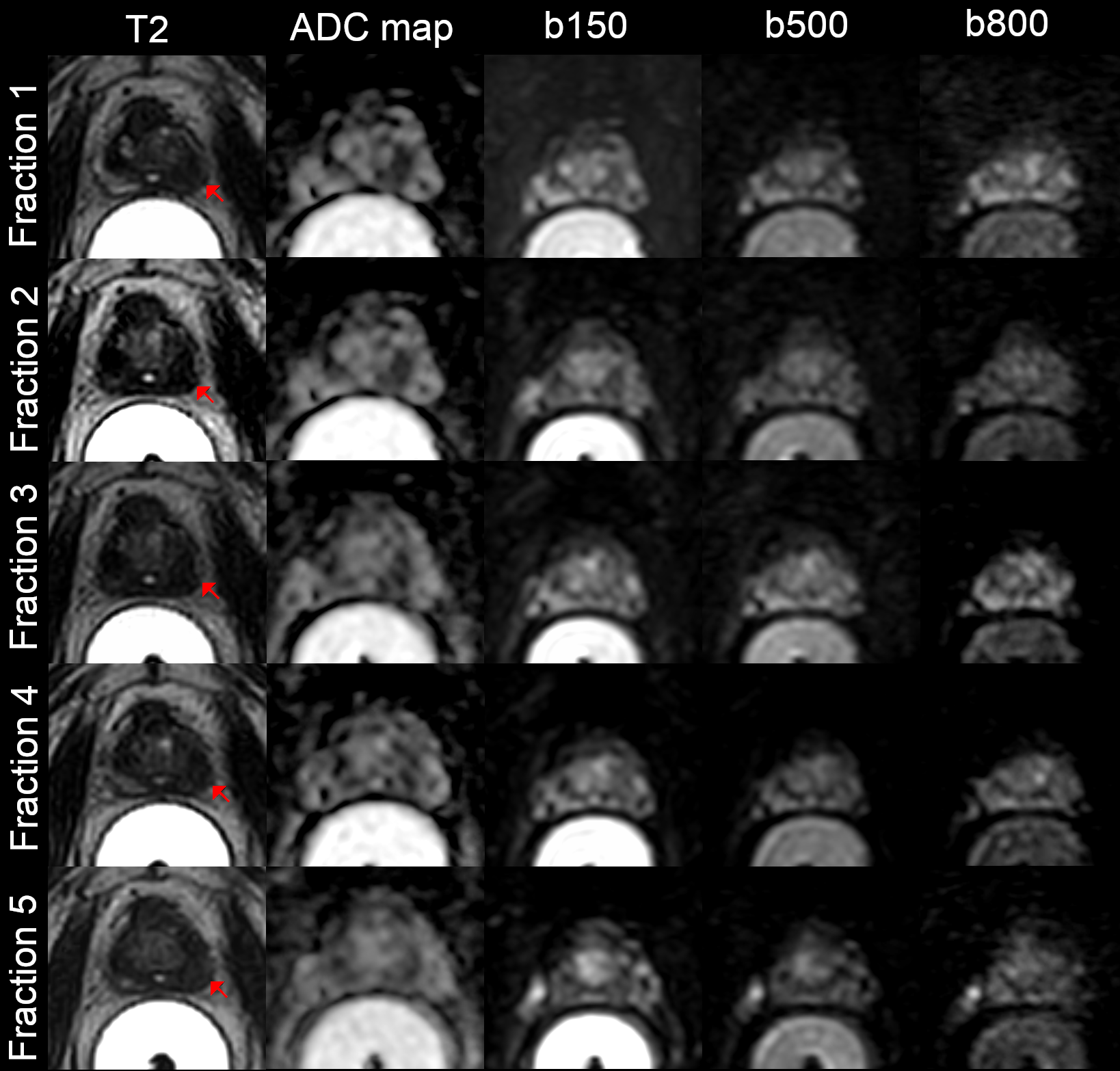
As depicted in the box plot (Figure 1), no significant intra-fractional ADC change was observed in the prostate (1.15±0.20 for fraction 1, 1.24±0.20 for fraction 2, 1.24±0.13 for fraction 3, 1.24±0.06 for fraction 4, and 1.19±0.10 for fraction 5, p>0.05). Similarly, no significant intra-fractional ADC change was noted in intra-prostatic lesions (1.07±0.17 for fraction 1, 1.18±0.22 for fraction 2, 1.13±0.14 for fraction 3, 1.11±0.09 for fraction 4, and 1.05±0.22 for fraction 5, p>0.05). It was important to highlight that the ADC values for the prostate increased from fraction 1 to fraction 2 and then slightly decreased. However, this ADC trend was not observed in the ROI of the intra-prostatic lesions.Generally, the lesion conspicuity on the ADC map gradually reduced with an increase in treatment fractions in some patients (Figure 2). This could potentially reduce the accuracy of the lesion ROI placement, thereby introducing additional bias in the ADC measurement. Although not measured in this study, a discrepancy in lesion size between T2-weighted and DWI images was observed in a few patients due to image artifacts in the DWI images. Hence, while DWI might help verify the lesion location, the delineation should be done on the T2-weighted 3D TSE images. Similar SNR among treatment fractions and b-values were also observed, with an overall mean SNR of 38.33±10.39 in the prostate and 47.02±15.10 in the intraprostatic lesions, all with p>0.05 (Table 1). To our knowledge, this is the first study that assesses intra-fractional ADC change in prostate patients undergoing hypofractionated SBRT via MR-Linac. The results of this study shows no significant inter-fraction ADC change, suggesting that ADC change alone may not be sensitive enough to detect early treatment response. The limitations of this study include a small sample size and neglect of organ deformation. Further research with larger sample sizes is required to confirm the value of MR-Linac DWI in radiotherapy.
Conclusion
While no significant change in ADC was observed during the course of treatment for the prostate and intra-prostatic lesions, further studies with a larger sample size are needed to confirm the usefulness of DWI for radiotherapy.Acknowledgements
No acknowledgement found.References
Figures