0413
Supine breast MRI with a wearable coil (BraCoil) improves lesion localization and clinical workflow for US-guided biopsy1High Field MR Center, Center for Medical Physics and Biomedical Engineering, Medical University of Vienna, Vienna, Austria, 2Department of Biomedical Imaging and Image-guided Therapy, Division of General and Pediatric Radiology, Medical University of Vienna, Vienna, Austria
Synopsis
Keywords: Breast, Visualization
Motivation: Supine breast MRI might enable higher image correlation to supine ultrasound (US) and therefore facilitate the clinical workflow.
Goal(s): The aim was to quantify lesion displacement between supine US, prone MRI, and supine MRI in Cartesian and panoramic views, and derive the impact on the clinical workflow.
Approach: Using MRI and US patient data, the spatial lesion displacement was measured. For supine MRI a wearable breast coil (BraCoil) was used.
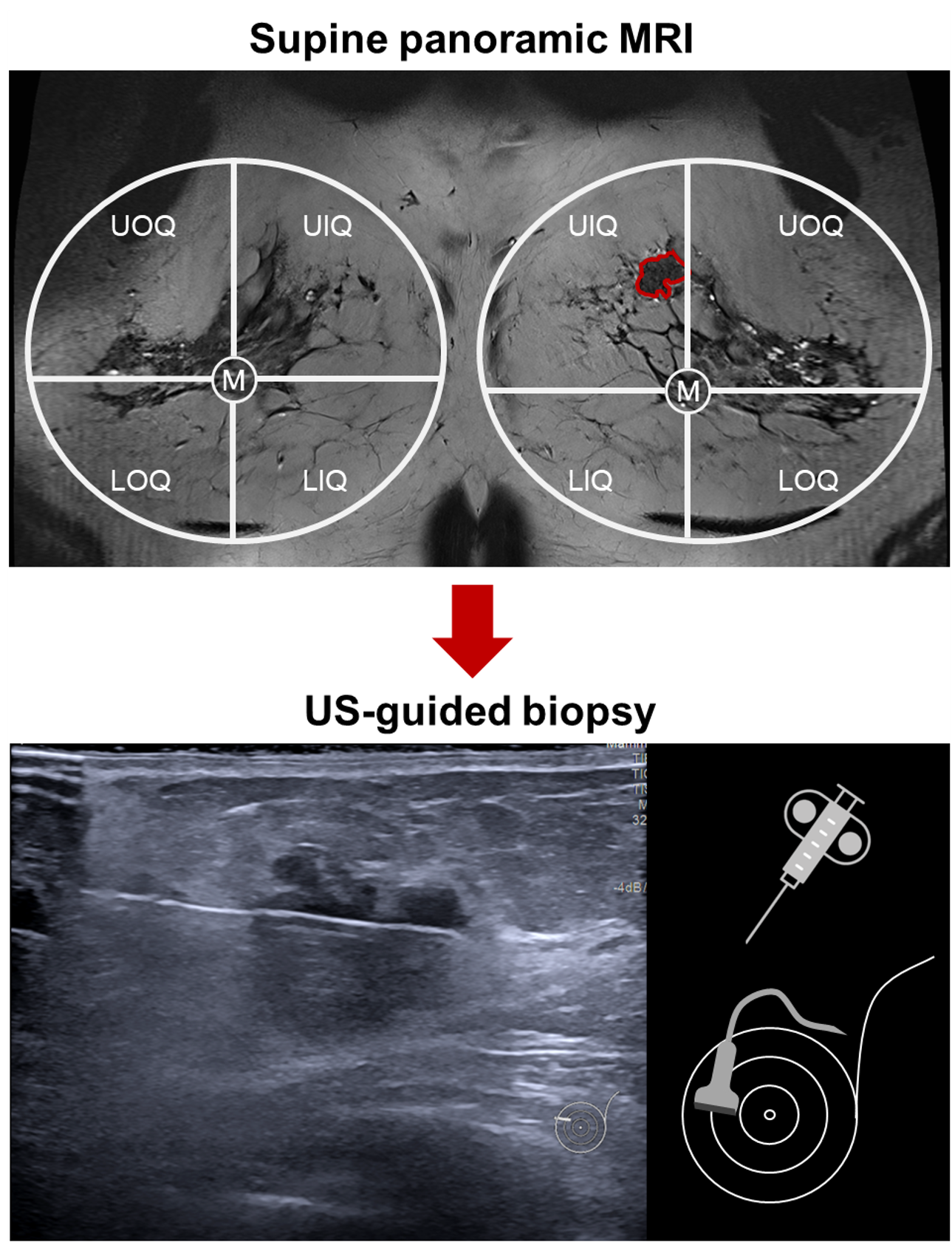
Results: Supine MRI shows comparable lesion position compared to US, in contrast to prone MRI. 18% of the lesions could only be localized in 2nd look US or biopsy after supine BraCoil MRI.
Impact: Supine breast MRI with a wearable coil could improve the clinical workflow by facilitating lesion localization for 2nd look US, biopsy, or surgery.
Introduction
Tissue deformation between standard prone breast MRI and other imaging modalities or therapeutic interventions which are performed in supine position causes considerable spatial lesion displacement1 which can complicate diagnosis and treatment. The acquisition of breast MRI in a supine position2–4 would facilitate image correlation between MRI and supine ultrasound (US)5 and therefore easier tumor localization of MRI-only lesions for US-guided biopsy, surgery or radiotherapy6.Recently, a wearable radio frequency coil vest (“BraCoil”) for supine breast MRI has been introduced4, enhancing signal-to-noise ratio significantly and improving patient comfort. The purpose of this work was to quantify the lesion displacement between supine US, standard prone MRI, and supine BraCoil MRI. The latter was read in Cartesian view and transformed to a panoramic view4 allowing for a more efficient visualization. In addition, we aim to derive the impact of supine breast MRI on the clinical workflow for US-guided biopsy following breast MRI.
Methods
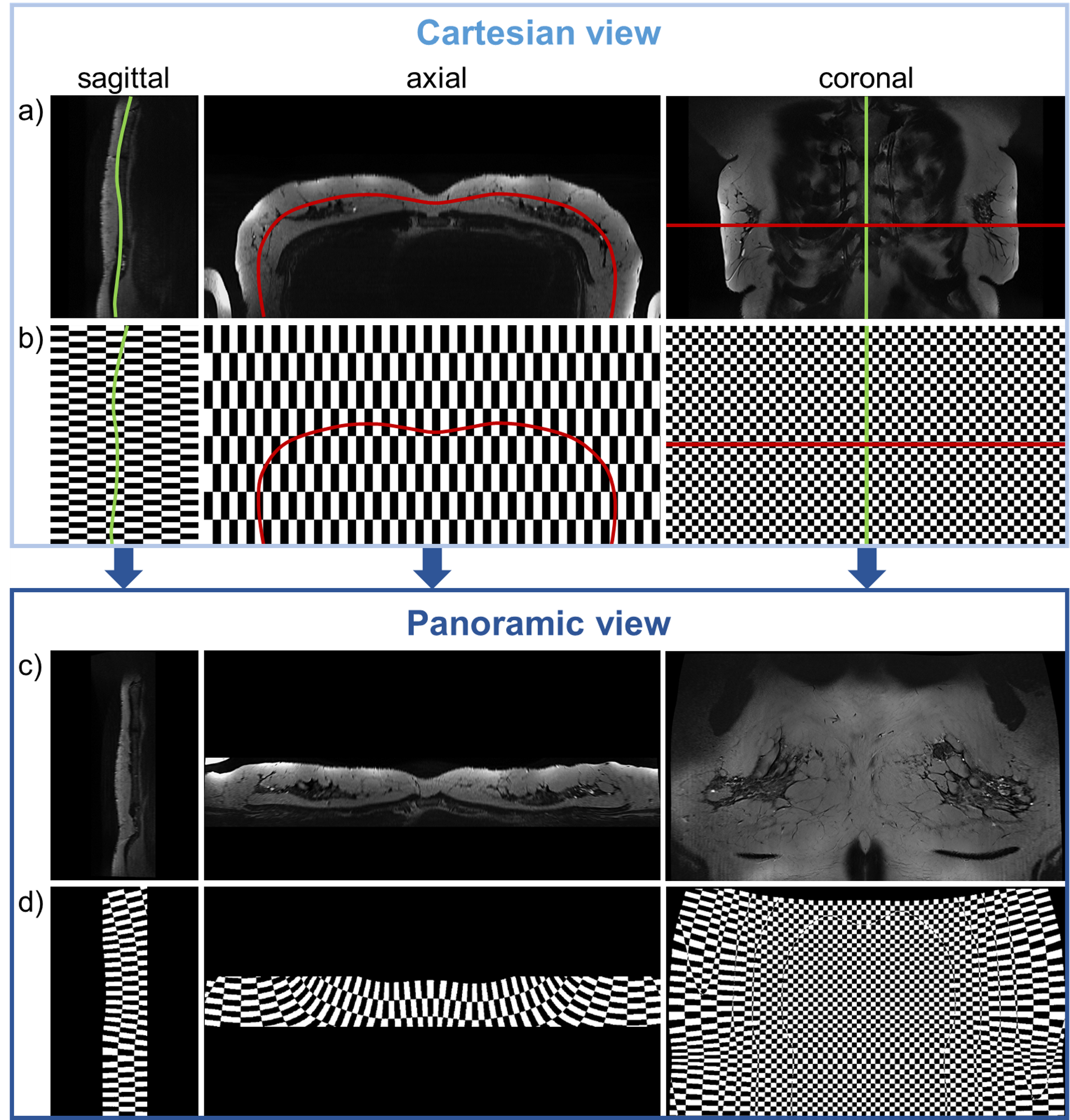
MRI and US data were acquired from 11 patients (female, 26-84 years, bra sizes 75A-100C). Each subject underwent two MRI exams using 1) a wearable breast coil4 (“BraCoil”, Fig. 1) in supine position on a 3 T MR scanner (Prisma Fit, Siemens Healthineers, Erlangen, Germany) and 2) a standard prone breast MRI at 1.5 T (3 patients) or 3 T (9 patients). The study was approved by the local ethics committee (EK No. 2137/2021) and informed written consent was obtained from all patients.Panoramic views were created using 3D Slicer7 by applying two consecutive curved planar reformatting transforms along manually drawn curves (sagittally along the sternum, and axially along the breast shape) as illustrated in Fig. 2. Volumes were cropped to the extent of the breast tissue. To visualize image distortion caused by the transform, a checkerboard patterned volume with the same image and voxel dimensions was processed the same way as breast data (Fig. 2).
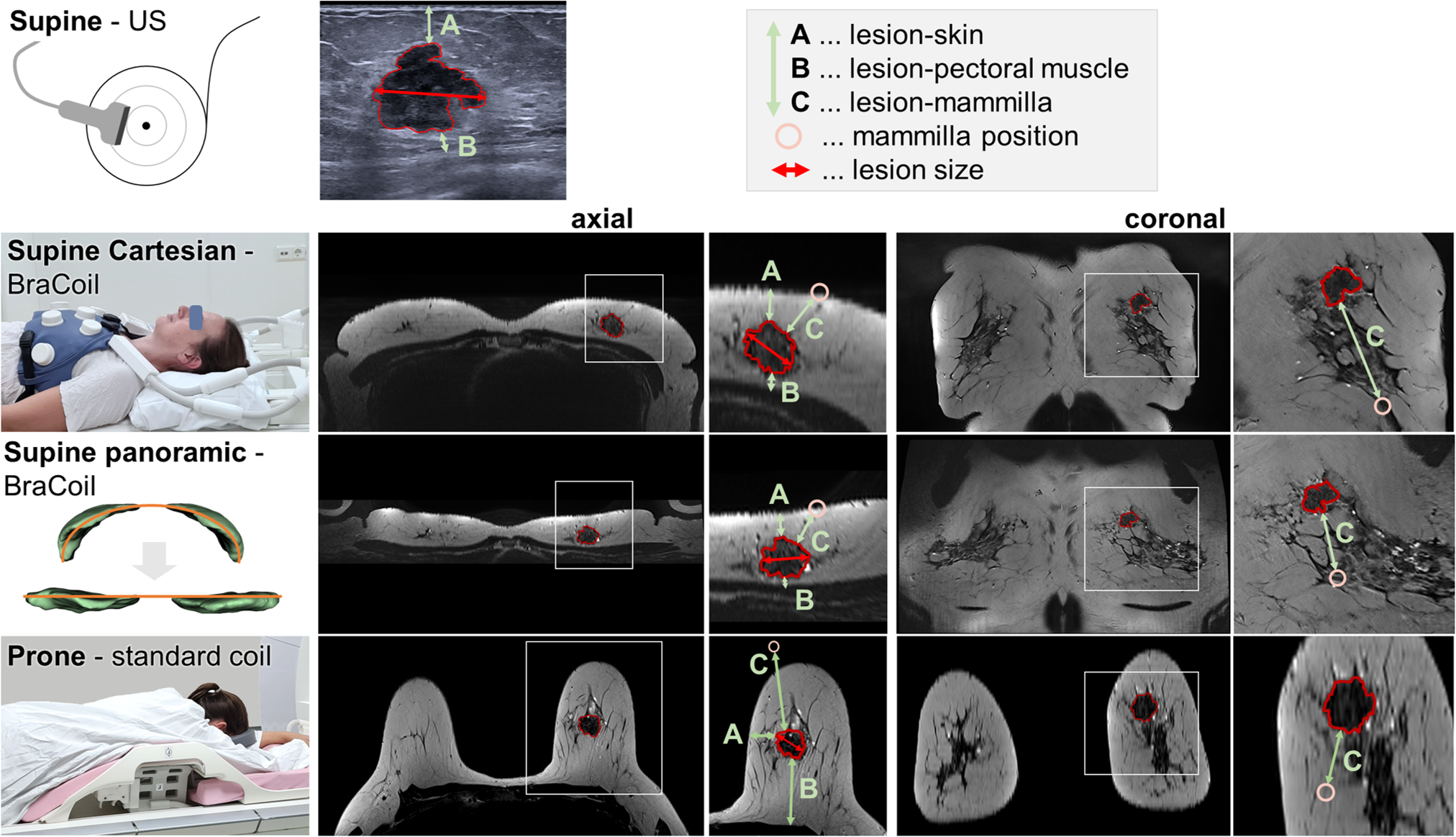
To define the spatial displacement of a lesion between different positions and visualization types, four distance measures and lesion size were compared using Cartesian supine, panoramic supine, prone MRI and supine US data (Fig. 1).
Results
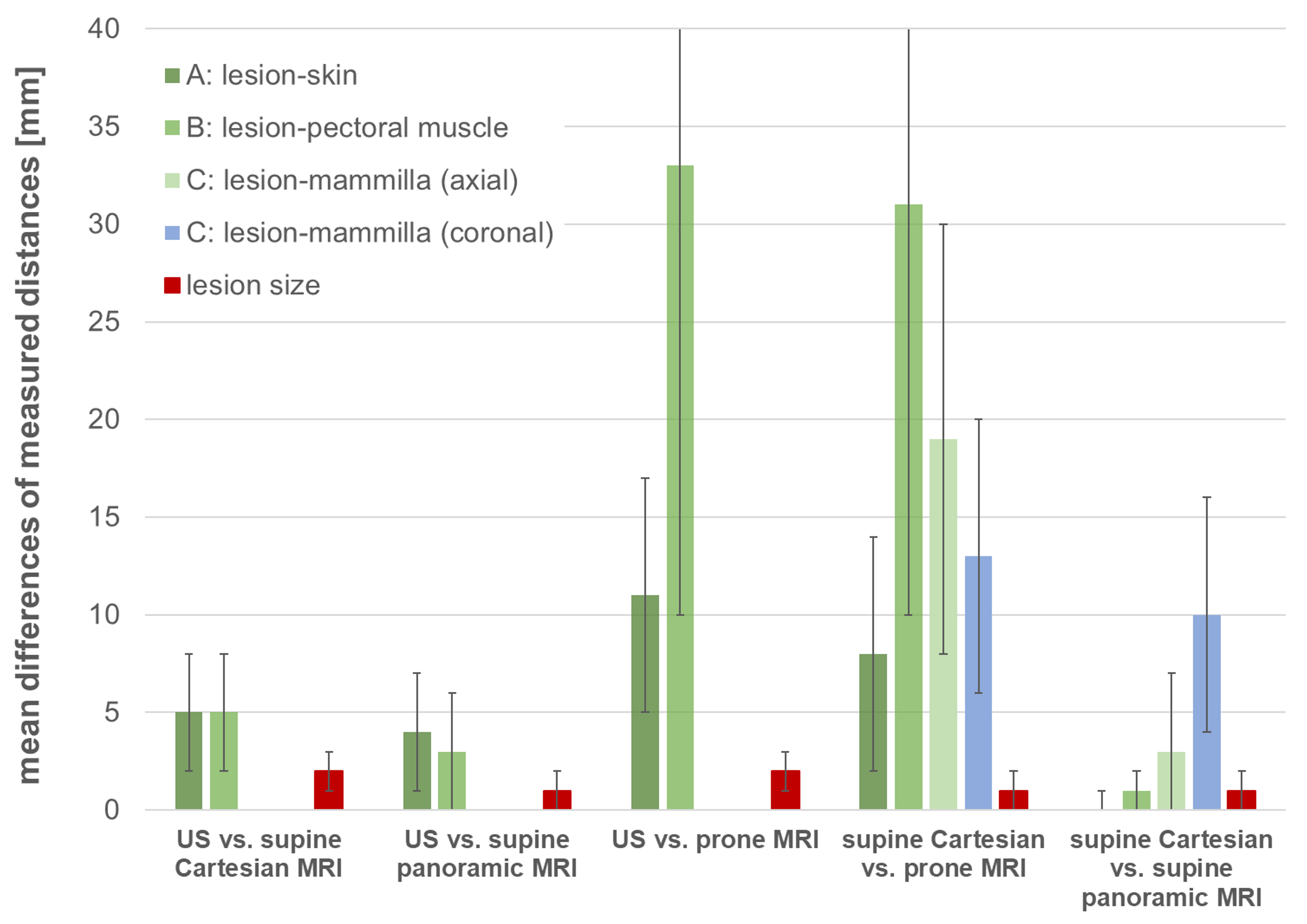
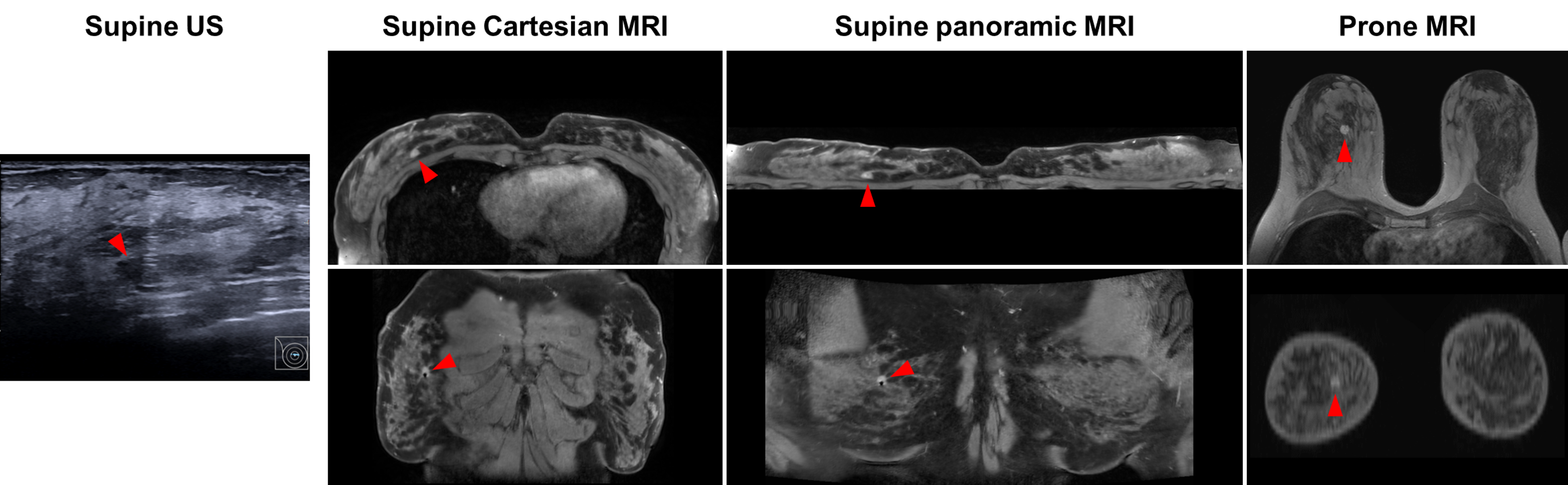
In total, 17 lesions were observed, from which 16 were further biopsied to confirm diagnosis. The calculated displacements of all lesions between supine US, prone MRI, supine Cartesian and supine panoramic MRI are summarized in Fig. 3. Considering supine US as the reference, supine Cartesian MRI had significantly less displacement than prone MRI. This is further confirmed by considerably deviating lesion positions between prone and supine MRI due to breast tissue deformation, especially in larger breasts, illustrated by the patient case in Fig. 4. In panoramic images the lesion positions were very similar to supine US and supine Cartesian MRI. Only the coronal lesion-to-mammilla displacements are slightly larger. Lesion size was consistent across all modalities. 3 out of 17 lesions (18%) could only be successfully localized in 2nd look US or US-guided biopsy after supine BraCoil MRI.Fig. 2 shows that in the panoramic view, the in-plane resolution varies from the Cartesian in-plane resolution (0.5x0.5 mm2) in the center to the Cartesian slice thickness (1.8 mm) laterally, due to the bending of the panoramic slice through the original Cartesian volume.
Discussion
In our study, supine MRI was performed with a dedicated wearable and lightweight coil vest, conserving a natural non-compressed breast shape. In addition to confirming lesion displacement between supine and prone MRI1, we assessed US and panoramic MRI distance measures. Due to limited image resolution, slight tissue deformation during US and reader-dependent distance measures, the error margin lies within a few millimeters. Differences in this range can therefore be considered negligible. From the measured lesion displacements (Fig. 3), we can conclude that the panoramic view is suitable for lesion localization. However, measured quasi-coronal distances along the breast are inherently overestimated because of the flattening.As almost 1 in 5 lesions could only be found in 2nd look US following supine MRI, its benefit for the clinical workflow might consist in a reduction of costly MR-guided biopsies. The panoramic view of supine breast MRI data enables easy and intuitive lesion description (Fig. 5).
In future studies, we aim at verifying inter-reader agreement of lesion positions, isotropic voxel acquisition, flattening following a 3D surface8, and dedicated software, correcting measured distances in quasi-coronal panoramic view.
Conclusion
We demonstrate a comparable lesion position between supine BraCoil MRI and US, in contrast to prone MRI. Integrating a panoramic view of supine breast MR data into the clinical workflow could facilitate lesion localization in 2nd look US, biopsy, or surgery.Acknowledgements
This work was funded by the joint Austrian/French grant “BRACOIL“ (Austrian Science Fund FWF Nr. I-3618/Agence Nationale de Recherche ANR-17-CE19-0022), Austrian Society for Senology (ÖGS), “MRITwins” (Horizon Europe grant, Nr. 101078393) and “CITRUS” (Horizon Europe research and innovation programme, Nr. 101071008).References
1. Carbonaro, L. A. et al. Contrast enhanced breast MRI: spatial displacement from prone to supine patient’s position. Preliminary results. Eur. J. Radiol. 81, e771–4 (2012).
2. Siegler, P., Holloway, C. M. B., Causer, P., Thevathasan, G. & Plewes, D. B. Supine breast MRI. J. Magn. Reson. Imaging 34, 1212–1217 (2011).
3. Fausto, A. et al. Feasibility, Image Quality and Clinical Evaluation of Contrast-Enhanced Breast MRI Performed in a Supine Position Compared to the Standard Prone Position. Cancers 12, (2020).
4. Obermann M & Nohava L et al. Panoramic magnetic resonance imaging of the breast with a wearable coil vest. Invest. Radiol. 58, 799–810 (2023).
5. Yoon, G. Y. et al. Feasibility of supine MRI (Magnetic Resonance Imaging)-navigated ultrasound in breast cancer patients. Asian J. Surg. 43, 787–794 (2020).
6. Groot Koerkamp, M. L. et al. Optimizing MR-Guided Radiotherapy for Breast Cancer Patients. Front. Oncol. 10, 1107 (2020).
7. 3D Slicer image computing platform. 3D Slicer https://www.slicer.org/.
8. Kretschmer, J. et al. ADR--Anatomy-Driven Reformation. IEEE Trans. Vis. Comput. Graph. 20, 2496–2505 (2014).
Figures