0425
Spiral T1w-Dixon-VIBE for high resolution abdominal imaging at 0.55T1Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Siemens Medical Solutions USA, Los Angeles, CA, United States
Synopsis
Keywords: Liver, Low-Field MRI, Spiral, Dixon, abdomen
Motivation: Breath-held abdominal fat-suppressed imaging is challenging at mid- and low-field strengths (<1.5T). Fat saturation often fails due to the short T1 of lipid; and Cartesian Dixon imaging provides poor spatial resolution due to the need for long ∆TE, due to the smaller ∆f between water and lipid.
Goal(s): Breath-held fat-suppressed high-resolution volumetric abdominal imaging with T1 contrast.
Approach: Stack-of-Spirals Dixon imaging, with estimation and compensation for phase due to concomitant fields
Results: We demonstrate that spiral Dixon imaging at 0.55T makes excellent use of the required ∆TE, improving SNR efficiency and spatial resolution (1.7x1.7x5.0mm3) compared Cartesian Dixon (3.5x3.5x5.0mm3), within a 17-second breath-hold.
Impact: We demonstrate that spiral Dixon single breath-hold volumetric imaging is an attractive alternative to existing Cartesian-based methods for volumetric single breath-hold fat-suppressed imaging at 0.55T, as it simultaneously provides high-resolution and excellent fat-suppression.
Introduction
The role of fat-suppressed T1-weighted 3D-GRE abdominal imaging is well established, with applications from liver tumor detection, surgical planning, to evaluation of pancreatic disease [1-3]. Chemically-selective fat-suppression techniques provide desired contrast at conventional field-strengths (1.5T, 3T). For cases where excellent fat-suppression is required, T1w-Dixon-VIBE used [4], at the cost of increased scan time.At lower field strengths (<1.5T), existing fat-suppression techniques often fail due to shorter fat T1 and smaller chemical-shift between fat and water. In this case, Cartesian Dixon-VIBE still provides excellent fat-suppression, but the increased optimal echo separation requires compromising the spatial resolution to fit the acquisition within a single breath-hold.
In this work, we propose using Stack-of-Spiral Dixon-VIBE to leverage increased inter-echo duration with efficient sampling [5]. This allows us to achieve 4-fold finer in-plane resolution compared to Cartesian, while keeping the same breath-hold duration with fat suppression.
Methods
Experiments were performed using a whole-body 0.55T system (prototype MAGNETOM Aera, Siemens Healthineers, Erlangen, Germany) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). Data collection used a 6-channel body array (anterior) and 6 elements from a table-integrated 18-channel spine array (posterior).After providing written informed consent, one healthy female volunteer and two volunteers with elevated liver fat (Male BMI=33, Female BMI=26.3), were scanned in supine position arms-down, under a protocol approved by our Institutional Review Board.
All scans were RF-spoiled multi-echo gradient-recalled echo and covered a single 26-28cm axial slab of the abdomen from the top of the liver to the iliac crest. Cartesian-VIBE and prototype stack-of-spirals-VIBE sequences were designed to utilize the same 16-18sec breath-hold duration. Table 1 summarizes the scan parameters. To optimize contrast and SNR, 11 flip-angles from 4° to 90° were tested in one volunteer using the spiral sequence. Muscle, kidney and liver regions were manually segmented and mean-signal and contrast were plotted.
Echo images are reconstructed using parallel-imaging compressed-sensing with locally low-rank constraint in BART [6] for spiral acquisitions. Coil sensitivities were estimated from low-resolution non-linear inversion (NLINV) [7]. Concomitant field compensation for axial spiral acquisitions was applied [8]. Gradient non-linearity is corrected by image-based interpolation using calculated displacement maps. Water/Fat separation was performed using region-growing IDEAL [9-10]. Aliasing from arms are reduced using ROVir [11].
Results
Figure 1b shows the mean-signal and contrast curves for each segmented tissue (solid lines). The measured curves are validated against SPGR simulation with previously reported T1 and T2 values [12] (dashed lines). According to these, FA of 16-18° provides the best SNR efficiency, and 22-24° provides the best CNR efficiency.Figure 2 shows a comparison between Cartesian Fat-Sat-VIBE (FS-VIBE), Cartesian Dixon-VIBE, and spiral-Dixon-VIBE water-only images, using 3 axis reformat. FS-VIBE imaging provides adequate spatial resolution with incomplete fat suppression. Cartesian Dixon-VIBE provides excellent fat suppression and comparable contrast, but has poor spatial resolution. Spiral-Dixon-VIBE imaging simultaneously provides appropriate contrast, excellent fat-suppression, and superb spatial resolution.
Figures 3 and 4 compare representative water-only images of Cartesian-Dixon-VIBE and spiral-Dixon-VIBE imaging for volunteers with elevated liver fat with 21.8±2.8% and 11.6±2.7% PDFF, respectively. Both figures demonstrate the proposed techniques’ ability to image different body habitus.
Discussion
Fat saturation pre-pulses are impractical at 0.55T, due to the shorter T1 (~150ms) and smaller fat/water chemical-shift (-80Hz), as shown in Figure 2. As an alternative, we demonstrate high resolution, single breath-hold water-only abdominal imaging at low-field utilizing spiral-Dixon-VIBE with concomitant field compensation.There are Fat-Sat pulses tailored for lower fields [13], however, fundamental limitations mentioned above is still challenging. One issue is available imaging window being extremely short after each Fat-Sat pulse due to rapid T1-recovery. This causes reduction in scan efficiency, limiting the resolution that can be achieved.
Dixon imaging also provides fat-only images, which has added value for quantifying visceral fat and other adipose tissue. This could be valuable for risk assessment in some patient groups such as those with fatty liver (Figure 3, 4).
This study emphasized the demonstration of adequate contrast, fat suppression, and ability to achieve 4-fold finer spatial resolution. We applied this to a “catch-all” abdominal protocol in terms of the coverage and resolution. This can be easily adapted to “focused” protocols that covers only liver/pancreas or kidneys/adrenals, and we would expect a similar 4-fold increase in spatial resolution over Cartesian-Dixon-VIBE. The proposed method requires broader testing and validation in a larger cohort including diverse clinical cases.
Conclusion
High resolution single breath-hold volumetric fat suppressed T1 weighted abdominal imaging is feasible at 0.55T using spiral trajectories. This approach provides superior spatial resolution compared to Cartesian Dixon-VIBE and superior fat suppression compared to Cartesian fat-suppressed VIBE.Acknowledgements
We acknowledge grant support from the National Science Foundation (#1828736) and research support from Siemens Healthineers. We thank Liyun Yuan, Darryl Hwang and Vikas Gulani for helpful discussions.References
Rofsky NM, Lee VS, Laub G, et al. Abdominal MR Imaging with a Volumetric Interpolated Breath-hold Examination. Radiology. 1999;212(3):876-884. doi:10.1148/radiology.212.3.r99se34876
Conversano F, Franchini R, Demitri C, et al. Hepatic Vessel Segmentation for 3D Planning of Liver Surgery: Experimental Evaluation of a New Fully Automatic Algorithm. Academic Radiology. 2011;18(4):461-470. doi:10.1016/j.acra.2010.11.015
Koç U, Ocakoğlu G, Algın O. The efficacy of the 3-dimensional vibe-caipirinha-dixon technique in the evaluation of pancreatic steatosis. Turk J Med Sci. 2020;50(1):184-194. doi:10.3906/sag-1909-83
Ding Y, Rao SX, Chen CZ, Li RC, Zeng MS. Usefulness of two-point Dixon fat-water separation technique in gadoxetic acid-enhanced liver magnetic resonance imaging. World J Gastroenterol. 2015;21(16):5017-5022. doi:10.3748/wjg.v21.i16.5017
Mugler JP, Fielden SW, Meyer CH, et al. Breath-hold UTE Lung Imaging using a Stack-of-Spirals Acquisition. Proc. ISMRM. 2015. Abstract 1476.
Blumenthal M, Holme C, Roeloffs V, et al. BART Toolbox for Computational Magnetic Resonance Imaging. Published online September 24, 2022. doi:10.5281/ZENODO.592960
Uecker M, Hohage T, Block KT, Frahm J. Image reconstruction by regularized nonlinear inversion—Joint estimation of coil sensitivities and image content. Magnetic Resonance in Medicine. 2008;60(3):674-682. doi:10.1002/mrm.21691
King KF, Ganin A, Zhou XJ, Bernstein MA. Concomitant gradient field effects in spiral scans. Magn Reson Med. 1999;41(1):103-112. doi:10.1002/(sici)1522-2594(199901)41:1<103::aid-mrm15>3.0.co;2-m
Yu H, McKenzie CA, Shimakawa A, et al. Multiecho reconstruction for simultaneous water-fat decomposition and T2* estimation. J Magn Reson Imaging. 2007;26(4):1153-1161. doi:10.1002/jmri.21090
Hu HH, Börnert P, Hernando D, et al. ISMRM workshop on fat-water separation: Insights, applications and progress in MRI. Magn Reson Med Off J Soc Magn Reson Med Soc Magn Reson Med. 2012;68(2):378-388.
Kim D, Cauley SF, Nayak KS, Leahy RM, Haldar JP. Region-optimized virtual (ROVir) coils: Localization and/or suppression of spatial regions using sensor-domain beamforming. Magnetic Resonance in Medicine. 2021;86(1):197-212. doi:10.1002/mrm.28706
Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
Hori M, Hagiwara A, Goto M, Wada A, Aoki S. Low-Field Magnetic Resonance Imaging. Invest Radiol. 2021;56(11):669-679. doi:10.1097/RLI.0000000000000810
Figures
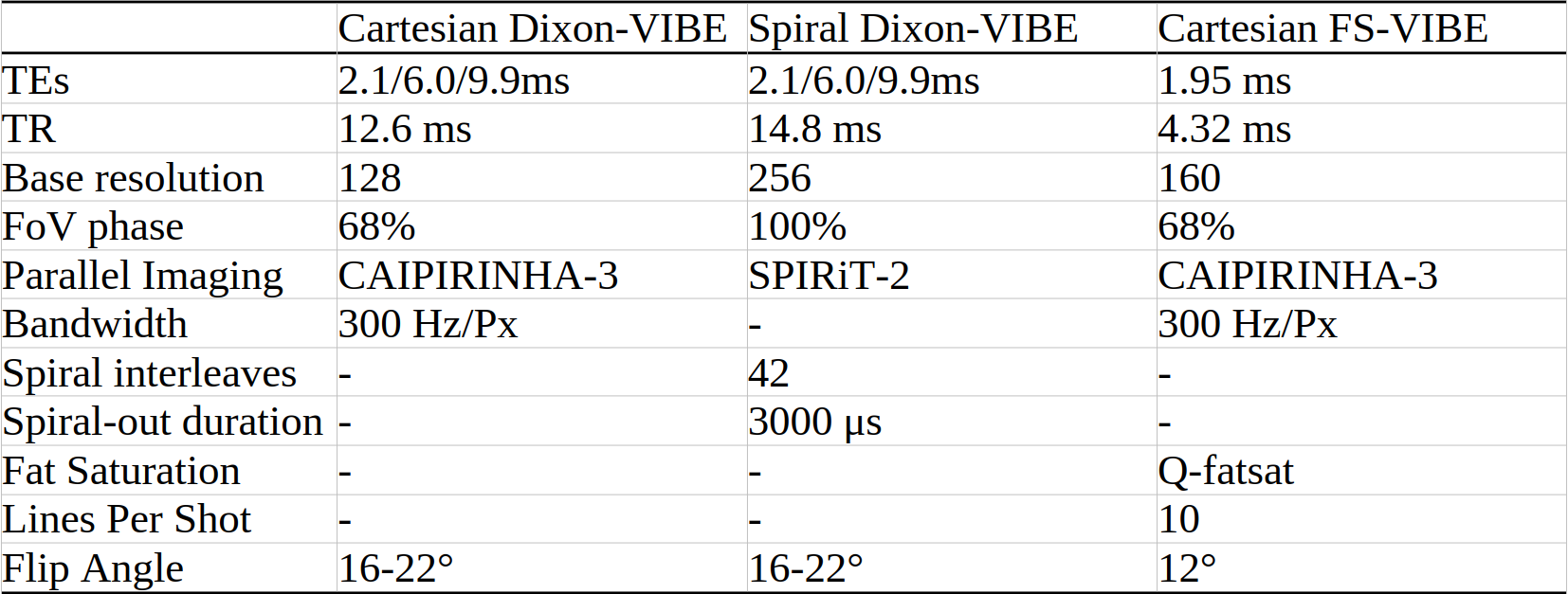
Table 1: Sequence parameters for Cartesian Dixon-VIBE, Spiral Dixon-VIBE, and Cartesian FS-VIBE.
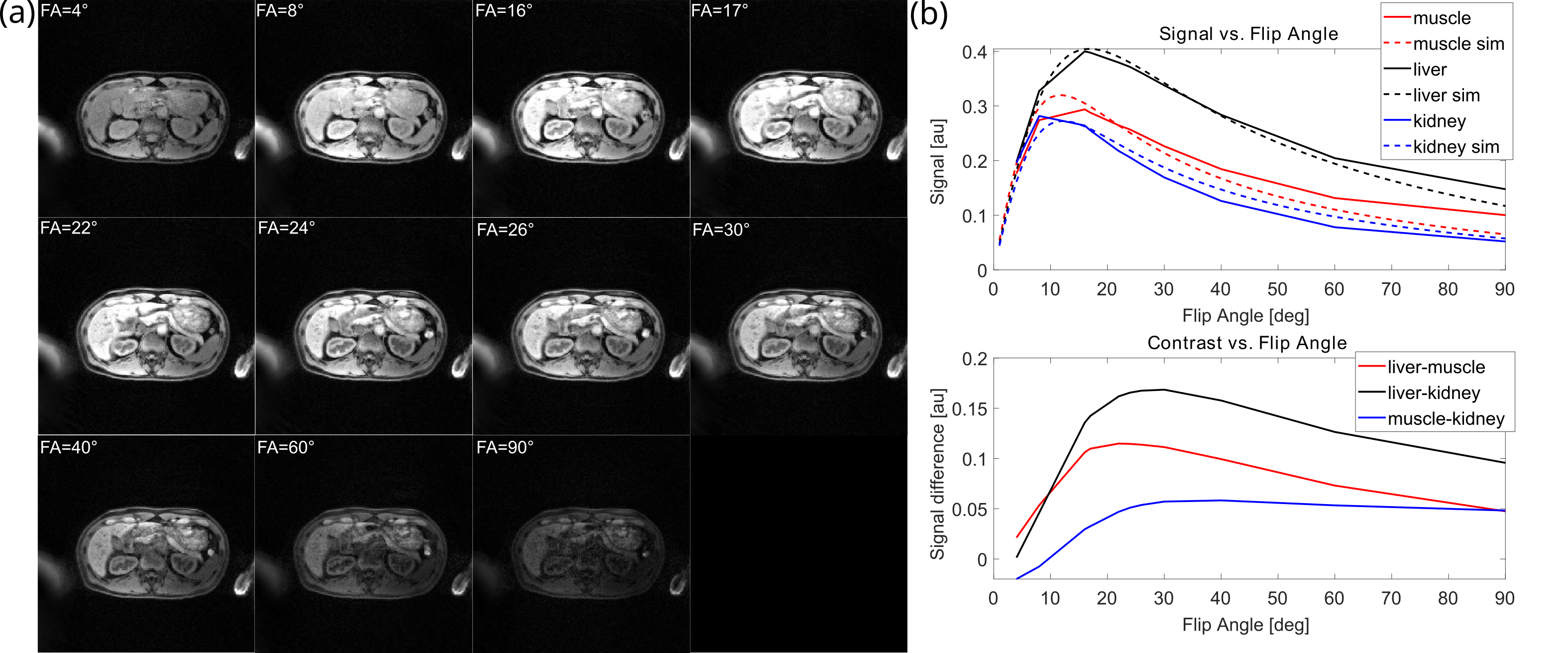
Figure 1: Optimization of Imaging Flip Angle. Eleven flip angles are tested, spanning the range from 4º to 90º. Liver, skeletal muscle, and kidney are segmented, and average signal from these tissues are plotted as a function of flip angle. Simulated curves are shown with dashed lines. A flip angle of ~17° provides the strongest overall signal, and ~24° provides the strongest contrast between tissues of interest.
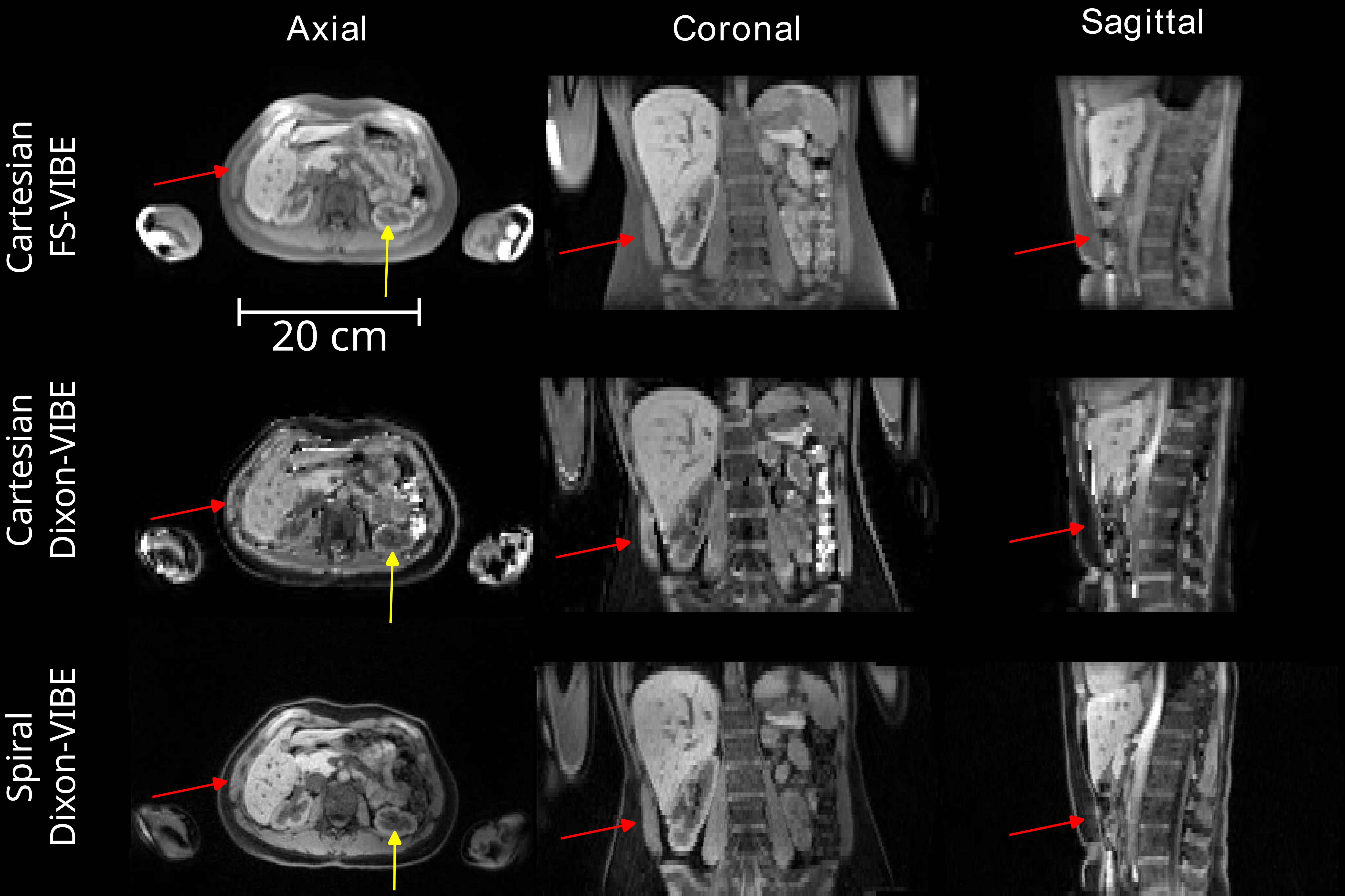
Figure 2: In-vivo results from one adult volunteer, with axial, coronal, and sagittal reformats. (top) Cartesian FS-VIBE, (middle) Cartesian Dixon-VIBE water-only, (bottom) spiral-Dixon-VIBE, each acquired in a single ~17 sec breath-hold. Fat-Sat provides insufficient fat suppression, and poor contrast between subcutaneous fat and muscle (red arrows). Cartesian and spiral Dixon-VIBE provide excellent fat suppression. Only spiral imaging provides spatial resolution necessary to resolve finer structures (yellow arrows).
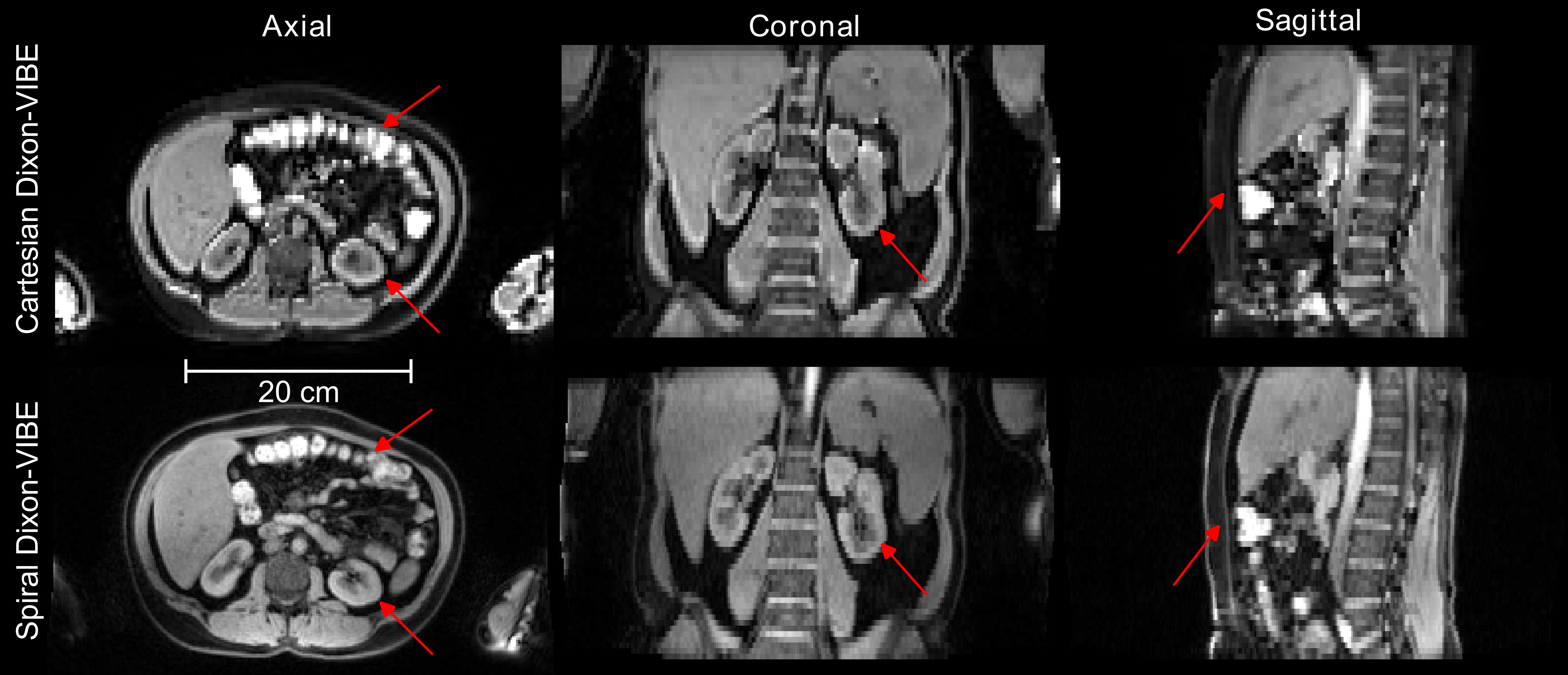
Figure 3: In-vivo comparison of Cartesian and Spiral Dixon-VIBE water-only images from a female subject with ~22% PDFF, with axial, coronal and sagittal reformats. Red arrows point to fine structures where increase in spatial resolution can be appreciated.
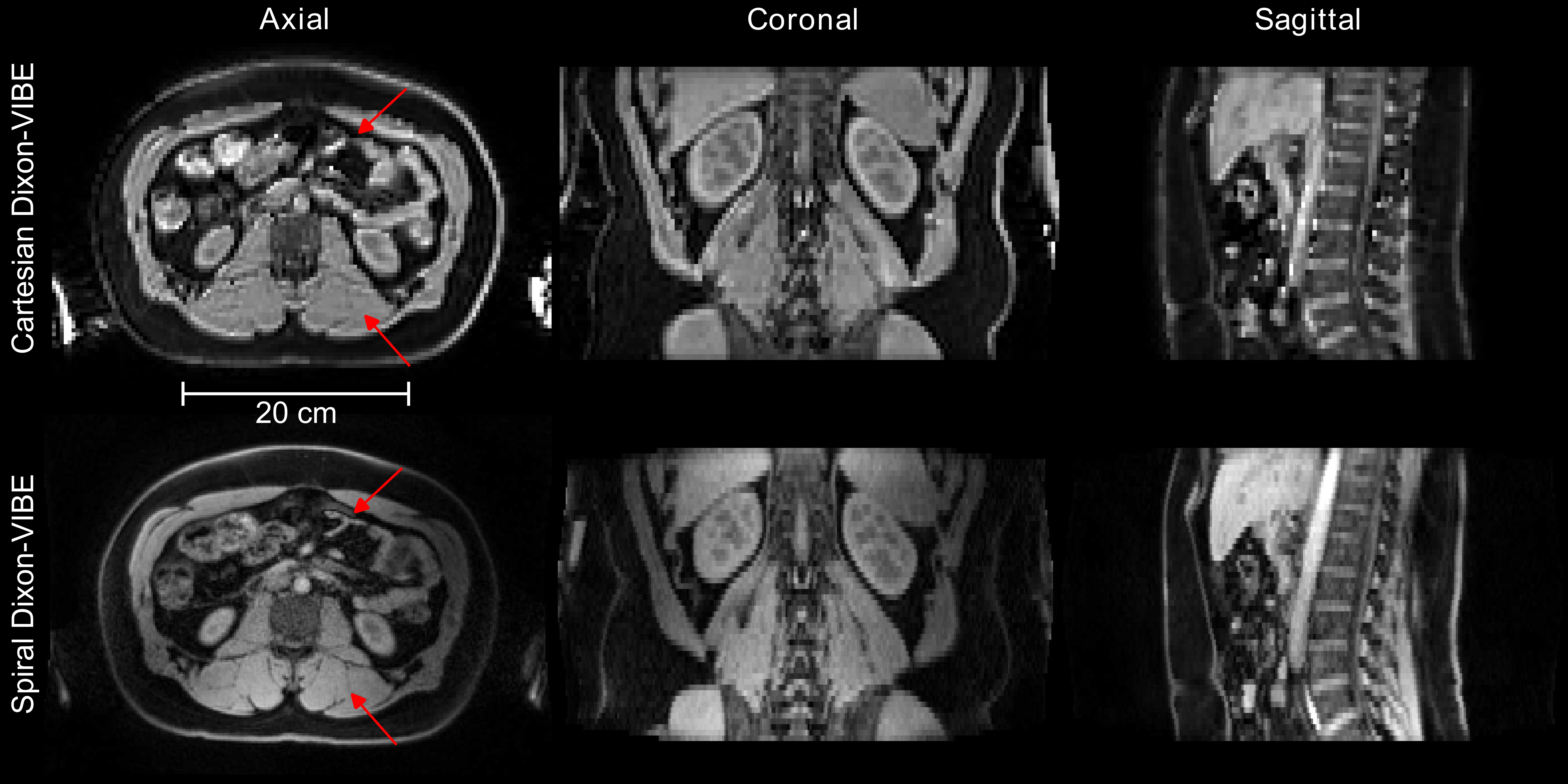
Figure 4: In-vivo comparison of Cartesian and Spiral Dixon-VIBE water-only images from a male subject with ~12% PDFF, with axial, coronal and sagittal reformats. Red arrows point to fine structures where increase in spatial resolution can be appreciated.