0424
Clinical Utility of 0.55T MRI System for the Surveillance of Intraductal Papillary Mucinous Neoplasm1Department of Radiology, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Hepatobiliary, Biliary
Motivation: Explore surveillance of Intraductal Papillary Mucinous Neoplasms (IPMN) at 0.55T, as an alternative to high field strength systems.
Goal(s): To assess the image quality at 0.55T and its impact on radiologists' confidence in evaluating IPMN versus 1.5T/3T
Approach: Images from 39 patients with IPMN who underwent 0.55T and 1.5/3T MRI were rated by 7 blinded radiologists for image quality and diagnostic certainty. Pearson correlation analysis performed
Results: A strong positive correlation existed between image quality and rater’s confidence. Negligible differences in confidence observed between 0.55T and 1.5T/3T for images with quality scores≥5.
Impact: 0.55T can be used for IPMN surveillance without compromising diagnostic effectiveness
Introduction
Intraductal Papillary Mucinous Neoplasms (IPMN) constitute the largest fraction of incidentally detected cystic pancreatic neoplasms and represent identifiable and treatable precursors of pancreatic adenocarcinoma. IPMN can involve the main pancreatic duct (MPD), branch duct(s) (BD), or both (mixed) with reported malignancy risk ranging from 38% to 68% for MPD and mixed IPMN, and 12% -47% for BD-IPMN. This necessitates effective surveillance and MRI/MRCP plays a pivotal role in clinical decision making. Stratifying IPMN into low-risk and high-risk categories is primarily based on imaging features. The risk of an IPMN progressing to cancer within 10 years is 8% for low-risk and 25% for high-risk IPMNs. With varying surveillance recommendations, some advocating lifetime surveillance, there is a need for an efficient and accessible imaging test. Commercial 0.55T MRI has emerged as a potential alternative to 1.5T/3T MRI for many abdominal indications. These systems may improve patient compliance through reduced acoustic noise and large bore size (80cm), thereby enabling imaging of larger patients and alleviating the psychological burden on patients who require frequent scans. However, lower field has lower image signal-to-noise (SNR), and thus the risk is non-diagnostic images or low reader confidence. Our aims are to determine if the image quality at 0.55T is sufficient for the evaluation of IPMN, compare image quality and diagnostic confidence at low and high fields, and establish the effect of image quality on the diagnostic confidence.Materials and Methods
We conducted a retrospective study of 39 patients with known IPMN who underwent MRI at 0.55T and 1.5T/3T. An abbreviated surveillance protocol was employed that included coronal and axial T2w HASTE, multiphase axial T1w VIBE pre- and post-contrast, coronal 3D MRCP, and 2D HASTE MRCP. Seven radiologists at various career stages assessed the overall scans independently, evaluating the type, size, and enhancement characteristics of IPMN, and image quality and diagnostic confidence on a 10-point scale (1: non-diagnostic/not confident, 10: excellent/extremely confident). Statistical analyses included Intraclass Correlation Coefficient (ICC) to measure intrarater agreement for IPMN features, image quality and diagnostic confidence; Wilcoxon matched-pairs signed rank test for assessing differences in image quality and diagnostic confidence between low and high field images; and Pearson correlation analysis to explore the relationship between image quality and diagnostic confidence.Results
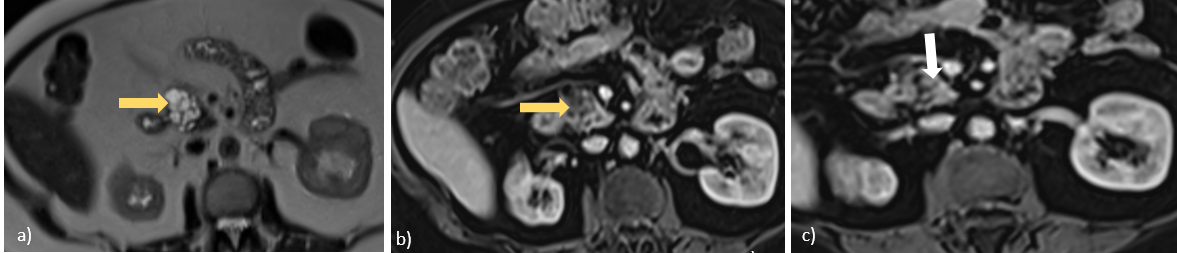
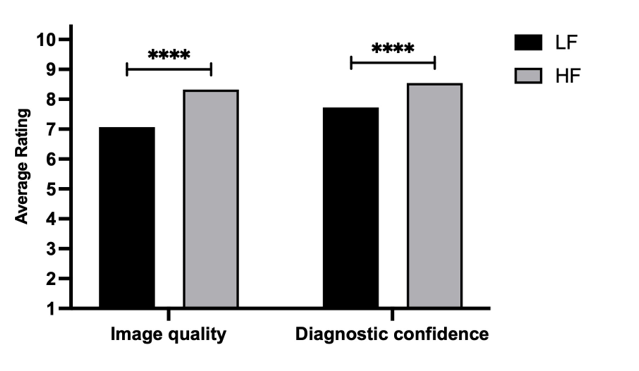
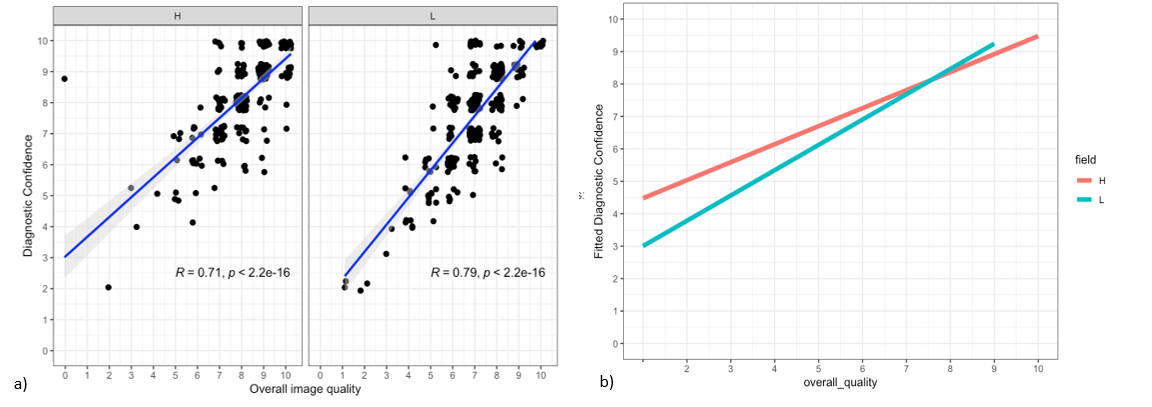
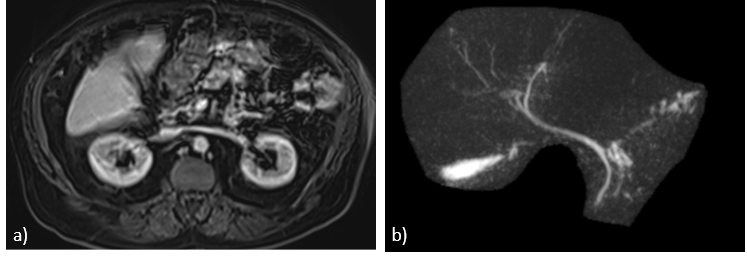
IPMN types were MPD-IPMN(n=2), mixed(n=3), and BD(n=34; 25/34 multifocal, 4 ≥3cm). Intrarater agreement at 0.55T and 1.5T/3T was moderate (k >0.41; CI 0.38-0.6) for IPMN type, size, number and location, fair (k 0.22; CI 0.07-0.37) for high-risk features (Figure 1), poor for image quality (ICC 0.1; CI:-0.01-0.22) and poor for diagnostic confidence (ICC 0.4; CI 0.28-0.47). For the cohort of readers, both image quality (p<0.0001) and diagnostic confidence (p<0.0001) scores were significantly higher at high-field when compared to low-field (Figure 2). There were significant differences in image quality scores of 6 and diagnostic confidence scores of 5 of the 7 raters. There was strong positive correlation between image quality and diagnostic confidence for both field strengths with a negligible difference in reader’s confidence when image quality score was high (≥5) (Figure 3). Only 1 of 39 0.55T scans were scored <5 (Figure 4). There were differences in confidence scores for different lesion sizes at both field strengths (no significant difference (p 0.06) for lesions ≥3cm (n=4); significant difference for 1-3cm lesions (n=16, p 0.00084) and <1cm (n=19, p 0.012).Discussion
The results indicate that there is a strong positive correlation between image quality and reader’s confidence for low and high field scans, which may be due to the predominance of small (<3 cm) IPMNs that require high quality imaging for evaluation. Our results also show loss of image quality at 0.55T compared to higher field strength, which is expected given lower SNR. However, when image quality was rated >5, there was negligible loss of diagnostic confidence, and the mean image quality scores encountered at 0.55T was >7 in 38 of 39 patients assessed in this study. Thus, 0.55T MRI appears to be a viable alternative for IPMN surveillance. However, a larger number of patients at multiple sites need to be studied, to better ascertain the frequency of diagnostic failure. The results also indicate a relationship between lesion size and diagnostic confidence, which also merits further exploration, as this presents an opportunity for both appropriate patient selection and improvement in acquisition quality, in future studies.Conclusion
Low-field MRI at 0.55T can effectively support IPMN surveillance without compromising diagnostic effectiveness. Utilizing these scanners can enhance accessibility to MRI, offering a valuable option for patient careAcknowledgements
No acknowledgement found.References
1. Matthaei H, Schulick RD, Hruban RH, Maitra A. Cystic precursors to invasive pancreatic cancer. Nat Rev Gastroenterol Hepatol. 2011 Mar;8(3):141–50.
2. Zamboni G, Hirabayashi K, Castelli P, Lennon AM. Precancerous lesions of the pancreas. Best Practice & Research Clinical Gastroenterology. 2013 Apr 1;27(2):299–322.
3. Stark A, Donahue TR, Reber HA, Hines OJ. Pancreatic Cyst Disease: A Review. JAMA. 2016 May 3;315(17):1882–93.
4. Tanaka M, Fernández-del Castillo C, Kamisawa T, Jang JY, Levy P, Ohtsuka T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017 Sep 1;17(5):738–53.
5. Choi SH, Park SH, Kim KW, Lee JY, Lee SS. Progression of Unresected Intraductal Papillary Mucinous Neoplasms of the Pancreas to Cancer: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2017 Oct;15(10):1509-1520.e4.
6. European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut. 2018 May;67(5):789–804.
7. Rusche T, Vosshenrich J, Winkel DJ, Donners R, Segeroth M, Bach M, et al. More Space, Less Noise—New-generation Low-Field Magnetic Resonance Imaging Systems Can Improve Patient Comfort: A Prospective 0.55T–1.5T-Scanner Comparison. Journal of Clinical Medicine. 2022 Jan;11(22):6705.
Figures