0449
Technical validation of DWI in the abdomen using different motion compensation techniques on a 1.5T MR-Linac1Radiation Oncology, the Netherlands Cancer Institute, Amsterdam, Netherlands, 2Christie Medical Physics and Engineering, The Christie NHS Foundation Trust, Manchester, United Kingdom, 3Section for Biomedical Physics, Department of Radiation Oncology, University Hospital Tübingen, Tübingen, Germany, 4Joint Department of Physics, The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London, United Kingdom, 5Radiotherapy, UMC Utrecht, Utrecht, Netherlands, 6MR Clinical Science, Philips Healthcare, Best, Netherlands, 7Radiation Physics, The University of Texas MD Anderson Cancer Center, Houston, TX, United States, 8Radiation Oncology, Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
Keywords: Diffusion Acquisition, Radiotherapy, ADC, MR-linac, abdomen, repeatability
Motivation: The apparent diffusion coefficient (ADC), derived from diffusion-weighted imaging (DWI), is a promising quantitative biomarker for treatment response during radiotherapy. However, DWI in the abdomen is complicated by respiratory motion.
Goal(s): To compare the repeatability of the ADC acquired with different motion compensation techniques on a 1.5T MR-linac.
Approach: A phantom and test-retest study (26 healthy volunteers) were performed, evaluating four DWI acquisitions (free breathing, navigator-triggered, and both repeated with an abdominal compression belt).
Results: From the 11 datasets analyzed so far, absolute ADC values and repeatability were comparable between the acquisitions in healthy regions of the liver, spleen and kidney.
Impact: This study initiates defining the optimal DWI acquisition strategy to measure treatment-related ADC changes of abdominal tumors on an MR-linac.
Purpose
With MRI-guided linear accelerators (MR-linac), monitoring treatment response with quantitative MRI during radiotherapy becomes practically feasible. As increasing ADC has been associated with positive treatment response in various tumors1, the apparent diffusion coefficient (ADC) derived from diffusion-weighted imaging (DWI) is a promising biomarker for this application. Sufficient repeatability of ADC measurements is crucial for treatment response monitoring. In the abdomen ADC repeatability might be affected by respiratory motion. Motion effects can be reduced by e.g. navigator triggering2 or using an abdominal compression belt3, but it is unknown whether these methods improve the repeatability. Therefore, this study aimed to perform technical validation of DWI in the abdomen using different motion compensation techniques on a 1.5T MR-linac system.Materials and Methods
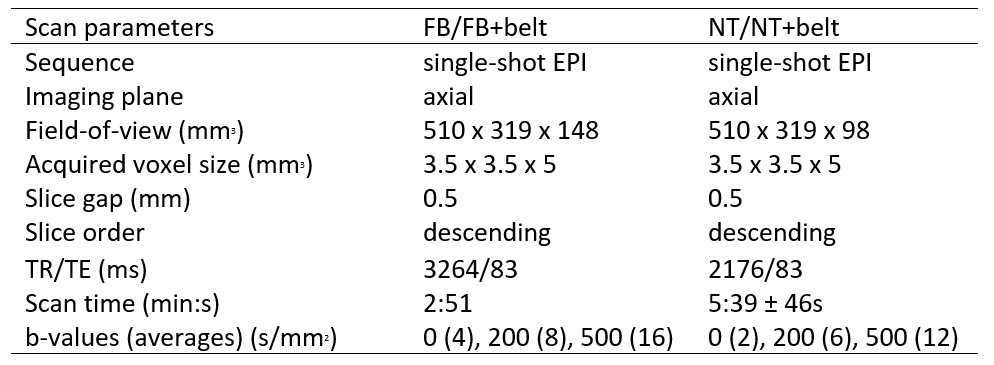
A free breathing (FB) and navigator-triggered (NT) acquisition with and without the use of an abdominal compression belt (Aspen Medical Products, Irvine, USA; FB+belt and NT+belt) were compared on a 1.5T MR-linac (Unity, Elekta AB). Most acquisition parameters were equal between FB and NT (Table 1). To keep the scan time for the NT acquisition around 5 min, different settings were used for TR, number of slices, and number of averages per b-value. ADC maps were derived from b = 200 and 500 s/mm2.To determine the accuracy of the FB and NT acquisitions with respect to a calibration sequence, the NIST/QIBA diffusion phantom was scanned in one center. The ADC bias and intra-session repeatability (RC) near isocenter were estimated according to QIBA guidelines4.
To assess the repeatability, a test-retest study was performed with 26 volunteers (12 female, 37±9 y/o). The study was approved by the institutional review board and all volunteers signed informed consent. DWI data of all four acquisitions were acquired on two separate days (max 2 weeks apart). For each acquisition, circular ROIs of 1 or 2 cm in diameter were delineated on the b = 0 s/mm2 image at three consecutive slices in homogeneous areas of the liver (2 ROIs), left kidney (1 ROI) and spleen (1 ROI). For each ROI, the median ADC was determined and compared between the four acquisitions of the first scan session using the Friedman test and Bonferroni corrected post-hoc testing. The repeatability coefficient (RC = 2.77✕wSD) and percentage RC (%RC = 2.77✕wCV) were determined from the two repeated measurements for each acquisition and ROI5.
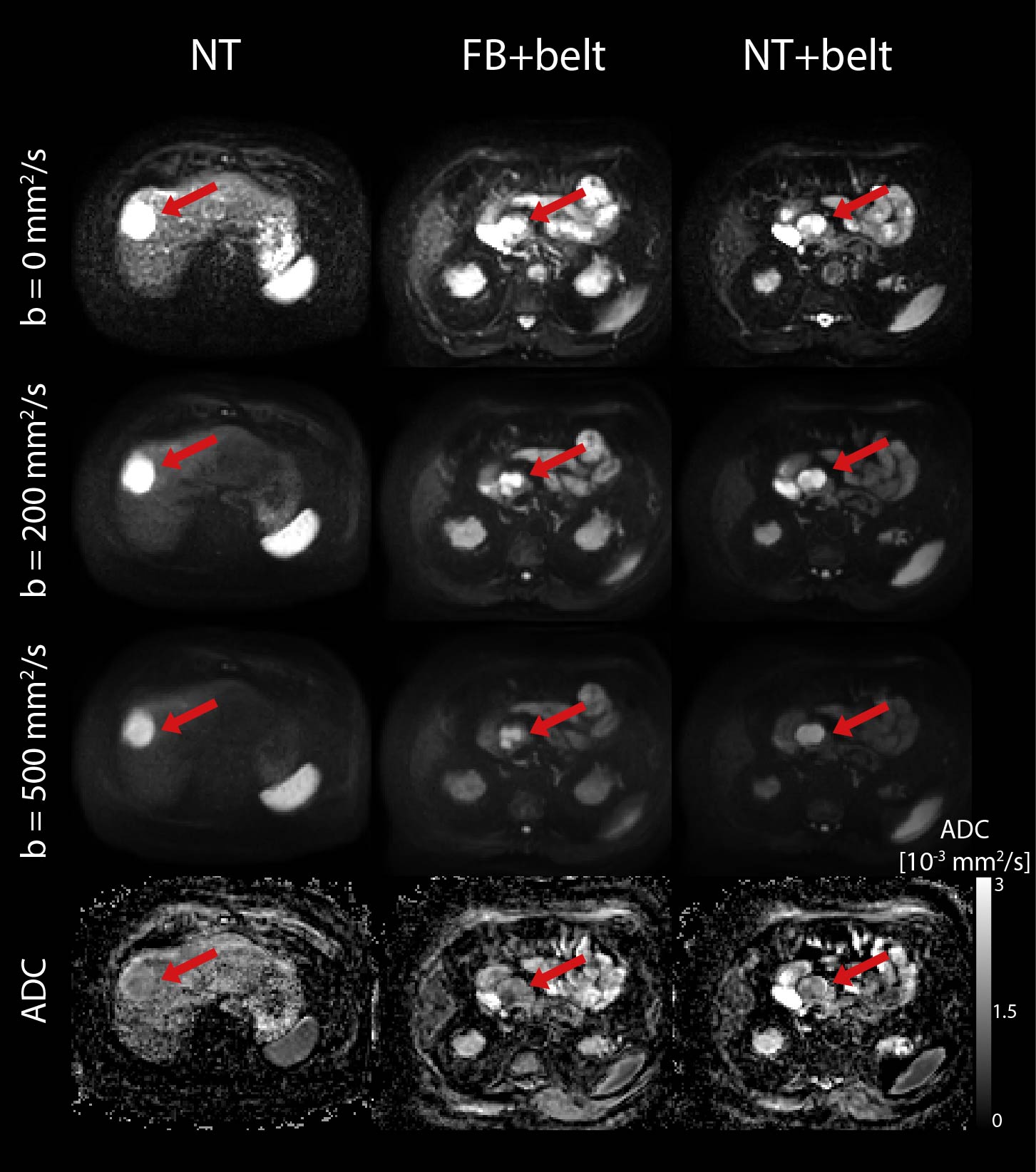
To assess feasibility, the sequences were tested in two patients in different institutes: NT in a patient with liver metastases (male, 66 y/o), FB+belt and NT+belt in a patient with pancreatic cancer (male, 69 y/o).
Results
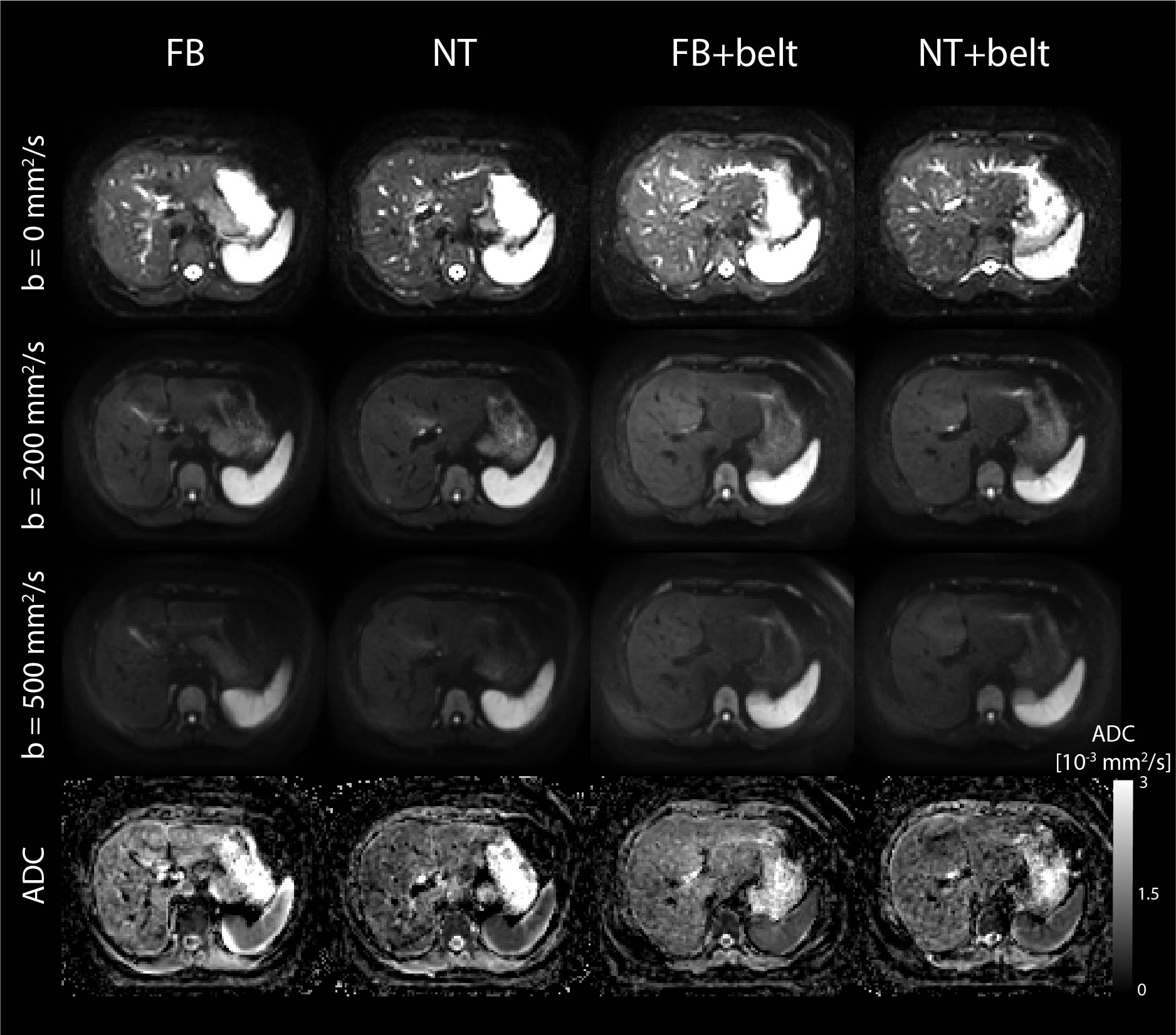
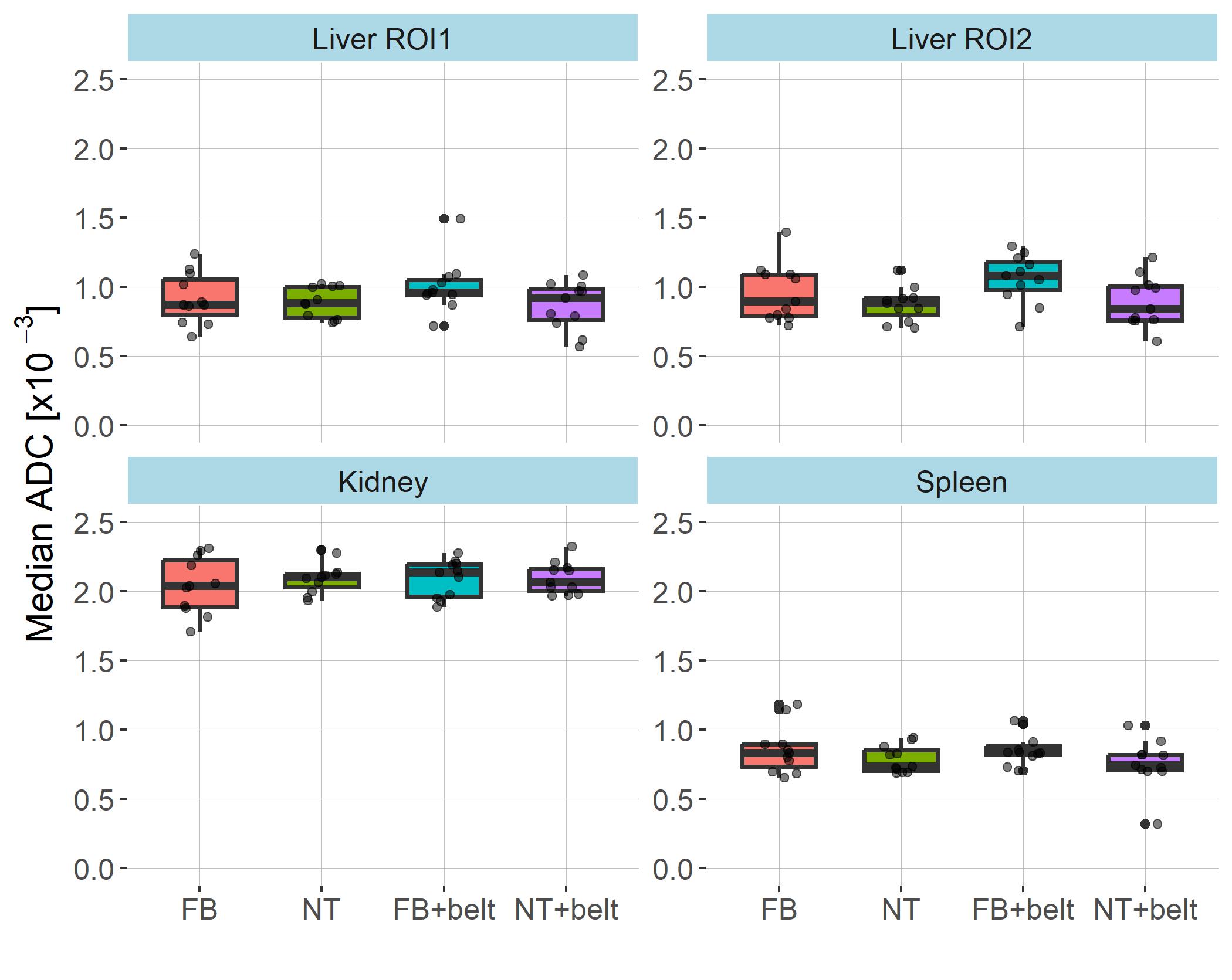
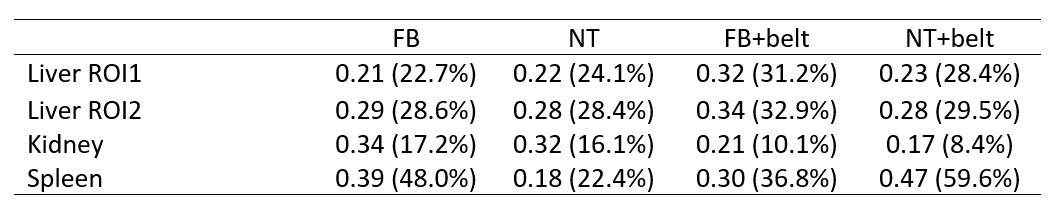
Compared to the reference value of the vial in the isocenter, the FB and NT acquisitions underestimated the ADC of -0.057✕10-3 and -0.060✕10-3 mm2/s respectively, which was smaller using the calibration sequence (-0.013✕10-3 mm2/s). The short-term repeatability was 0.023✕10-3 mm2/s for FB and 0.032✕10-3 mm2/s for NT, compared to 0.016✕10-3 mm2/s for the calibration sequence. A paired t-test showed that ADC values from the FB and NT acquisition were similar for all vials in the phantom (p=0.79).Generally, image quality improved using the NT acquisition and the compression belt (Fig. 1). So far, the data from 11 volunteers were analyzed. ADC values were similar across acquisitions (all adjusted p>0.16, Figure 2). RC values ranged from 0.17✕10-3 to 0.47✕10-3 mm2/s across ROIs and acquisitions (Table 2).
Applying the acquisitions in two patients demonstrated feasibility of motion compensation strategies in the clinical workflow (Figure 3).
Discussion
Phantom ADC was underestimated by the FB and NT acquisitions, exceeding the tolerance level of 0.04✕10-3 mm2/s of the QIBA DWI profile. Preliminary investigation suggest this underestimation was due to slice ordering. Nevertheless, median ADC values were similar between FB and NT acquisitions in both the phantom and in vivo data, suggesting that these acquisitions can be used interchangeably. None of the acquisitions showed superior repeatability compared to the other acquisitions although this remains to be confirmed using the complete dataset (n=26).Reproducible positioning of ROIs in homogeneous regions was challenging, especially in the liver, and might have affected the repeatability results6. Next steps are analyzing the complete dataset, applying offline motion compensation7, and including patient test-retest data. As tumor tissue typically exhibits higher signal, repeatability might be better in tumors. The results of this study are a first step in defining the best strategy for DWI acquisition for treatment-related changes in ADC of tumors in the abdomen on an MR-linac.
Acknowledgements
The authors thank Elekta AB and Philips Healthcare for their support to organize and participation during a hackathon weekend to develop the scan protocols for this study.References
[1] Van Houdt, P.J., et al. (2021). Quantitative Magnetic Resonance Imaging for Biological Image-Guided Adaptive Radiotherapy. Frontiers in Oncology.
[2] Taouli, B., et al. (2009). Diffusion‐weighted imaging of the liver: comparison of navigator triggered and breathhold acquisitions. Journal of Magnetic Resonance Imaging.
[3] Lovelock, D.M., et al. (2014). The Effectiveness of a Pneumatic Compression Belt in Reducing Respiratory Motion of Abdominal Tumors in Patients Undergoing Stereotactic Body Radiotherapy. Technology in Cancer Research & Treatment.
[4] https://qibawiki.rsna.org/images/6/63/QIBA_DWI
[5] Shukla-Dave A., et al. (2019). Quantitative imaging biomarkers alliance (QIBA) recommendations for improved precision of DWI and DCE-MRI derived biomarkers in multicenter oncology trials. Journal of Magnetic Resonance Imaging
[6] Bisgaard, A.L.H., et al. (2023). Recommendations for improved reproducibility of ADC derivation on behalf of the Elekta MRI-linac consortium image analysis working group. Radiotherapy and Oncology
[7] Pathak R., et al. (2019). Considering tumour volume for motion corrected DWI of colorectal liver metastases increases sensitivity of ADC to detect treatment-induced changes. Scientific Reports.
Figures