0410
Identification of pretreatment habitat signatures for the prediction of patient outcome in triple negative breast cancer1University of Washigton, Seattle, WA, United States, 2Vanderbilt University, Nashville, TN, United States
Synopsis
Keywords: Breast, Radiomics, habitat imaging
Motivation: Triple negative breast cancer (TNBC) patients exhibit diverse response to therapy, with ~30% achieving pathological complete response (pCR).
Goal(s): In this study, we seek to spatially-resolve heterogeneity of the tumor microenvironment using multiparametric MRI (mpMRI) in TNBC patients undergoing neoadjuvant chemotherapy to predict treatment outcomes.
Approach: We employ habitat imaging, clustering mpMRI data to identify physiologically distinct tumor subregions, or habitats. Patients are then defined by tumor habitat composition and clustered to identify common habitat signatures. Associations between habitat signatures and patient outcomes are evaluated.
Results: Clustering of patients yielded three habitat signatures with significantly different rates of pCR and recurrence-free survival.
Impact: We demonstrate that tumor habitat signatures can differentiate triple-negative breast cancer patients prior to neoadjuvant chemotherapy, identifying those with improved treatment response and long-term outcomes. Clinical translation of this approach could enable patient stratification for therapy escalation/de-escalation and treatment optimization.
Introduction
Triple negative breast cancer (TNBC) is an aggressive subtype of breast cancer associated with poorer patient prognosis and decreased overall survival compared to non-TNBC subtypes1. TNBC patients with locally advanced disease are typically treated with neoadjuvant chemotherapy (NAC), with achievement of pathological complete response (pCR) associated with improved long term outcomes2,3. However, TNBC patients exhibit diverse response to therapy, with 30-50% achieving pCR, attributable in-part to heterogeneity of the tumor microenvironment, affecting therapeutic efficacy4. Multiparametric magnetic resonance imaging (mpMRI) of the breast enables noninvasive 3D measurement of tumor microenvironment characteristics across a tumor volume. Habitat imaging is an emerging approach that leverages mpMRI data to spatially resolve intratumoral heterogeneity into physiologically-distinct tumor subregions, or habitats5. Here, we investigated whether MRI tumor habitats identified prior to initiation of NAC can be used to stratify TNBC patients and predict patient outcome.Methods
Subjects and pathologyWomen with locally advanced TNBC who underwent pre-treatment clinical breast MRI and NAC (e.g., anthracycline/taxane-based) at our institution from 2010 to 2022 were retrospectively identified for this study. Tumor size information was retrieved from patient medical records. Response to NAC was determined by pathology at surgery and pCR was defined as no residual tumor present within the breast.
MRI acquisition and analysis
Patients were scanned prior to initiation of NAC on a 3T (Achieva, Philips Healthcare) clinical scanner with a dedicated breast coil. Diffusion-weighted (DW-) MRI was acquired with a single shot echo-planar imaging sequence, using b-values = 0 and 800 s/mm2. DCE-MRI data was acquired with a fat suppressed, 3D fast gradient echo sequence with one pre-contrast and at least three post-contrast acquisitions centered at 2, 5, and 8 minutes after gadolinium-based contrast injection (0.1mmol/kg-body-weight delivered at 2cc/sec followed by a 15cc saline flush).
MRI data was corrected for patient motion using a 2D affine registration (MATLAB, MathWorks, Natick, MA) across b-values (DW-MRI) and across dynamic acquisitions (DCE-MRI). DCE-MRI was downsampled to match DW-MRI spatial resolution. To then spatially align DW and DCE-MRI, the b=0 image from DW-MRI was registered to the first post-contrast image from DCE-MRI using nonrigid registration registration6 (MATLAB, MathWorks, Natick, MA). Apparent diffusion coefficient (ADC) maps were calculated using a mono-exponential fit to registered DW-MRI data. Contrast kinetics were calculated using custom software providing voxel-wise measures of percent enhancement (PE) at 2 minutes post-contrast, signal enhancement ratio (SER), and area under the DCE-MRI curve (AUC). Tumors regions-of-interest (ROIs) were segmented using fuzzy c-means clustering of DCE-MRI data.
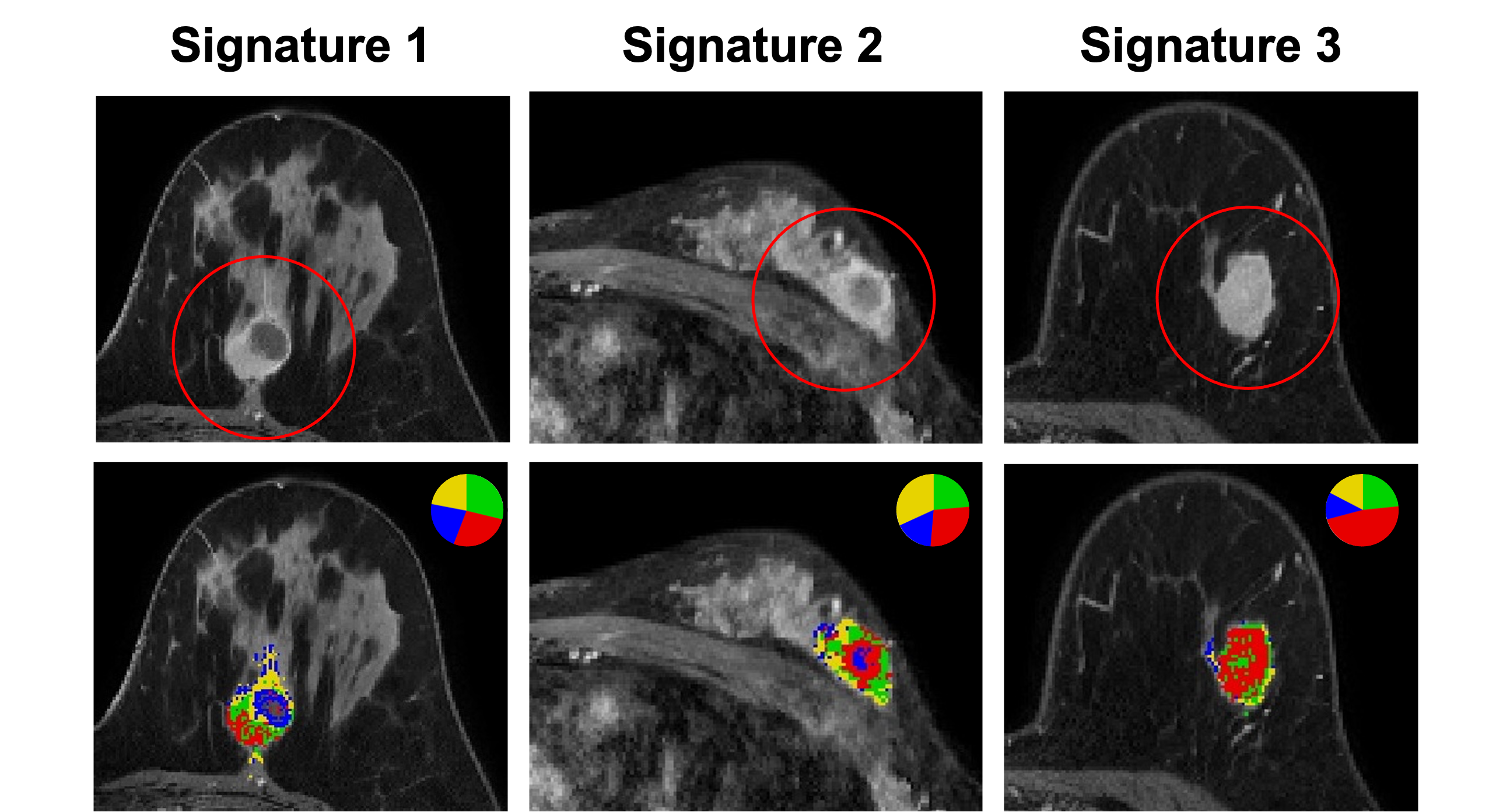
K-means clustering of multiparametric voxel data (ADC, PE, SER, AUC) was used to identify tumor habitats, with each subregion labeled in terms of “high” or “low” vascularity (DCE-MRI) and cellularity (DW-MRI) based on mean parameter values for the subregion. Each patient was then defined by features measuring the spatial distribution and size of habitats. Unique habitat signatures were identified through consensus clustering of patients.
Statistical analyses
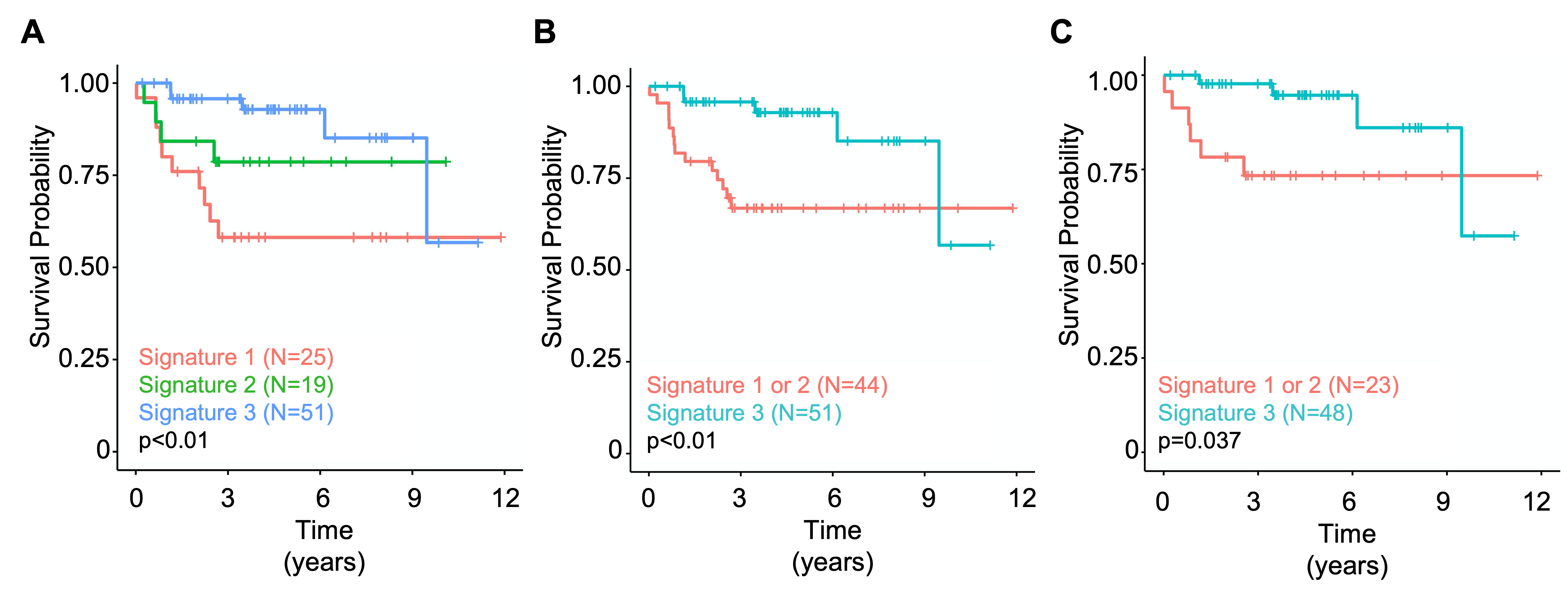
Differences in pCR rates across habitat signatures were evaluated using a chi-squared test. Recurrence-free survival (RFS) was measured as time from NAC initiation to recurrence. To evaluate association with RFS, Kaplan-Meier curves were calculated for each signature and compared using the log-rank test. A sub-analysis of patients with earlier stage (T1/T2, i.e., <50 mm) tumors was performed to evaluate associations when accounting for tumor size.
Results
Ninety-five women with TNBC were retrospectively identified (median age: 48, range 30-78 yrs), of which 33 (35%) achieved pCR. Clustering of patients yielded three habitat signatures (Signatures 1, 2, 3) that exhibited different pCR rates (Signature 1, 16%; Signature 2, 31%; Signature 3, 45%; p=0.04) and were significantly associated with RFS (Figure 1, p<0.01). Signature 3 patients demonstrated longer RFS compared to Signatures 1 and 2 when considering all patients (p<0.01) and those with T1/T2 tumors (p=0.04). Figure 2 shows example habitat maps from three distinct patient of each identified habitat signature.Discussion & Conclusion
Our findings suggest multiparametric MRI can identify distinct tumor habitats prior to treatment, which are predictive of patient outcome. Signature 3 patients demonstrated higher rates of pCR and longer RFS compared to other signatures. In the current era of immunotherapy7, these patients may represent a “low-risk” group for whom standard chemotherapy is sufficient. Clinical translation of this approach could enable patient stratification for therapy escalation/de-escalation, allowing for personalization and optimization of regimens. Future work will validate habitat signatures in external datasets and explore their predictive value in women with TNBC undergoing immunotherapy-supplemented neoadjuvant regimens.Acknowledgements
Supported by NIH grants P30CA015704, R01CA248192, Roger E. Moe Fellowship, ASCO/CCF Hayden Family Foundation Young Investigator Award in Breast Cancer, UW Medicine Institute of Medical Data Science Pilot Award.References
- Liedtke, C. et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. J. Clin. Oncol. 26, 1275–1281 (2008).
- Golshan, M. et al. Breast Conservation After Neoadjuvant Chemotherapy for Triple-Negative Breast Cancer: Surgical Results From the BrighTNess Randomized Clinical Trial. JAMA Surg. 155, e195410 (2020).
- Schmid, P. et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 382, 810–821 (2020).
- Bianchini, G., De Angelis, C., Licata, L. & Gianni, L. Treatment landscape of triple-negative breast cancer — expanded options, evolving needs. Nat. Rev. Clin. Oncol. 19, 91–113 (2022)
- Jardim-Perassi, B. V., Martinez, G. & Gillies, R. Habitat imaging of tumor evolution by magnetic resonance imaging (MRI). in Radiomics and Radiogenomics (eds. Li, R., Xing, L., Napel, S. & Rubin, D. L.) 115–120 (Chapman and Hall/CRC, 2019). doi:10.1201/9781351208277-7.
- Vercauteren, T., Pennec, X., Perchant, A. & Ayache, N. Diffeomorphic demons: Efficient non-parametric image registration. NeuroImage 45, S61–S72 (2009).
- Conroy, M. & Naidoo, J. Immune-related adverse events and the balancing act of immunotherapy. Nat. Commun. 13, 392 (2022).
Figures