0407
Early Prediction of Treatment Response in HER2-Positive Breast Cancer Using multiparametric MRI1Department of Radiology, Guangzhou First People's Hospital, Guangzhou, China, 2Philips Healthcare, Guangzhou, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Breast, Tumor, multiparametric MRI, neoadjuvant chemotherapy (NAC), HER2-positive breast cancer
Motivation: Imaging pre- and post- neoadjuvant chemotherapy (NAC) fails to adequately capture and quantify temporal heterogeneity and biological changes of tumors.
Goal(s): To assess if longitudinal changes in multiparametric MRI can predict early response to neoadjuvant chemotherapy (NAC) in HER2-positive breast cancer and to establish quantitative models based on these features.
Approach: Two predictive models were developed, one based on clinicopathologic features and another that combined clinicopathologic and MRI features.
Results: The combined model performs optimally in all datasets. Changes observed in multiparametric MRI can predict early treatment responses in HER2-positive BC and assist in tailoring personalized treatment plans.
Impact: The prediction model was simple and feasible, which was helpful for individualized treatment planning.
Introduction
Neoadjuvant chemotherapy (NAC) is the standard treatment for human epidermal growth factor receptor 2 (HER2)-positive breast cancer (BC) patients1, but some individuals do not respond well to this therapy, leading to adverse outcomes, such as early recurrence, metastasis, and even death2. The conventional measure for prognosis, pathological complete response (pCR) can only be determined after surgery, when significant treatment has already been administered. To address this issue, there is a need for a reliable early biomarker to guide treatment adaption based on response. However, there is a lack of systematic analysis of the change in functional MRI features in response to NAC in HER2-positive BC in the literature. Therefore, the aim of this study was to evaluate the potential of using multiparametric MRI to monitor changes in tumors during early NAC in HER2-positive BC and establish a model that incorporates functional MRI biomarkers for quantifying treatment efficacy.Methods
The study included patients with HER2-positive invasive breast cancer who underwent NAC and received MRI examinations both before NAC and after two cycles of NAC. The MRI images were analyzed by two radiologists using the American Society of Radiology BI-RADS MRI 2013 standard. Changes in the largest diameter (LD) of the tumor, represented as ΔLD (mm), were calculated using the formula ΔLD = LD2 - LD1, where LD1 and LD2 correspond to the LD before and after two cycles of NAC, respectively. Similarly, changes in apparent diffusion coefficient (ΔADC) and time-intensity curve (ΔTIC) were calculated. The predictive power of the different models was assessed using the area under the receiver operating characteristic curve (AUC). Additionally, decision curve analysis (DCA) was employed to evaluate the clinical utility of the model by quantifying net benefits.Results
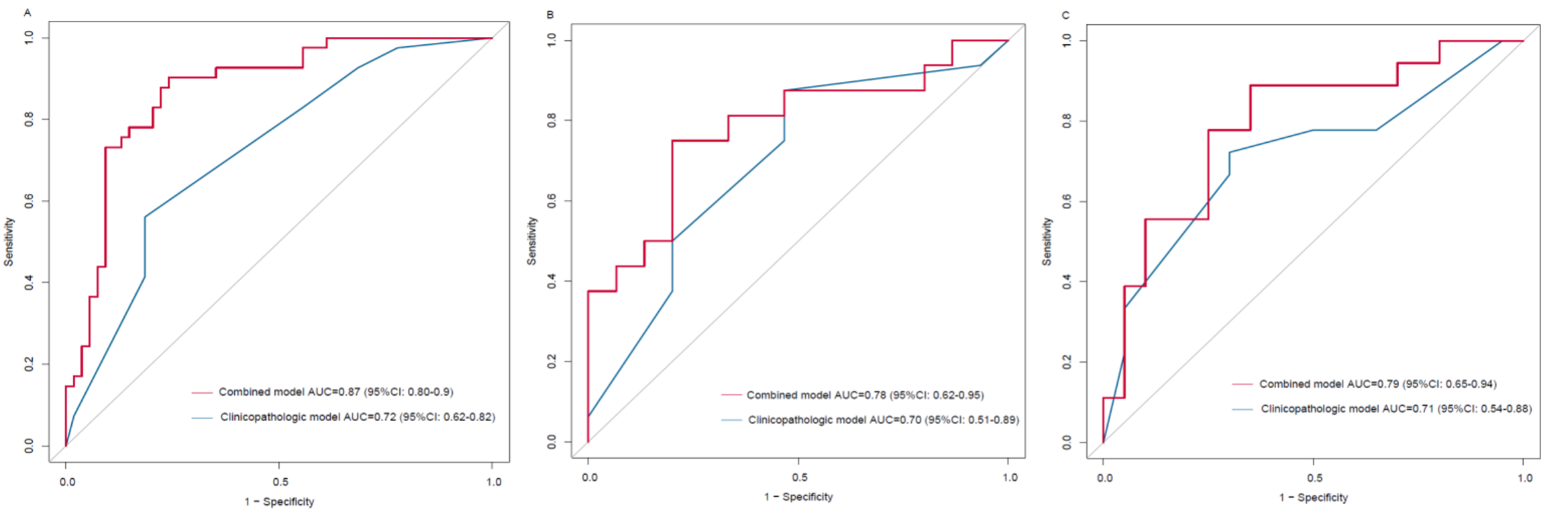
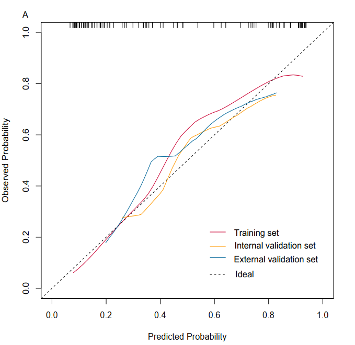
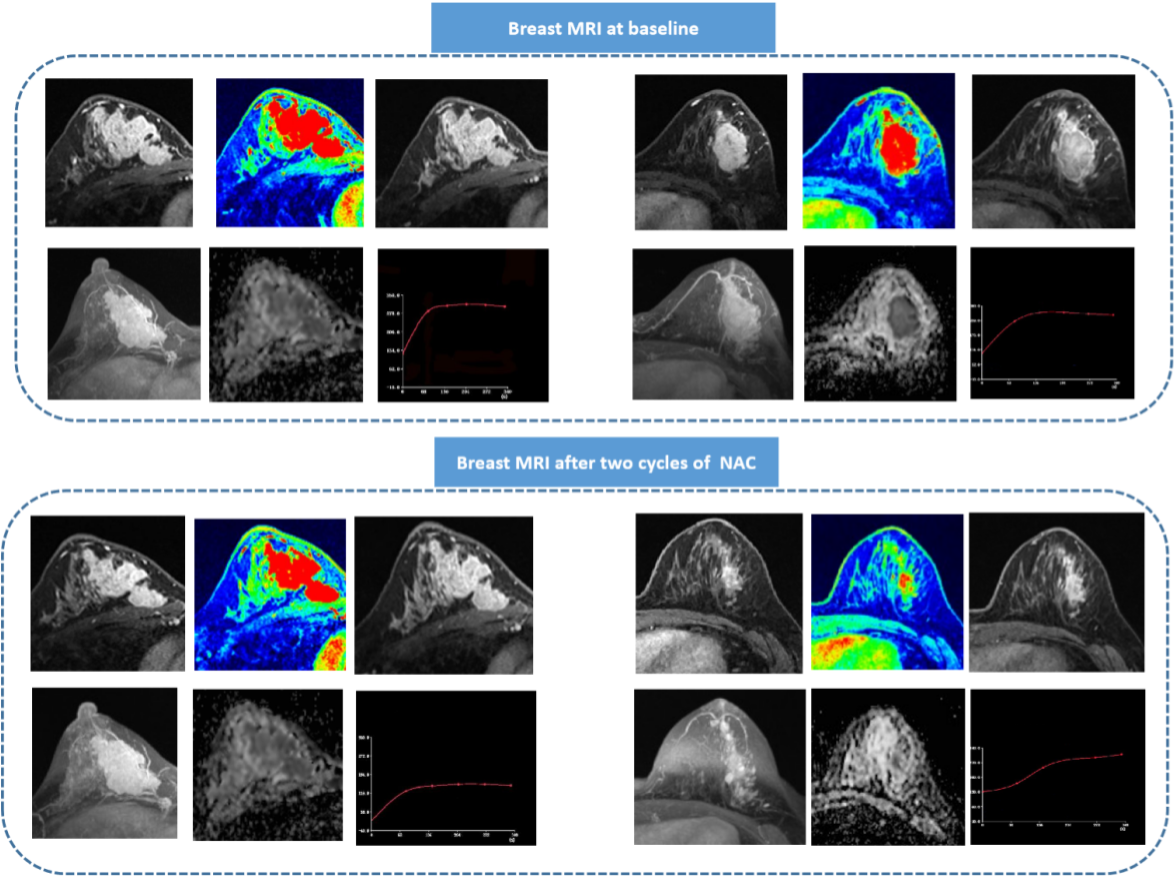
The clinicopathologic model was developed based on Ki-67 status and clinical T stage. In the training set, the model achieved an AUC of 0.72 (95% CI: 0.62-0.82). Similar AUC values of 0.70 (95% CI: 0.51-0.89), and 0.71 (95% CI: 0.36-0.73) were obtained for the internal and external validation sets, respectively.Compared to the clinicopathologic model, the combined model, which incorporated LD2, ΔADC, and ΔTIC, exhibited improved performance in both the training and validation datasets. The combined model achieved AUC values of 0.85 (95% CI: 0.80-0.95) in the training data set, 0.78 (95% CI: 0.62-0.95) in the internal validation set, and 0.79 (95% CI=0.65-0.94) in the external validation set (Figure 1). Calibration curves for the combined model indicated good consistency between the predicted probabilities of pCR by the model in all datasets (Figure 2). Typical MRI examples of the combined model are illustrated in Figure 3.
Discussion
Patients with HER2-positive BC represent a population that is often chosen for NAC with relatively high rates of pCR. However, it is critical to identify patients who do not respond to NAC early in their treatment in order to modify therapeutic strategies, reduce side effects, and improve pCR rates. While many prior investigations have assessed the use of MRI to detect pCR in BC patients receiving NAC, these studies typically had limited representation of HER2-positive cases. In contrast, our study includes a substantial cohort of 164 HER2-positive patients, specifically aiming to evaluate the effectiveness of multiparametric MRI in assessing NAC.One notable finding from our study is that pretreatment MRI features alone did not effectively predict pCR in HER2-positive BC. This observation aligns with similar results reported by Malhaire et al.3. However, the combined model, which integrated MRI features, showed higher diagnostic performance compared to the clinicopathologic model across all sets. The AUCs in our study ranged from 0.58 to 0.79, outperforming earlier studies that employed radiomics or DCE-MRI feature analysis to predict pCR to NAC in HER2-positive BC4, 5. The AUC of our combined model, based on multiparameter MRI, reached 0.87. Furthermore, the combined model also showed strong predictive capabilities across different subgroups. Validation in both the internal and external validation sets yielded AUCs of 0.79 and 0.78, respectively, indicating the model’s robust generalization and stability.
Conclusion
In conclusion, our results indicated that the combined model, utilizing multiparameter MRI, was highly effective in early prediction of pCR in HER2-positive BC. This model successfully identified HER2-positive BC patients who did not respond well to NAC at an early stage. The simplicity and feasibility of this prediction model make it a valuable tool for individualized treatment planning. To future establish the robustness of our model, future studies should include larger patient cohorts for validation.Acknowledgements
No acknowledgements found.References
1. Mieog JS, van der Hage JA, van de Velde CJ. Neoadjuvant chemotherapy for operable breast cancer. Br J Surg. 2007; 94(10):1189-200.
2. Rye IH, Trinh A, Saetersdal AB, et al. Intratumor heterogeneity defines treatment-resistant HER2+ breast tumors. Mol Oncol. 2018; 12(11):1838-55.
3. Malhaire C, Selhane F, Saint-Martin MJ, et al. Exploring the added value of pretherapeutic MR descriptors in predicting breast cancer pathologic complete response to neoadjuvant chemotherapy. Eur Radiol. 2023.
4. Heacock L, Lewin A, Ayoola A, et al. Dynamic Contrast-Enhanced MRI Evaluation of Pathologic Complete Response in Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Breast Cancer After HER2-Targeted Therapy. Acad Radiol. 2020; 27(5):e87-e93.
5. Liu Z, Li Z, Qu J, et al. Radiomics of Multiparametric MRI for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Chemotherapy in Breast Cancer: A Multicenter Study. Clin Cancer Res. 2019; 25(12):3538-47.
Figures