0421
Research use of an ultra-low-field MRI to measure child neurodevelopment at 3 and 12 months of age in Southern Malawi, Sub-Saharan Africa1Neuroscience, Training & Research Unit of Excellence (TRUE), Blantyre, Malawi, 2Kamuzu University of Health Sciences (KUHeS), Blantyre, Malawi, 3Radiology, Kamuzu University of Health Sciences (KUHeS), Blantyre, Malawi, 4Pasricha Lab, Population Health and Immunity, Walter and Eliza Hall Institute (WEHI), Voctoria, Australia, 5Developmental Imaging, Murdoch Children's Research Institute, The Royal Children's Hospital, Voctoria, Australia, 6Centre for Neuroimaging Sciences, Psychology and Neuroscience, King’s College London, London, United Kingdom, 7Hyperfine.io, London, United Kingdom, 85. Maternal, Newborn, and Child Health Discovery & Tools, Bill & Melinda Gates Foundation, Seattle, WA, United States
Synopsis
Keywords: Neuro, Low-Field MRI, Infant Brain Development; Brain MRI; Ultra-Low-Field MRI
Motivation: In Sub-Saharan Africa, limited MRI access and expertise can be addressed through international collaborations to enhance quality neuroimaging data collection in brain research.
Goal(s): We describe research usability and reliability of an ultra-low-field (64mT) MRI data collection from Zomba, Malawi.
Approach: We scanned ~481 children at 3 and 12 months of age, using hyperfine Swoop ULF-MRI (64T) for neuroimaging data to augment traditional randomized control trial outcome measures. We summarize procedures, participant responsiveness, and neuroimaging quality.
Results: Full-scan success was in over 88% of participants within 55 weeks, with 87.4 to 99.6% completing all 5 scanning sequences. Full-brain quality scans were in >79%.
Impact: International collaborations, such as UNITY project, utilizing ultra-low-field MRI improves research capacity and enables reliable measurement of brain development in Sub-Saharan Africa. This significantly promotes advancement of developmental neuroscience in the region.
INTRODUCTION
Sub-Saharan Africa, a low-resource global south region, faces significant challenges of access and expertise in magnetic resonance imaging (MRI) technology for the assessment of child neurodevelopment. This leads to a substantial gap in understanding brain development in the region1. This scarcity is particularly pronounced in research and clinical settings. International collaborations, such as the ‘Ultra-low-field Neuroimaging in The Young’ (UNITY) project, seek to address this disparity through use of portable technology, supporting feasible procedures and enabling collection of reliable quantitative neuroimaging data.We describe research usability and reliability of an ultra-low-field (64mT) MRI data collection from Zomba, Malawi.
METHODS
Participants:Participants are children coming for scheduled outcome visits at 3 and 12-month of age as part of a controlled trial investigating the developmental benefits of preventive treatments for maternal anaemia in Zomba, Malawi. A total of 403 children (49.5% female) participated at 3 months and 288 children (51.0% female) at 12 months of age, including 214 who were retested.
Procedures:
The Hyperfine Swoop ultra-low-field (64T) MRI system is successfully implemented in Malawi2. We used Localizer, triplanar T2-weighted and axial T1-weighted sequence acquisitions. A full scan acquisition averages 25 minutes. Controlled through an iPad console, image data is uploaded to a cloud platform facilitating easy access for analysis. A local team of 2 radiology technicians, 2 nurses, early child development assessors, a research scientist, was supported by a consultant radiologist and international neuroimaging researchers. Site team trained over 3 days in safety and non-sedated pediatric neuroimaging protocols 3 in addition to educational materials and mentorship through ISMRM 2023. Informed consent preceded all neuroimaging sessions, which were conducted in a designated room, minimizing possible distraction. The standard phantom was used to calibrate machine on electricity, UPS, and generator power settings. Artifacts control measures include exclusion of metallic objects and mobile phones from the scanning room. Image acquisition sequences required participants to be asleep or still. Uptake numbers and challenges were summarized and discussed weekly. In addition to visual inspection, different software versions were used to check for SSM, CHT, and motion artefacts. In addition, images were subjected to standard processing for brain volume metrics to rate quality in all three directions. Uptake is summarized using percentages of totals expected for attendance, quality as full-brain count against total recruitment. Descriptive statistics are presented for participant characteristics at both 3- and 12-month time points.
RESULTS
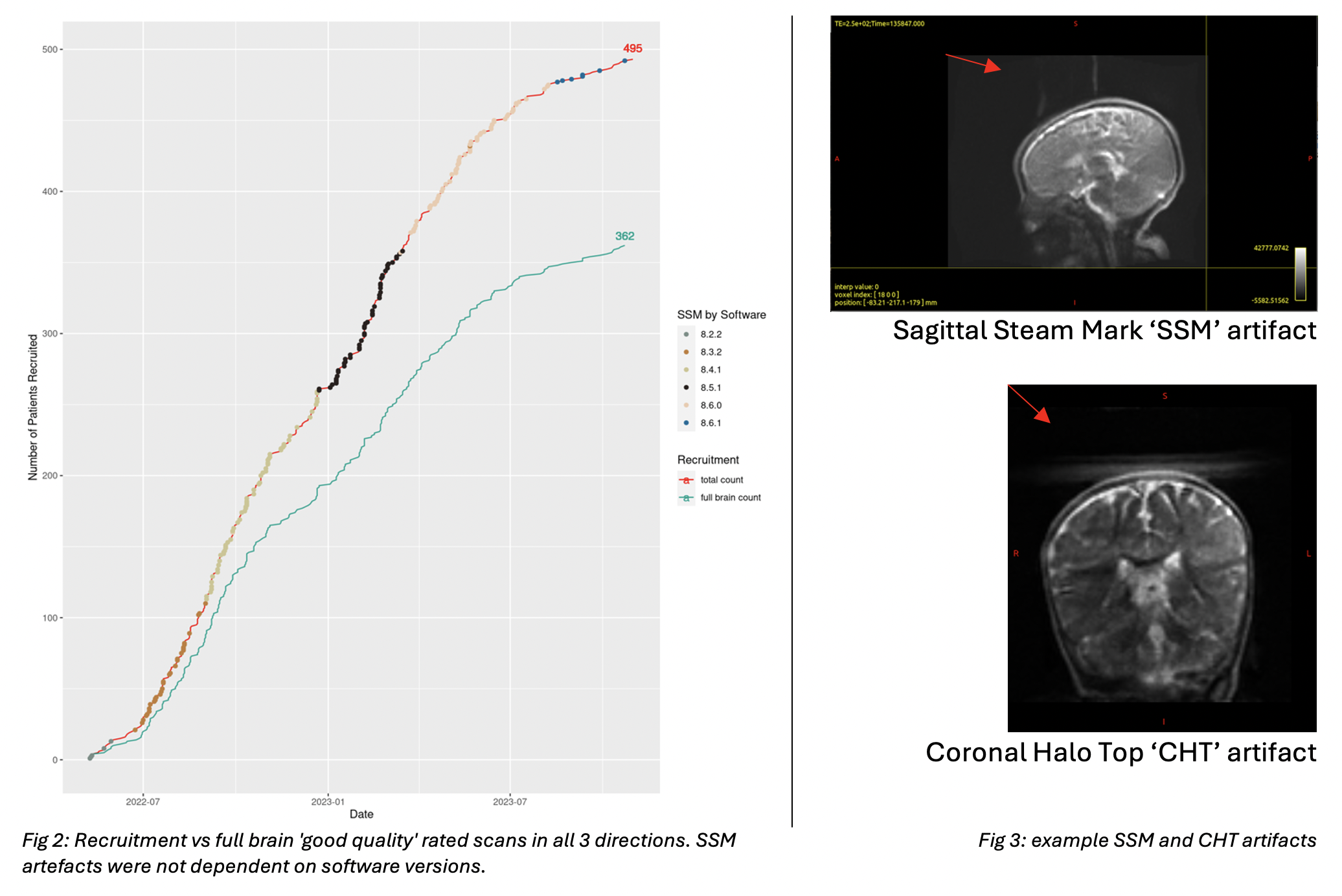
Over a 55-week period, an increasing number of participants showed up for neuroimaging averaging 14 participants weekly, with about 90.2% undergoing scan sessions. Although there were some failures primarily due to baby restlessness (81.8% 3-m, 93.0% 12-m / all failures), and other reasons, overall participant responsiveness was high with success for sequence completion across localizer, T2-AXI, T2-SAG, T2-COR, and T1-AXI ranging from 91.1% to 99.4% for 3-months-olds and from 87.4% to 99.6% for 12-month-olds [table 1]. Most scans were completed around mid-day.As at October 2023, we had a total of 3459 DICOM images of T1 and T2 (axial, coronal, and sagittal) with ~79% of good quality T2 scans in all planes. Participants with good quality scans in all planes were ~362 [fig 2].
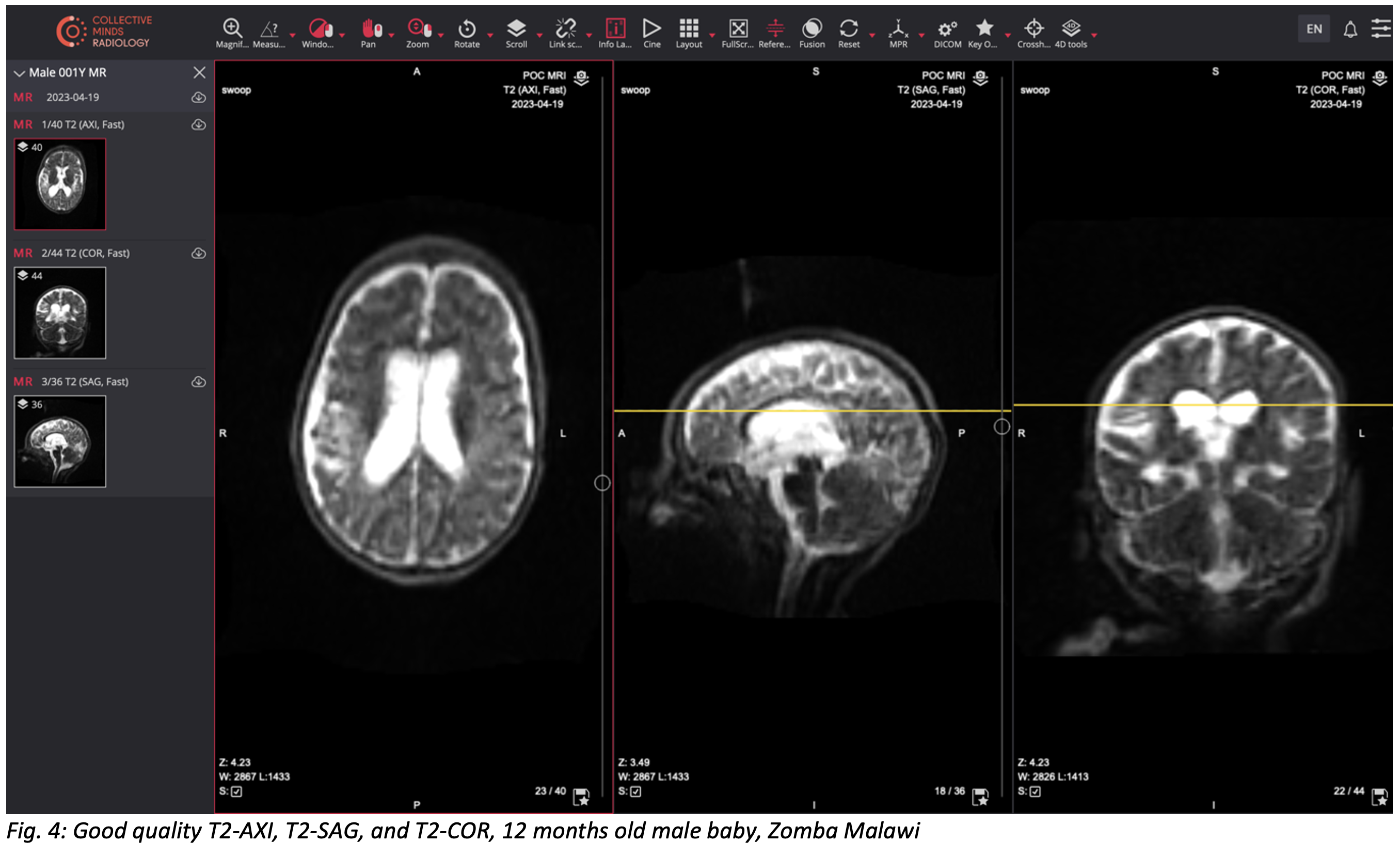
'SSM' Artefacts were prevalent in the sagittal plane, occurring in 37.3% of sagittal images, the 'CHT' artefact only occured in 4.9% of coronal images [Fig.3], while motion artifacts appeared in 10.5% of images in all planes.During an image quality webinar on CollectiveMindsRadiology platform, members of the UNITY project observed that de-identified images from Zomba showed good quality [Fig. 4].
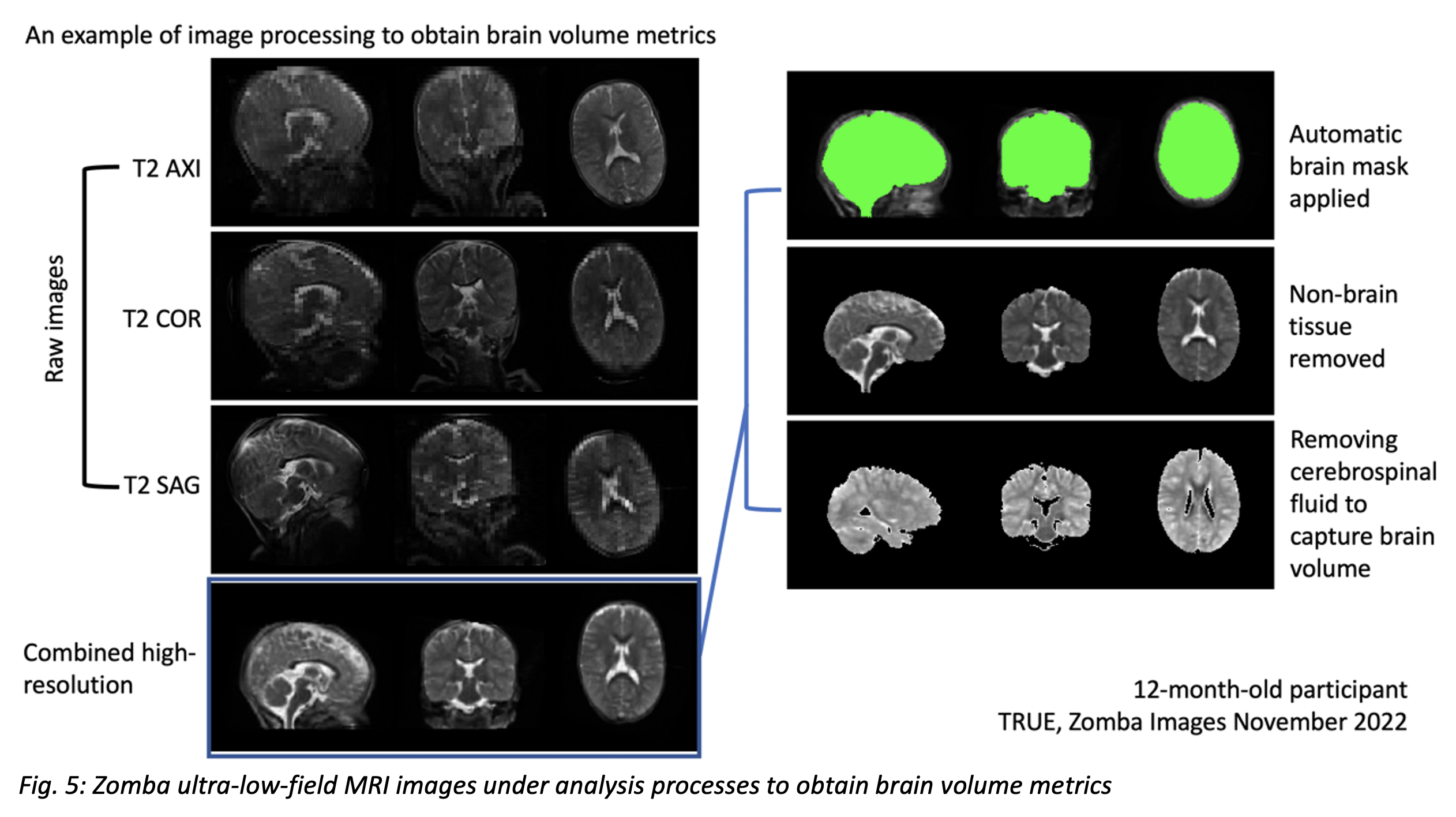
In addition, the quality of images renders them amenable to standard processing for obtaining brain volume metrics [Fig. 5].
DISCUSSION
The results suggest that an ultra-low-field MRI can be effectively used to collect neuroimaging data in a low-resource setting like Zomba, Malawi. Excellent participant responsiveness, despite occasional challenges, demonstrates the feasibility of implementing neuroimaging. The quality of data, combined with its acquiescence to standard image processing pipelines, supports the utility of this technology for studying child neurodevelopment.CONCLUSION
We demonstrate the potential of ultra-low-field MRI technology in study of child neurodevelopment in Sub-Saharan Africa. The findings provide valuable insights into the practicality of conducting neuroimaging research in regions with limited access to high-field MRI systems. The successful collection and quality of data make a compelling case for further research and clinical applications of ultra-low-field MRI in measurement of child neurodevelopment in resource-constrained areas.LIMITATIONS
We acknowledge limitations, such as participant engagement, technical issues, and limited generalizability due to studying within a controlled trial. More research will expand the utility of ultra-low-field MRI in child neurodevelopment in low-resource settings.Acknowledgements
Special thanks to UNITY consortium partners for invaluable contributions to MRI activity in Malawi. We appreciate the contribution of our international collaborators at Walter and Eliza Hall Institute, Australia. We also thank Hyperfine for their ongoing technical support. UNITY is supported by the Bill and Melinda Gates Foundation.
References
1. Deoni, S. C. L. et al. Accessible pediatric neuroimaging using a low field strength MRI scanner. Neuroimage 238, 118273 (2021).
2. Chetcuti, K. et al. Implementation of a Low-Field Portable MRI Scanner in a Resource-Constrained Environment: Our Experience in Malawi. AJNR Am J Neuroradiol 43, 670 (2022).
3. Dean, D. C. et al. Pediatric neuroimaging using magnetic resonance imaging during non-sedated sleep. Pediatr Radiol 44, 64–72 (2014).
Figures
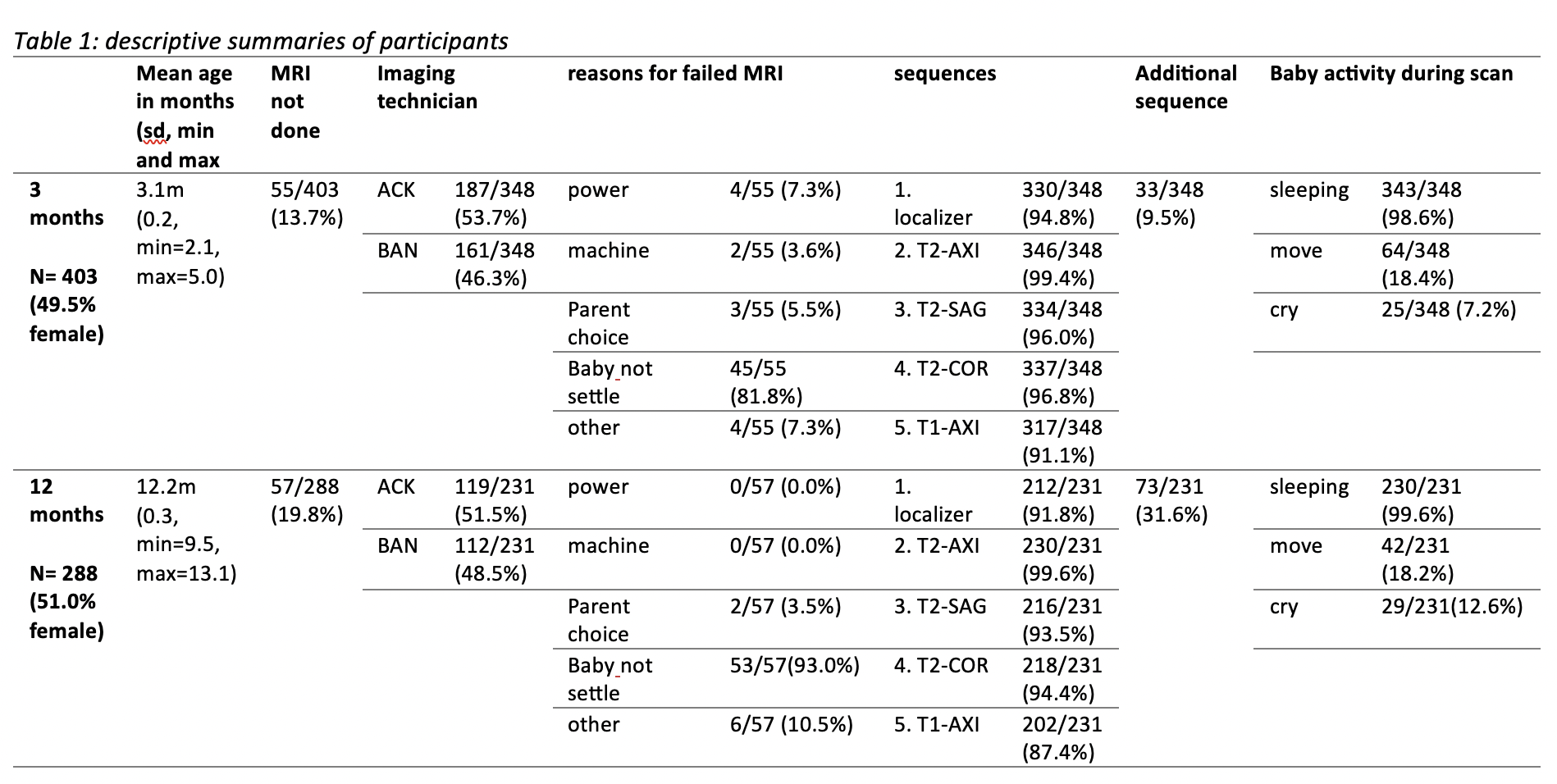
Table1: descriptive summaries of participants