0446
Toward Hypoxia Imaging for Adaptive Dose Painting: Optimization of MP2RAGE for T1 Mapping in a Low-Field 0.35T MR-Linac (MRL)1Division of Physics and Biophysics, Department of Radiation Oncology, Brigham and Women's Hospital and Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, United States, 2Harvard–MIT Health Sciences and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Keywords: MR-Guided Radiotherapy, Radiotherapy
Motivation: Stereotactic MR-guided Adaptive Radiation Therapy (SMART) ‘dose painting’ for hypoxia can improve treatment outcomes, but implementation on MR-Linac (MRL) faces low-field SNR challenges. Optimization of T1-to-noise ratio at 0.35T will enable clinical implementation of oxygen-enhanced (OE)-MRI.
Goal(s): Develop and validate an optimized MP2RAGE sequence for low-field T1 mapping, establish feasibility and evaluate reproducibility in phantoms and healthy subjects.
Approach: We optimized and validated an MP2RAGE sequence with simulations and a ground-truth phantom. T1 mapping feasibility was established in healthy subjects, variability and reproducibility was assessed.
Results: A clinically feasible optimized low-field MP2RAGE protocol was developed, yielding accurate and reproducible T1 mapping.
Impact: This work builds a foundation towards clinically feasible hypoxia imaging for low-field MRL. This would facilitate a paradigm shift toward MR-guided biological adaptation and dose painting, leveraging the spatial distribution of hypoxia, and improving patient outcomes in conventionally challenging-to-treat cancers.
Introduction
Stereotactic MR-guided Adaptive Radiation Therapy (SMART) is improving patient outcomes through a shift towards high soft-tissue contrast MRI with online adaptive treatments, particularly in conventionally challenging-to-treat cancers.1 While advances in clinical efficacy have been made, online adaptions have been predominantly anatomic in nature, suggesting additional improvements with novel biological information. Hypoxic tissues demonstrate up to a threefold increased resistance to radiation damage, representing a significant challenge in radiation oncology.2 Adaptive dose escalation or ‘dose painting’ to hypoxic regions within tumours holds promise, but clinically feasible imaging and localization remains a challenge. Oxygen enhanced (OE)-MRI is an attractive solution, that detects hypoxia via preferential O2 uptake and T1 relaxation shortening in normoxic tissues. Magnetization Prepared Rapid (2) Gradient Echo (MP2RAGE) sequence can be used to generate quantitative T1 maps,3 and quantify the tissue oxygenation level dependent (TOLD) T1 contrast effect. Implementation of MP2RAGE for TOLD on MR-Linac (MRL) requires optimization specific to low-field T1 mapping. This study aims to develop and validate an optimized MP2RAGE sequence for low-field T1 mapping, and establish feasibility in a clinical 0.35T MRL and evaluate reproducibility in phantoms and human studies.Methods and Materials
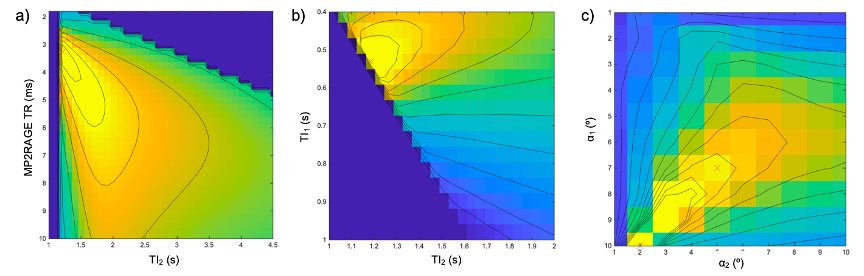
All scans were acquired with a multi-channel head coil on a low-field 0.35T MRL (MRIdian, ViewRay Inc., Mountain View, CA).Optimization of MP2RAGE for Low-Field: With Bloch equation simulations, we maximized contrast-to-noise ratio (CNR) per unit time in brain tissues, specifically white matter (WM) and grey matter (GM). MP2RAGE sequence parameters were systematically varied for all feasible combinations, encompassing MP2RAGE TR 2000–12000 (250 ms steps), TI1/TI2 from nTR/2 to MP2RAGE TR–nTR/2 (100 ms steps), and α1 and α2 from 1–90º. The GRE module number of excitations (n) was 160, TR was 4 ms, and adiabatic pulse inversion efficiency was 1.0.
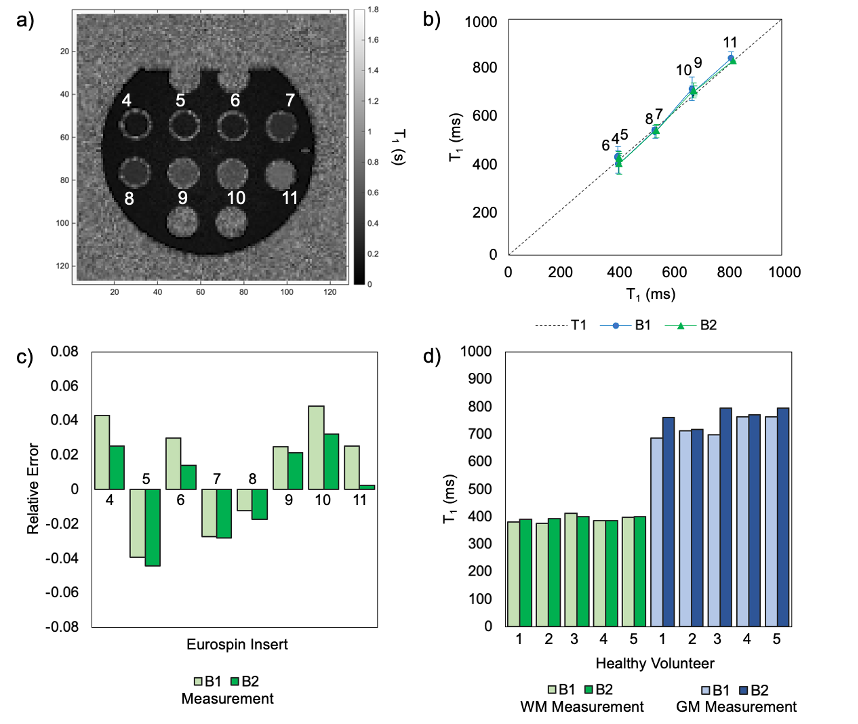
Ground-Truth T1 Mapping: The optimized MP2RAGE protocol and T1 mapping was validated with a ground-truth Eurospin phantom (ELSE Solutions, Naviglio, MI, Italy) containing eight inserts of known T1 values ranging from approximately 400–800 ms. Evaluation metrics included the mean (SD) T1 relative error (RE) and T1-to-noise ratio (TNR) in each insert compared with ground-truth T1 values. T1 mapping reproducibility was evaluated with the coefficient of variability (CV) for each T1 insert.
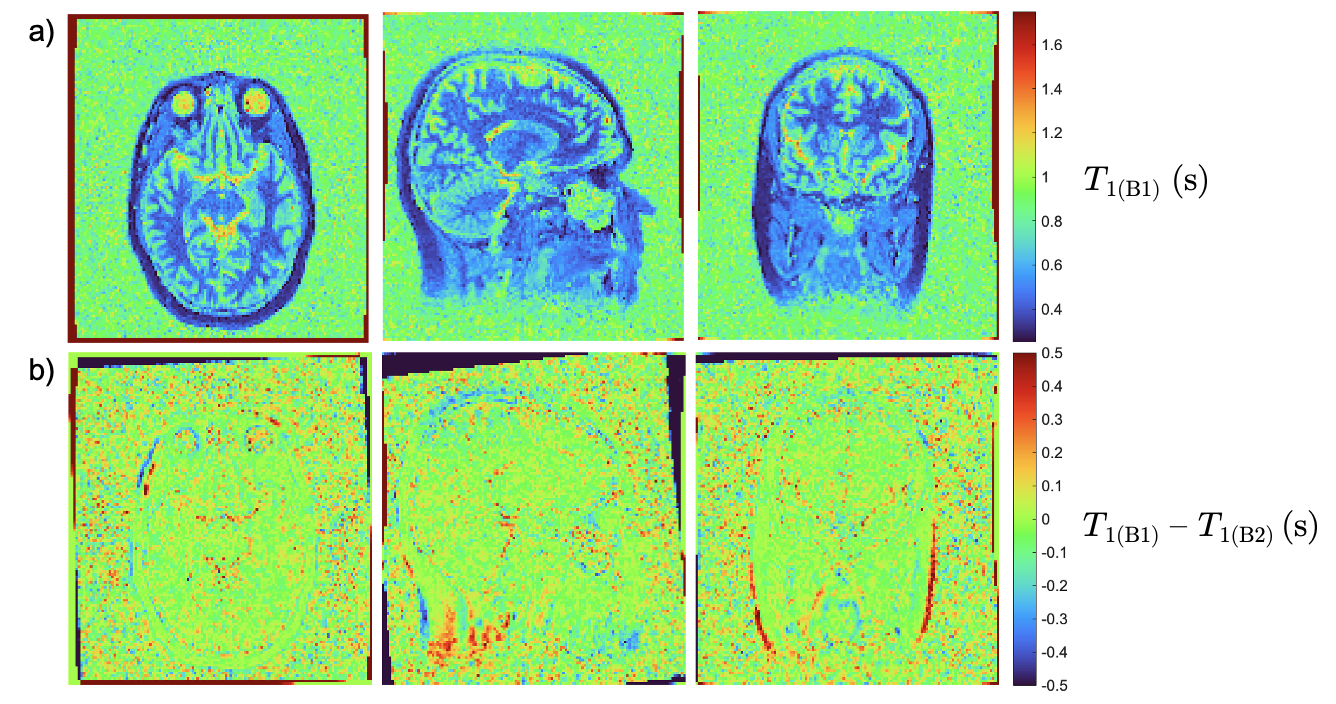
Healthy Volunteer Studies: Feasibility of the optimized low-field MP2RAGE protocol was established in a cohort of five healthy subjects following informed consent. Whole-head acquisitions with 2.0 mm3 isotropic voxels and two averages were acquired with an approximate 13-minute acquisition time, across two sessions at least 48-hours apart. T1 maps were generated and the mean (SD) T1 values for WM and GM from a region of interest (ROI) were calculated. To evaluate reproducibility, the CV was calculated, and a voxel-to-voxel T1 difference map was generated to assess the spatial variation between the scan sessions.
Results and Discussion
Optimization of MP2RAGE for low-field (0.35T) in brain tissues resulted in sequence parameters: MP2RAGE TR = 3250 ms, TI1/TI2 = 500/1200 ms, and α1/α2 = 7/5º. Fig. 1 illustrates low-field MP2RAGE simulation cross-sections of the CNR per unit of time as a function of (a) MP2RAGE TR versus TI2, (b) TI1 versus TI2, and (c) α1 versus α2. Generated T1 maps of the Eurospin [Fig. 2(a)] exhibited in a mean (SD) RE of 0.01 ± 0.03 from ground-truth T1 values and TNR of 23.39 ± 6.67. Strong linear correlations (R2 > 0.99) were observed between measured and ground-truth T1 values [Fig. 2(b)]. The CV between two acquisition sessions was 0.90 ± 2.24, indicating reproducibility.In healthy subjects, images showed high anatomical quality and brain tissue (WM and GM) differentiation without discernible image artifacts. T1 maps were generated [Fig. 3(a)] and the mean (SD) T1 values were 392 ± 11 ms for WM and 746 ± 44 ms for GM, consistent with reported literature values of approximately 427 ms and 652 ms, respectively.4 The CV between two sessions was 0.02 ± 0.01, and a voxel-to-voxel T1 difference map was generated, demonstrating a normal spatial distribution of noise [Fig. 3(b)].
Conclusion
We successfully optimized MP2RAGE parameters for low-field and demonstrated its ability to generate accurate, reproducible, and clinically feasible T1 maps in phantom and healthy subjects. This work builds the foundation toward clinically feasible hypoxia imaging for low-field MRL with an OE-MRI mechanism, with current work focused on refining the protocol for TOLD T1 contrast in the brain. This advancement would facilitate a paradigm shift toward MR-guided biological adaptation and dose painting, leveraging the spatial distribution of hypoxia, and improving patient outcomes in conventionally challenging-to-treat cancers.Acknowledgements
The authors acknowledge funding support from the Natural Sciences and Engineering Research Council of Canada (NSERC) Postdoctoral Fellowship (PDF) program.References
- Otazo R, Lambin P, Pignol JP, Ladd ME, Schlemmer HP, Baumann M, Hricak H. MRI-guided Radiation Therapy: An Emerging Paradigm in Adaptive Radiation Oncology. Radiology. 2021 Feb; 298(2) 248-260.
- Sørensen BS, Horsman MR. Tumor Hypoxia: Impact on Radiation Therapy and Molecular Pathways. Front Oncol. 2020 Apr 21; 10(1) 562.
- Marques JP, Kober T, Krueger G, van der Zwaag W, Van de Moortele PF, Gruetter R. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. Neuroimage. 2010 Jan 15; 49(2) 1271-81.
- Zhu J, Klarhöfer M, Santini, F, Scheffler K, Bieri O. Relaxation Measurements in Brain Tissue at Field Strengths Between 0.35T and 9.4T. Proc. Intl. Soc. Mag. Reson. Med. 2014, 22: 3208. Milan, Italy.
Figures