0408
Classification of Breast Edema on T2-weighted imaging for predicting sentinel lymph node metastasis and biological behavior in breast cancer1Yijishan Hospitial, Wuhu, China, 2MR Research Collaboration Team, Diagnostic Imaging, Siemens Healthineers Ltd, Shanghai, China, Shanghai, China
Synopsis
Keywords: Breast, Breast
Motivation: Predicting sentinel lymph node (SLN) metastasis and biological behavior in patients with early-stage breast cancer is important.
Goal(s): To determine whether preoperative classification of breast edema can predict SLN metastasis and biological behavior in patients with early-stage breast cancer.
Approach: Breast edema was scored on a scale of 1 to 4 on T2WI to explore additional predictive value of the breast edema score (BES) model.
Results: The combined BES model significantly improved the predictive performance of SLN metastasis.
Impact: Breast edema on T2-weighted imaging can be used to predict SLN metastasis in breast cancer, helping clinicians to develop individualized treatment plans and evaluate prognosis.
Introduction
Lymph node involvement in patients with breast cancer is a key determinant of the stage, treatment, and prognosis of the disease [1,2]. The sentinel lymph node (SLN), as the first station for local tissue drainage, is the first lymph node to metastasize in most tumors. Historically, axillary lymph node dissection (ALND) was performed for lymph node management and staging of all invasive breast cancers [3,4]. Some studies showed that SLN biopsy (SLNB) and ALND had similar effects on the overall survival of patients with clinically negative lymph nodes at the long-term follow-up [5]. However, SLNB is still an invasive procedure that can lead to complications [6]. Breast edema is one of the prognostic factors of breast cancer and may be related to tumor angiogenesis, increased vascular permeability, lymphatic vascular invasion, disturbance of lymphatic drainage, and peritumoral stromal tissue hydration [7]. One study divided breast edema into three different types: peritumoral edema, prepectoral edema, and subcutaneous edema. Each type demonstrated different mechanisms and indicated different severities based on location and pathological etiology [8]. Breast edema has been studied as a critical predictor associated with the outcome of patients with invasive breast cancer [9]. However, these studies did not always separate these various types of breast edema or examine the relationship between each type and SLN metastasis. Therefore, the present study was performed to determine whether classification of breast edema on T2-weighted imaging (T2WI) can predict SLN metastasis and to elucidate the relationship between subtypes of edema and biological behavior in early-stage breast cancer.Methods
This retrospective study involved 341 women with breast cancer who underwent breast MRI. To detect the SLN, blue dye was injected before or at the time of surgery, and all nodes containing blue dye were submitted for frozen section as SLNs. All examinations were performed on a 1.5T MR system (MAGNETOM Avanto Siemens Healthcare, Erlangen, Germany). Axial T1-weighted imaging parameters were: TR: 7.83ms, TE:4.78ms, FOV:340*340mm, Resolution:342*384, slice thickness:1.5mm, slices:96, scan time:2.09min; axial fat-suppressed T2WI parameters were: TR: 5600ms, TE:59ms, TI:170ms,FOV:340*340mm, Resolution:314*320, slice thickness:4mm, slices:34, scan time:2.09min; DWI was performed with the parameters: TR: 7100ms, TE:87ms, FOV:216*359mm, Resolution:140*292, B values: 0/800 s/mm2,slice thickness:4mm, slices:58, scan time:2.17min; Eight-phase dynamic contrast-enhanced MRI was performed with a gadolinium-based contrast agent intravenously power-injected at a rate of 2 ml s−1 and dose of 0.2ml kg−1 followed by 20ml of saline, using a fat-suppressed T1-weighted gradient-echo sequence. Breast edema was scored on a scale of 1 to 4 on T2WI [LMX2] (1, no edema; 2, peritumoral edema; 3, prepectoral edema; and 4, subcutaneous edema). Clinicopathological information were collected for all patients, including: SLN status, estrogen receptor status, progesterone receptor status, human epidermal growth factor receptor type 2 (HER2) status, Ki-67, and histologic grade A logistic regression model was used for univariate and multivariate analyses. The AUC values of breast edema, breast edema score (BES), clinicopathological and combined BES and clinicopathological were calculated to examine the addition predictive value, and compared with Delong test.Results
Logistic regression analysis showed that breast edema was an independent risk factor for sentinel lymph node metastasis. The combined BES model significantly improved the predictive performance of sentinel lymph node metastasis compared with the clinicopathological model alone (AUC, 0.77 vs. 0.71; p = 0.005). In the correlation analysis, the BES was significantly positively correlated with the tumor diameter (r = 0.492, p < 0.001), histologic grade (r = 0.177, p = 0.001), Ki-67 index (r = 0.268, p < 0.001), and non-luminal subtypes (r = 0.222, p < 0.001). The results of the univariable and multivariable logistic regression analyses for SLN metastasis are shown in Table 2.Discussion
Our results indicate that these types of tumors are more likely to have SLN metastasis than tumors without breast edema. Our study further divided breast edema into BES 2, BES 3, and BES 4 because each type of breast edema may have its own etiology, and this study showed that BES 2, 3, and 4 were significantly different from BES 1 and exhibited positive trends for SLN metastasis. Besides a significant positive correlation between the BES and tumor diameter and indicated that the probability of SLN metastasis increases with the tumor diameter, which support the evidence found in a previous study [10].Conclusion
The BES on T2WI is useful for predicting sentinel lymph node metastasis. A higher grade of breast edema is associated with breast cancer aggressiveness and increases the probability of sentinel lymph node metastasis.Acknowledgements
Breast edema on T2-weighted imaging can be used to predict SLN metastasis in breast cancer, helping clinicians to develop individualized treatment plans and evaluate prognosis.References
1.Chang JM, Leung JWT, Moy L, Ha SM, Moon WK.Axillary Nodal Evaluation in Breast Cancer: State of the Art. Radiology 2020;295(3):500-515.
2.Qiu PF, Liu JJ, Wang YS, Yang GR, Liu YB, Sun X, Wang CJ, et al.. Risk factors for sentinel lymph node metastasis and validation study of the MSKCC nomogram in breast cancer patients. Jpn J Clin Oncol 2012;42:1002–1007.
3.Chung HL, Le-Petross HT, Leung JWT. Imaging Updates to Breast Cancer Lymph Node Management. Radiographics 2021;41(5):1283-1299.
4.Mamounas EP, Kuehn T, Rutgers EJT, von Minckwitz G. Current approach of the axilla in patients with early-stage breast cancer. Lancet 2017;31451-31454:S0140–S6736.
5.Krag DN, Anderson SJ, Julian TB, Brown AM, Harlow SP, Ashikaga T, et al.. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer:results from the NSABP B-32 randomised phase III trial. Lancet Oncol 2007;8(10):881–888.
6.Giuliano AE, Ballman KV, McCall L , Beitsch PD, Brennan MB, Kelemen PR, et al.. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017;318(10):918–926.
7.Cheon H, Kim HJ, Lee SM , Cho SH, Shin KM, Kim GC, et al.. Preoperative MRI features associated with lymphovascular invasion in node-negative invasive breast cancer: a propensity-matched analysis. J Magn Reson Imaging 2017;46:1037–1044.
8.Uematsu T. Focal breast edema associated with malignancy on T2-weighted images of breast MRI: peritumoral edema, prepectoral edema, and subcutaneous edema. Breast Cancer 2015;22:66–70.
9.Panzironi G, Moffa G, Galati F , Marzocca F, Rizzo V, Pediconi F. Peritumoral edema as a biomarker of the aggressiveness of breast cancer: results of a retrospective study on a 3 T scanner. Breast Cancer Res Treat 2020;181:53–60.
10.Harada TL, Uematsu T , Nakashima K , Sugino T, Nishimura S, Takahashi K, et al.. Is the presence of edema and necrosis on T2WI pretreatment breast MRI the key to predict pCR of triple negative breast cancer. Eur Radiol 2020;30(6):3363–3370.
Figures
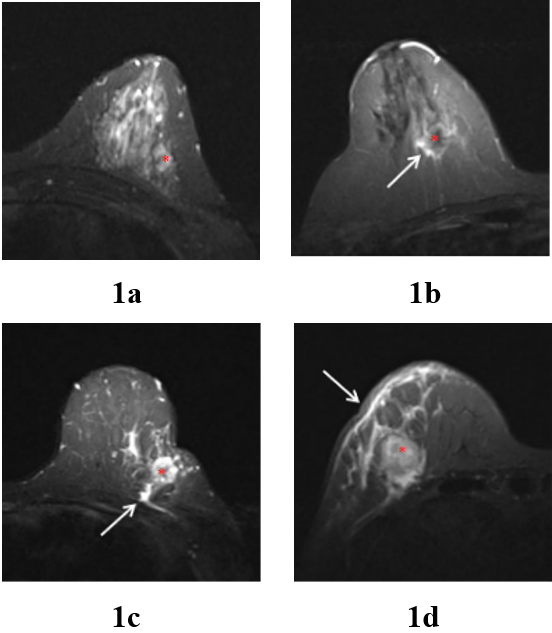
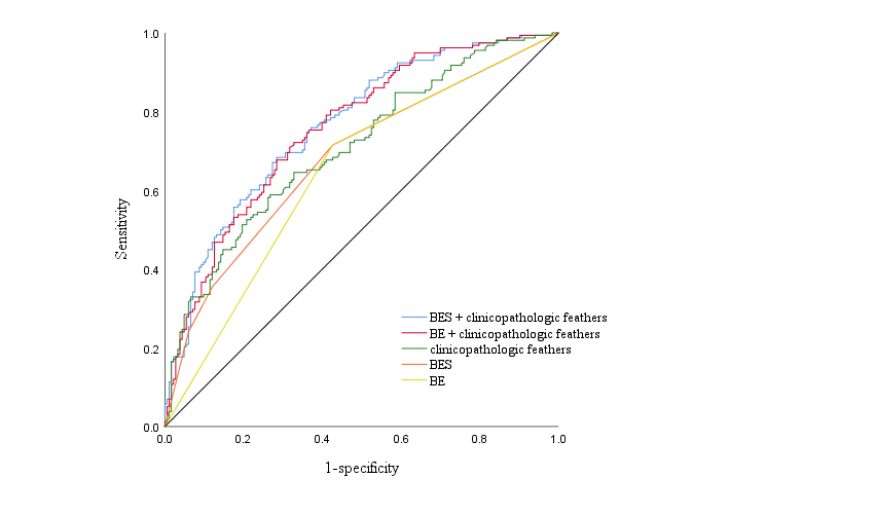
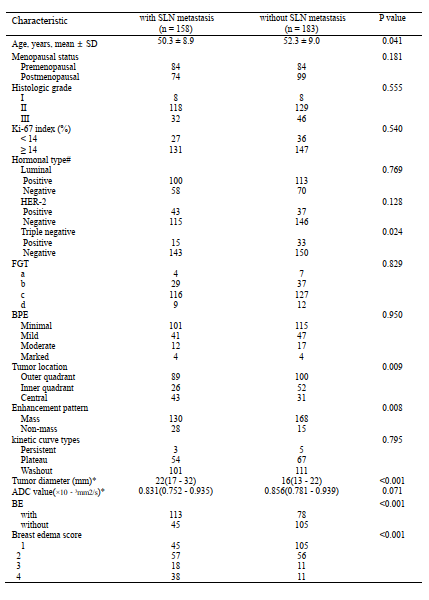
Table 1. Comparison of MRI and clinicopathologic characteristics in patients with and without SLN metastasis.
Note.—Except where indicated, data are numbers of patients. SLN, sentinel lymph node; HER2, human epidermal receptor 2; FGT, fibroglandular tissue; BPE, background parenchymal enhancement; ADC, apparent diffusion coefficient; BE, breast edema. * Data are medians, with interquartile ranges in parentheses.
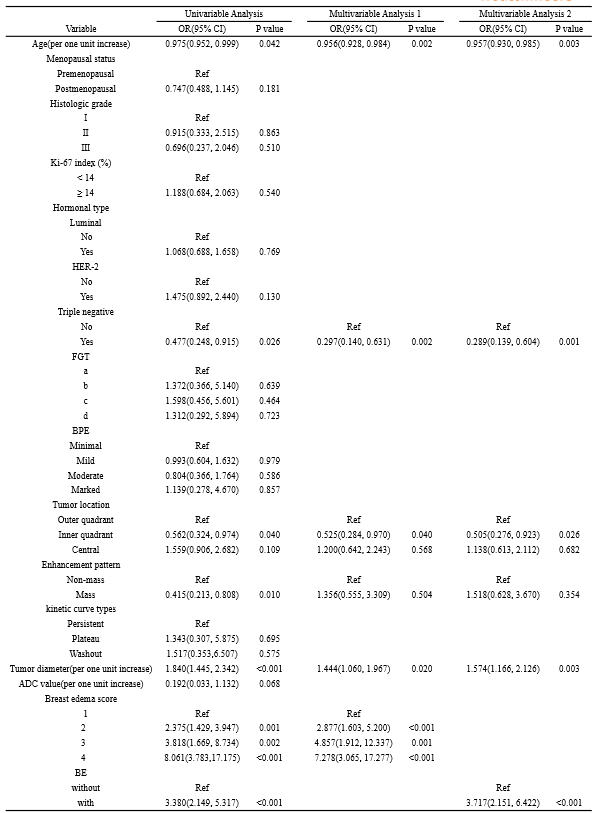
Table 2. Results of univariable and multivariable Logistic regression analysis for SLN metastasis.
Note.—HER2, human epidermal receptor 2; FGT, fibroglandular tissue; BPE, backgroundparenchymal enhancement; ADC, apparent diffusion coefficient; BE, breast edema; OR, odds ratio; CI, confidence interval; Ref, reference category (OR = 1.00).