0437
Distinct functional connectivity of anterior cingulate cortex subregional networks in first-episode and recurrent major depressive disorder1Department of Radiology and Huaxi MR Research Center (HMRRC), Functional and Molecular lmaging Key Laboratory of Sichuan Province, West China Hospital, Sichuan University, Chengdu, China, 2Research Unit of Psychoradiology, Chinese Academy of Medical Sciences, Chengdu, China, 3Department of Radiology, West China Xiamen Hospital of Sichuan University, Xiamen, China
Synopsis
Keywords: Psychiatric Disorders, fMRI (resting state), major depresive disorder
Motivation: The fine-grained anterior cingulate cortex (ACC) subregional functional connectivity alterations in first-episode and recurrent major depressive disorder (MDD) remained unclear.
Goal(s): To obtain optimal functional ACC subdivisions and explore alterations in intrinsic functional connectivity of ACC subregional networks in first-episode and recurrent MDD.
Approach: We utilized a data-driven connectivity-based parcellation to obtain optimal ACC subdivisions, calculated ACC subregional functional connectivity, and compared among first-episode, recurrent MDD patients and healthy controls.
Results: Ventral and dorsal ACC per hemisphere were identified as optimal parcellation. The ACC subregional connectivity was reduced in all MDD patients, while dorsal ACC connectivity was significantly reduced only in recurrent patients.
Impact: Our discovery of impaired functional architectures of ACC subdivisions in MDD, with a more prominent disrupted connectivity of dorsal ACC in relapsed patients, emphasize a potential role of ACC subregional connectivity in distinguishing MDD at different episodes and predicting relapse.
Introduction
The anterior cingulate cortex (ACC), a large brain region responsible for emotional processing, cognitive regulation and homeostatic maintenance, shows substantial functional heterogeneity along its ventral-dorsal axis1, 2. Growing neuroimaging evidences support a crucial involvement of the dysconnectivity of ACC and its subregions in pathophysiology of major depressive disorder (MDD)3, 4. Most researches exploring functional connectivity of ACC subregional networks used a priori coordinate or atlas of ACC subregions from previous studies, which may not fully adapt to the current data and lead to bias. The well-developed data-driven connectivity-based parcellation (CBP) method allows segmentation of the ACC based on functional connectivity properties to provide a better representation of the ACC functional subregions5. Our research utilized the ACC subdivisions obtained from CBP method to precisely delineate the fine-grained ACC subregional functional connectivity alterations in first-episode MDD (FED) and recurrent MDD (RED).Methods
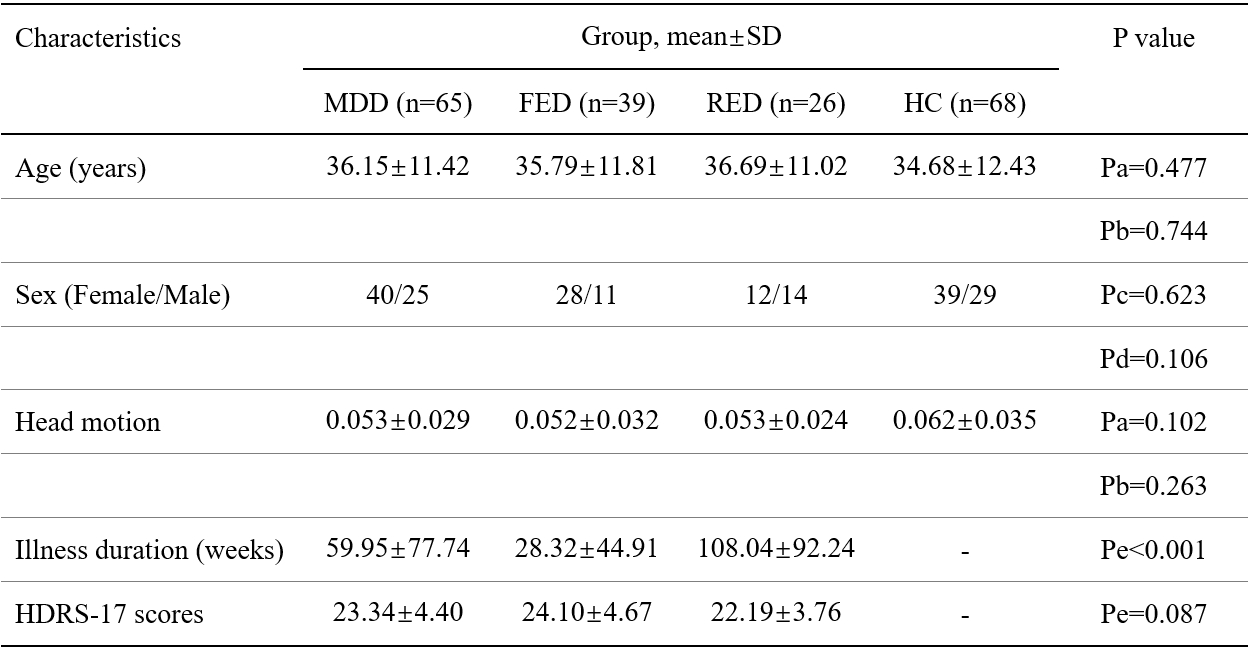
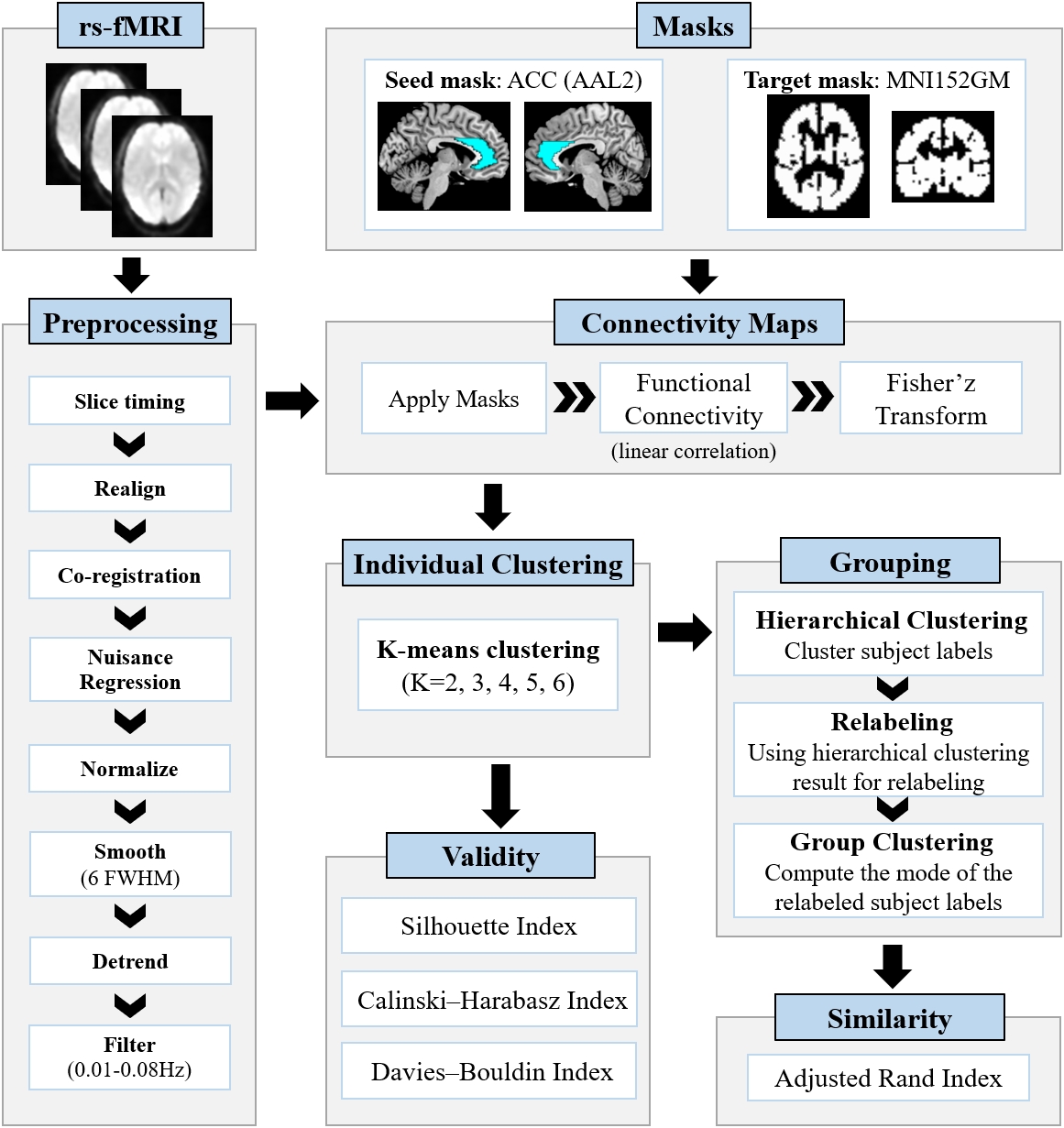
We recruited 65 medication-free MDD patients (39 FED and 26 RED) and 68 age- and sex- matched healthy controls (HC). All participants were scanned at rest using the GE Signa EXCITE 3‐T MR system (GE Healthcare, Milwaukee) with an 8‐channel phased‐array head coil. Preprocessing of neuroimaging data includes slice-timing, realignment, nuisance regression, spatial normalization (2mm), smoothing (6mm FWHM), detrending, and filtering (0.01-0.08Hz). The Friston 24-parameter model was used to regress out head motion confounding effects. Connectivity-based parcellation was conducted using CBPtools6 based on Python3.7 to segment the entire ACC per hemisphere from automated anatomical labeling atlas (AAL2) into distinct subdivisions based on their resting-state functional connectivity (rsFC) patterns with the rest of whole brain (Figure 1). Briefly, the rsFC between each voxel of ACC and every voxel of the rest brain was computed for each subject. Then, the k-means clustering was performed on the connectivity matrices to assign the voxels of ACC into clusters with similar connectivity characteristics to obtain the individual ACC parcellations. Next, the group-level clustering was calculated, containing relabeling individual clustering and computing mode of relabeled subject-wise clustering. The optimal number of clusters was determined by clustering quality indicators, including Silhouette index, Calinski-Harabasz index and Davies-Bouldin index.The rsFC map of each ACC subregion obtained was generated for all participants. Analysis of variance (ANCOVA) was used to evaluate group differences between MDD and HC groups, and to further investigate group differences among FED, RED and HC groups, both with age, sex and head motion as covariates. The significant threshold was set to Puncorrected <0.005 at voxel-level and PFWE <0.0125 (0.05/4) at cluster-level. Post-hoc analysis after ANCOVA among three groups was performed using Bonferroni test in SPSS24.0, with a significant threshold of P< 0.05. Moreover, relationships between the observed rsFC alterations with number of episodes, illness duration, and symptom severity in MDD group were explored via partial correlation, controlling for age, sex and head motion.
Results
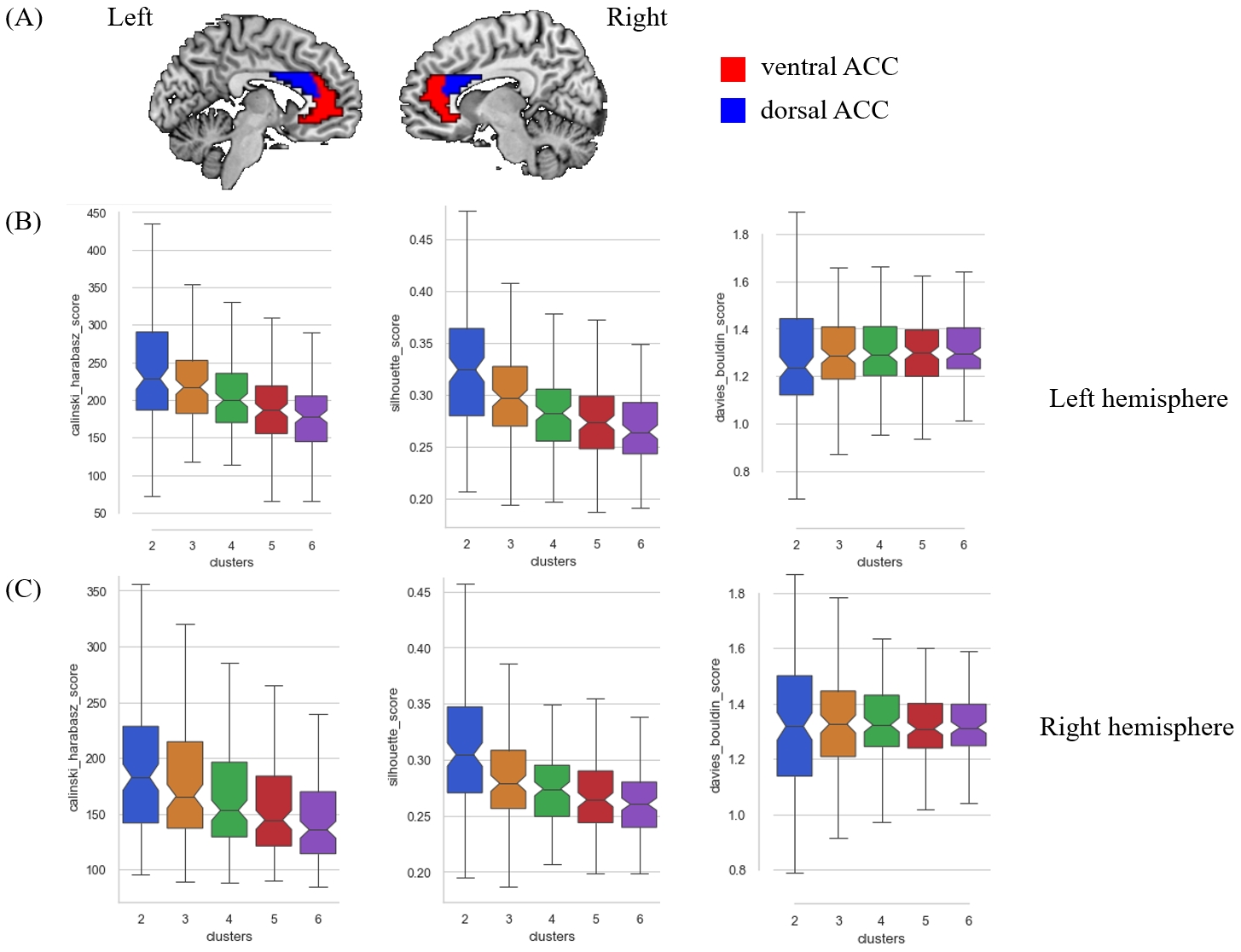
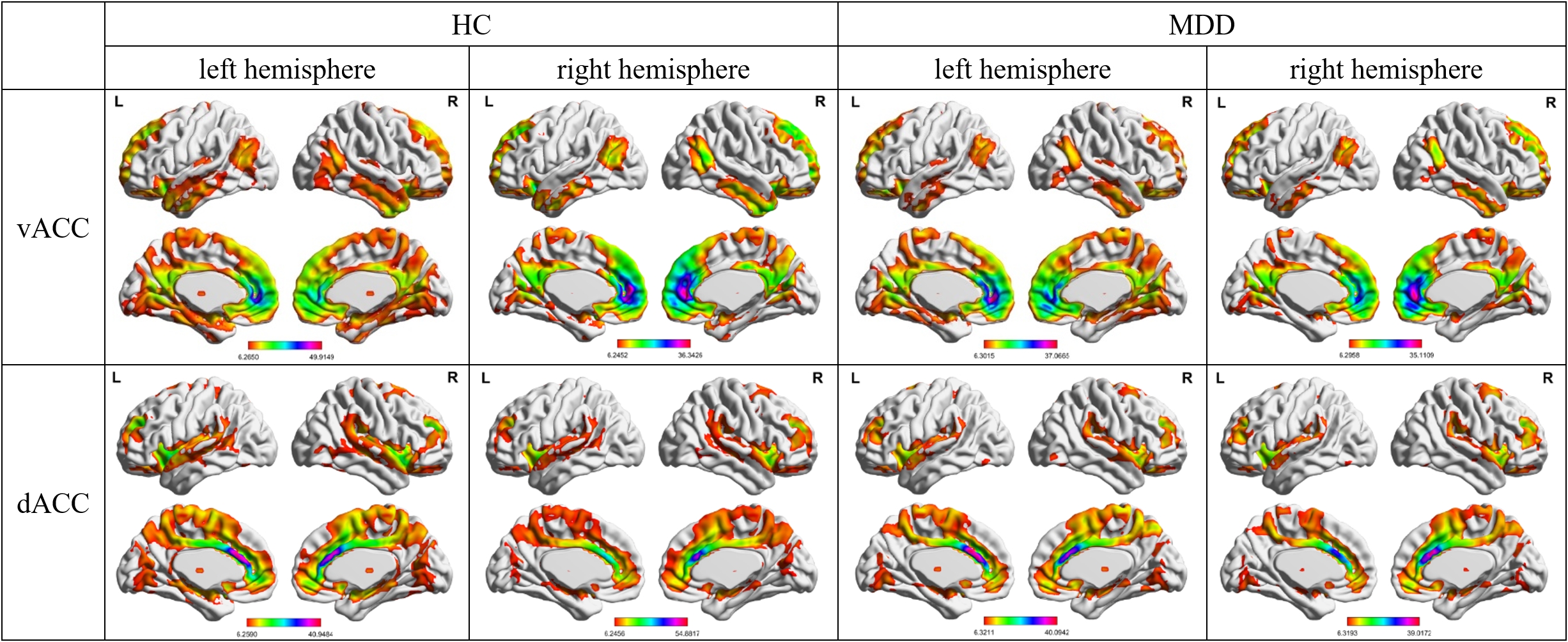
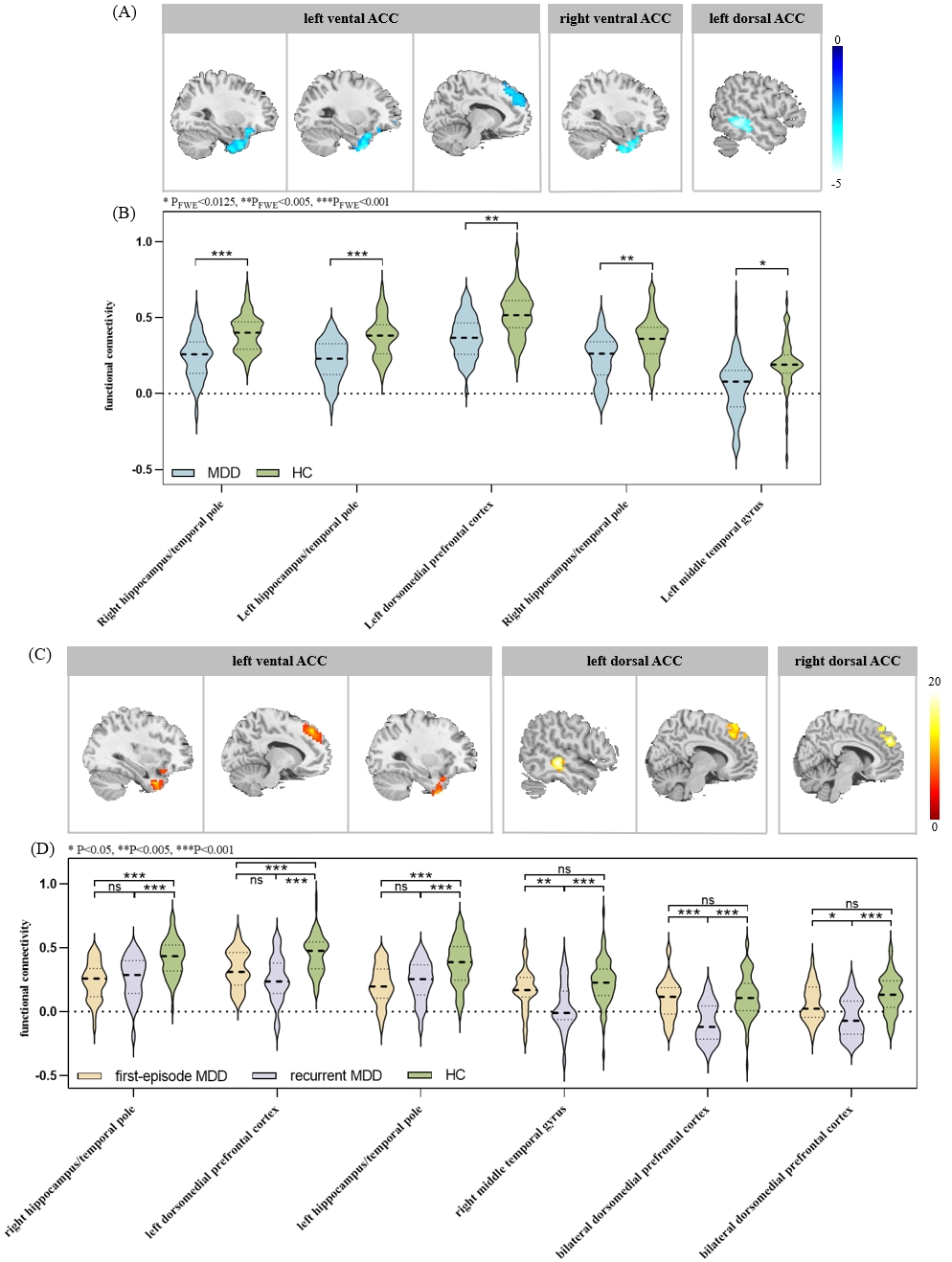
The socio-demographic and clinical characteristics of the participants were provided in Table 1.Two subdivisions of ACC per hemisphere, ventral ACC (vACC) and dorsal ACC (dACC), were identified as the optimal parcellation according to cluster quality indicators (Figure 2), and the rsFC map of each ACC subregion in MDD and HC group were available in Figure 3.
Relative to HC, MDD patients demonstrated significant hypoconnectivity between left vACC with left/right hippocampus/temporal pole (TP) and left dorsomedial prefrontal cortex (dmPFC), between right vACC and right hippocampus/TP, and between left dACC and left middle temporal gyrus (MTG). After categorizing patients into FED and RED subgroups, through ANCOVA and post-hoc analysis, we found significant disrupted rsFC of left vACC with left/right hippocampus/TP and left dmPFC in both FED and RED patients compared with HC. Additionally, the significant impaired connectivity between bilateral dACC and bilateral dmPFC, and between left dACC and right MTG were only observed in RED, relative to FED and HC groups. There was no significant correlation between the observed rsFC alterations and clinical features after correcting for multiple comparisons.
Discussion & Conclusion
Through data-driven connectivity-based parcellation, we identified that the ACC is best represented with a bipartite ventral-dorsal subdivision. We further discovered disrupted intrinsic connectivity of ACC subregions in MDD relative to HC, of which the hypoconnectivity of vACC with hippocampus and dmPFC were significant in MDD patients, while the hypoconnectivity of dACC with dmPFC and MTG were only significant in relapsed patients. These findings implicated the intrinsic connectivity of ACC subregions along ventral-dorsal axis was impaired in MDD patients, with disorganized functional architecture of dACC being more prominent in patients with relapses, which emphasize the importance of ACC subregional connectivity in distinguishing MDD with various number of episodes and provide potential translational neuroimage markers for relapse prediction.Acknowledgements
This study was supported by the Natural Science Foundation of Sichuan Province (Grant No. 2022NSFSC0052) and the National Key R&D Program of China (Grant No. 2022YFF1202400).References
1. Dixon ML, Thiruchselvam R, Todd R, et al. Emotion and the prefrontal cortex: An integrative review. Psychol Bull. 2017;143(10):1033-81.
2. Gasquoine PG. Localization of function in anterior cingulate cortex: from psychosurgery to functional neuroimaging. Neurosci Biobehav Rev. 2013;37(3):340-8.
3. Mulders PC, van Eijndhoven PF, Schene AH, et al. Resting-state functional connectivity in major depressive disorder: A review. Neurosci Biobehav Rev. 2015;56:330-44.
4. Pizzagalli DA, Roberts AC. Prefrontal cortex and depression. Neuropsychopharmacology. 2022;47(1):225-46.
5. Eickhoff SB, Yeo BTT, Genon S. Imaging-based parcellations of the human brain. Nat Rev Neurosci. 2018;19(11):672-86.
6. Reuter N, Genon S, Kharabian Masouleh S, et al. CBPtools: a Python package for regional connectivity-based parcellation. Brain Struct Funct. 2020;225(4):1261-75.
Figures