0420
Facilitating access to neuroimaging and computational resources in low-resource settings through a centralised biomedical imaging platform1Department of Neuroimaging, King's College London, London, United Kingdom, 2Maternal, Newborn, and Child Health Discovery & Tools, Bill & Melinda Gates Foundation, Seattle, WA, United States, 3Flywheel, Minneapolis, MN, United States, 4Department of Pediatrics, University of Wisconsin School of Medicine and Public Health, Wisconsin, WI, United States, 5Department of Medical Radiation Physics, Lund University, Lund, Sweden, 6Department of Paediatrics and Child Health, University of Cape Town, Cape Town, South Africa, 7Neuroscience, Training & Research Unit of Excellence, Blantyre, Malawi, 8Kamuzu University of Health Sciences, Blantyre, Malawi, 9Developmental Imaging, Murdoch Children's Research Institute, The Royal Children's Hospital, Victoria, Australia, 10Makerere University, Kampala, Uganda, 11Hyperfine, London, United Kingdom, 12King's College London, London, United Kingdom, 13University of Cape Town, Cape Town, South Africa, 14Department of Radiology, Korle Bu Teach Hospital, Accra, Ghana, 15Department of Obstetrics and Gynecology, Korle Bu Teach Hospital, Accra, Ghana, 16Stavanger University, Stavanger, Norway, 17University of Southern California, Los Angeles, CA, United States, 18Department of Computer Science, University College London, London, United Kingdom, 19Cardiff University Brain Research Imaging Centre, Cardiff University, Cardiff, United Kingdom
Synopsis
Keywords: Neuro, Low-Field MRI
Motivation: MRI remains inaccessible in many parts of the world, as are the computational resources to perform neuroimaging analysis. We hope to develop resources for a growing neuroimaging community in low-resource settings.
Goal(s): To develop scalable neuroimaging tools, building capacity across low-resource settings and supporting a community for neuroimaging research.
Approach: Partnership with Hyperfine, Flywheel and numerous collaborators in sub-Saharan Africa and south Asia to collect and process MRI scans of children in the early years of life.
Results: Containerised workflows optimised for ultra-low field paediatric imaging were developed. Derived volume estimates were generated from geographically dispersed regions for further global health questions.
Impact: Multiple low-resource sites in a global consortium have generated derived volume estimates through standardised workflows of ultra-low field MR images. This enables answering of locally relevant clinical questions on factors affecting neurodevelopment, such as maternal anaemia, HIV exposure, malnutrition etc.
Introduction
Portable low-field MRI has potential to make a huge positive impact on access to MRI worldwide. In low-middle income countries (LMIC) or low-resource settings, it can provide visualisation of healthy brain development or the detrimental effects of a variety of conditions and exposures including maternal anaemia, infection, hypoxic-ischemic encephalopathy amongst others (Cawley et al., 2023; Chetcuti et al., 2022; Deoni et al., 2021). A collaborative multi-site neuroimaging project, Ultra-Low Neuroimaging in the Young (UNITY), funded by the Bill & Melinda Gates Foundation aims to develop tools and improve capacity across a network of globally dispersed partners to answer questions relating to neurodevelopment in diverse and under-served populations, contributing to global health research and addressing factors affecting neurodevelopment in low-resource settings. Initial barriers to neuroimaging analysis can be high, including limited access to advanced computational resources or prior training. One potential paradigm to overcome this is to use a centralised image storage and processing platform. Each site in the consortium has control over their project and access to neuroimaging tools and computational resources through a simple web interface where analysis can be performed in a robust, reproducible, and scalable way. We are working with Flywheel to deliver these goals. Analysis tools and workflows can be containerised on the platform as ‘gears’. These are set up to run in user-initiated or automatic ways. Through this centralised platform, there is provenance of access to data, processes run and version control for gears run, ensuring integrity and reproducibility. The current work aims to onboard partner sites to the platform, uploading scans, building and wrapping neuroimaging tools as ‘gears’ on the platform, to optimise analysis for ultra-low field imaging in paediatrics and automate processing workflows. Analysis and gear building is done collaboratively with multidisciplinary partners across the consortium.Methods
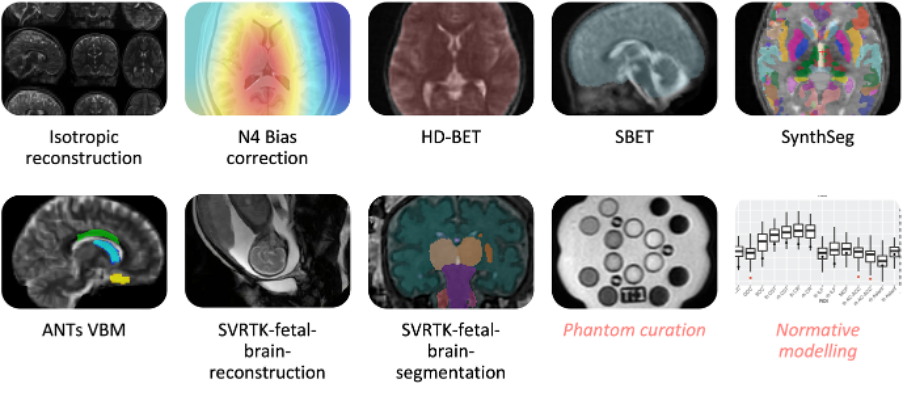
The integrated development environment (IDE) used was VS Code with GitHub and Docker add-ons as well as the Flywheel SDK. Algorithms were tested and refined for ultra-low field paediatric image processing locally before being packaged inside a Docker image and integrated with Flywheel. Dockerfiles were created, including all necessary dependencies, and libraries for frequently used neuroimaging software (ANTs, FSL, FreeSurfer). Open-source tools on GitHub, such as SynthSeg (Billot et al., 2023), HD-BET (Isensee et al., 2019), svrtk-brain-reconstruction (Uus et al., 2022) were integrated into our workflow as gears. When a functioning algorithm has been containerised, Flywheel specific requirements are integrated including a configuration file to specify inputs, outputs, and execution parameters (which can be selected by users through the GUI).Results
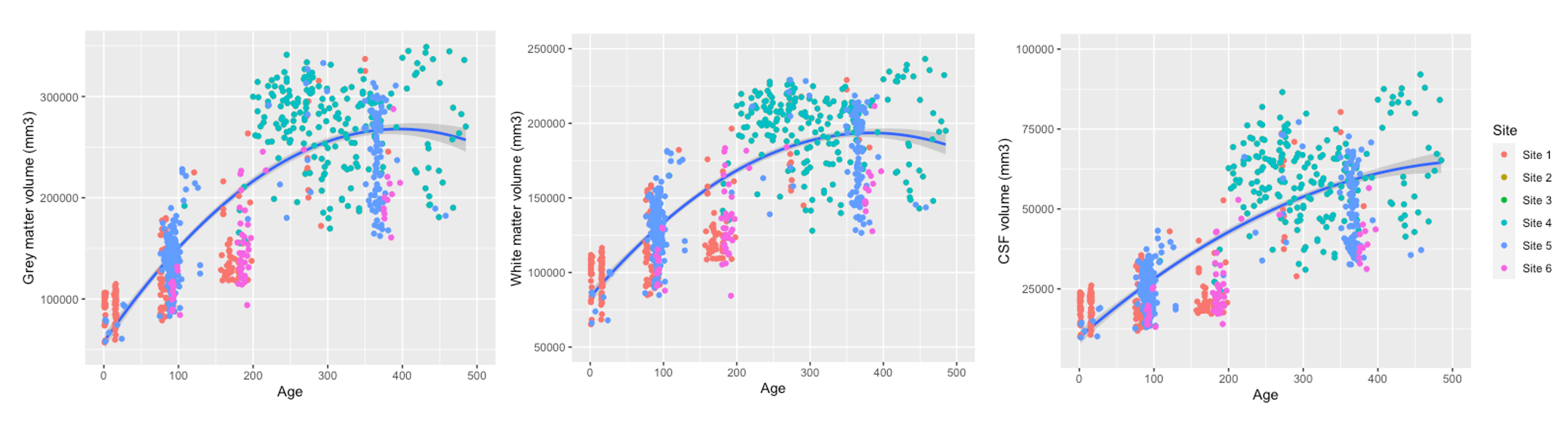
Eight projects with ultra-low field scanning (four with paired high field) and one fetal imaging project have been onboarded and are uploading scans. An additional eight are set up and ready to start scanning. An automatic workflow has been run on 1,223 scanning sessions (50% female; age range = 1-485 days), from initial reconstruction to generation of collated project volume estimates in a downloadable CSV file for further analysis. As part of this workflow, there are nine newly developed gears deployed and more under construction (Figure 1). These will be made publicly available. Each gear is set up as an isolated module and chained together under the dependency of the prior one completing. Scans uploaded are automatically classified into acquisition types and converted from DICOM to NIFTI. Quality control (QC) of the images can be performed anywhere in the world through a web-browser, allowing for collaborator input. Following image QC, initial reconstruction can be initiated by a user. Each subsequent step such as bias correction, skull stripping and volume estimation is set to run automatically upon completion of the previous step. Other tools can be selected manually or arranged as a ‘rule’ depending on project-specific needs, such as high-field fetal image segmentation or conversion of reconstructed images to DICOM for PACs upload. Derived outputs generated are standardised across projects supporting future collaboration and aggregation of data to answer global health questions (Figure 2).Discussion
Adoption of a centralized biomedical research platform has facilitated remote collaboration with partners across multiple geographical locations, improving access to neuroimaging pipelines and computational resources without the need to build local infrastructure. The automated workflows developed can be scaled to accommodate the growing consortium's needs. Further researcher training and support should be maintained with improved documentation through co-production and community support. Standardised derived measures from low-field imaging can support the evaluation of healthcare strategies and interventions where higher-resource systems are not currently feasible. This approach fosters accessibility and collaboration, ensuring the continued improvement of neuroimaging research and its applications in diverse and under-served populations.Acknowledgements
We would like to thank all the UNITY partners making invaluable contributions to the goals and objectives of the consortium. We also thank Flywheel and Hyperfine for their ongoing technical support. UNITY is supported by the Bill and Melinda Gates Foundation. The Wellcome LEAP has supported work carried out in South Africa and Malawi. Khula South Africa Data Collection Team who scanned the infants: Marlie Miles, Michal R. Zieff, Donna Herr, Layla Bradford, Lauren Davel, Simone Williams, Reese Samuels, Sadeeka Williams, Chloë A. Jacobs, Nwabisa Mlandu, Tracy Pan, Zamazimba Madi, Tembeka Mhlakwaphalwa, Thandeka Mazubane, Zayaan Goolam Nabi, Bokang Methola, Candice Knipe, and Khanyisa Nkubungu.
References
Billot, B., Magdamo, C., Cheng, Y., Arnold, S. E., Das, S., & Iglesias, J. E. (2023). Robust machine learning segmentation for large-scale analysis of heterogeneous clinical brain MRI datasets (arXiv:2209.02032). arXiv. http://arxiv.org/abs/2209.02032
Cawley, P., Padormo, F., Cromb, D., Almalbis, J., Marenzana, M., Teixeira, R., Deoni, S. C., Ljungberg, E., Bennallick, C., Kolind, S., Dean, D., Pepper, M. S., Sekoli, L., Canha, A. D., Rensburg, J. V., Jones, D. K., Bourke, N., Sabir, H., Lafayette, S. L., … Edwards, A. D. (2023). Development of neonatal-specific sequences for portable ultralow field magnetic resonance brain imaging: A prospective, single-centre, cohort study. eClinicalMedicine, 0(0). https://doi.org/10.1016/j.eclinm.2023.102253
Chetcuti, K., Chilingulo, C., Goyal, M. S., Vidal, L., O’Brien, N. F., Postels, D. G., Seydel, K. B., & Taylor, T. E. (2022). Implementation of a Low-Field Portable MRI Scanner in a Resource-Constrained Environment: Our Experience in Malawi. American Journal of Neuroradiology, ajnr;ajnr.A7494v1. https://doi.org/10.3174/ajnr.A7494
Deoni, S. C. L., Bruchhage, M. M. K., Beauchemin, J., Volpe, A., D’Sa, V., Huentelman, M., & Williams, S. C. R. (2021). Accessible pediatric neuroimaging using a low field strength MRI scanner. NeuroImage, 238, 118273. https://doi.org/10.1016/j.neuroimage.2021.118273
Isensee, F., Schell, M., Pflueger, I., Brugnara, G., Bonekamp, D., Neuberger, U., Wick, A., Schlemmer, H.-P., Heiland, S., Wick, W., Bendszus, M., Maier-Hein, K. H., & Kickingereder, P. (2019). Automated brain extraction of multisequence MRI using artificial neural networks. Human Brain Mapping, 40(17), 4952–4964. https://doi.org/10.1002/hbm.24750
Uus, A. U., Grigorescu, I., van Poppel, M. P. M., Steinweg, J. K., Roberts, T. A., Rutherford, M. A., Hajnal, J. V., Lloyd, D. F. A., Pushparajah, K., & Deprez, M. (2022). Automated 3D reconstruction of the fetal thorax in the standard atlas space from motion-corrupted MRI stacks for 21–36 weeks GA range. Medical Image Analysis, 80, 102484. https://doi.org/10.1016/j.media.2022.102484
Figures