0396
Pretreatment arterial spin labelling combined with depth of invasion predict disease progression in nonmetastatic NPC after IMRT1Department of Diagnostic Radiology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, China, Beijing, China
Synopsis
Keywords: Head & Neck/ENT, Arterial spin labelling, Nasopharyngeal carcinoma; prognosis; depth of invasion
Motivation: Arterial spin labeling (ASL) showed the promising value in diagnosis and early treatment outcome prediction in head and neck. Whether ASL combined with tumor invasion depth could help predicting disease progression needs further investigate.
Goal(s): To explore the value of CBF derived from ASL and depth of invasion in predicting 3-year disease progression in NPC.
Approach: Prospective inclusion of consecutive patients with regular follow-up. Selection of appropriate statistical methods to construct and compare models.
Results: CBF and tumor invasion depth are significantly correlated with progression-free survival, and both of them could help predicting 3-year disease progression.
Impact: ASL and tumor infiltration depth shown for the first time to predict disease progression in NPC, which could help with clinical treatment decisions.
Introduction
Nasopharyngeal carcinoma (NPC) is an aggressive head and neck cancer and approximately 80% of patients are diagnosed with advanced stage at initial diagnosis. After standard treatment, about 10-30% of patients would suffer disease progression. Although TNM stage is widely used in clinic, large variations in outcome are found in patients under similar treatment1. Based on fast spin-echo sequence, arterial spin labeling (ASL) has high signal-to-noise rate and spatial resolution, which is recommended for clinical applications. The predictive value of cerebral blood flow (CBF) in early treatment response (residual or non-residual) has been demonstrated in previous studies2. However, residual tumor tissue is difficult to distinguish from post-treatment changes at relatively short follow-up times. NPC with high T stage have poor prognosis than those with low T stage, and we hypothesised that depth of invasion (DOI) is a neglected quantitative prognostic indicator. Therefore, the aim of this study is to investigate the value of ASL and DOI in predicting disease progression in NPC.Methods
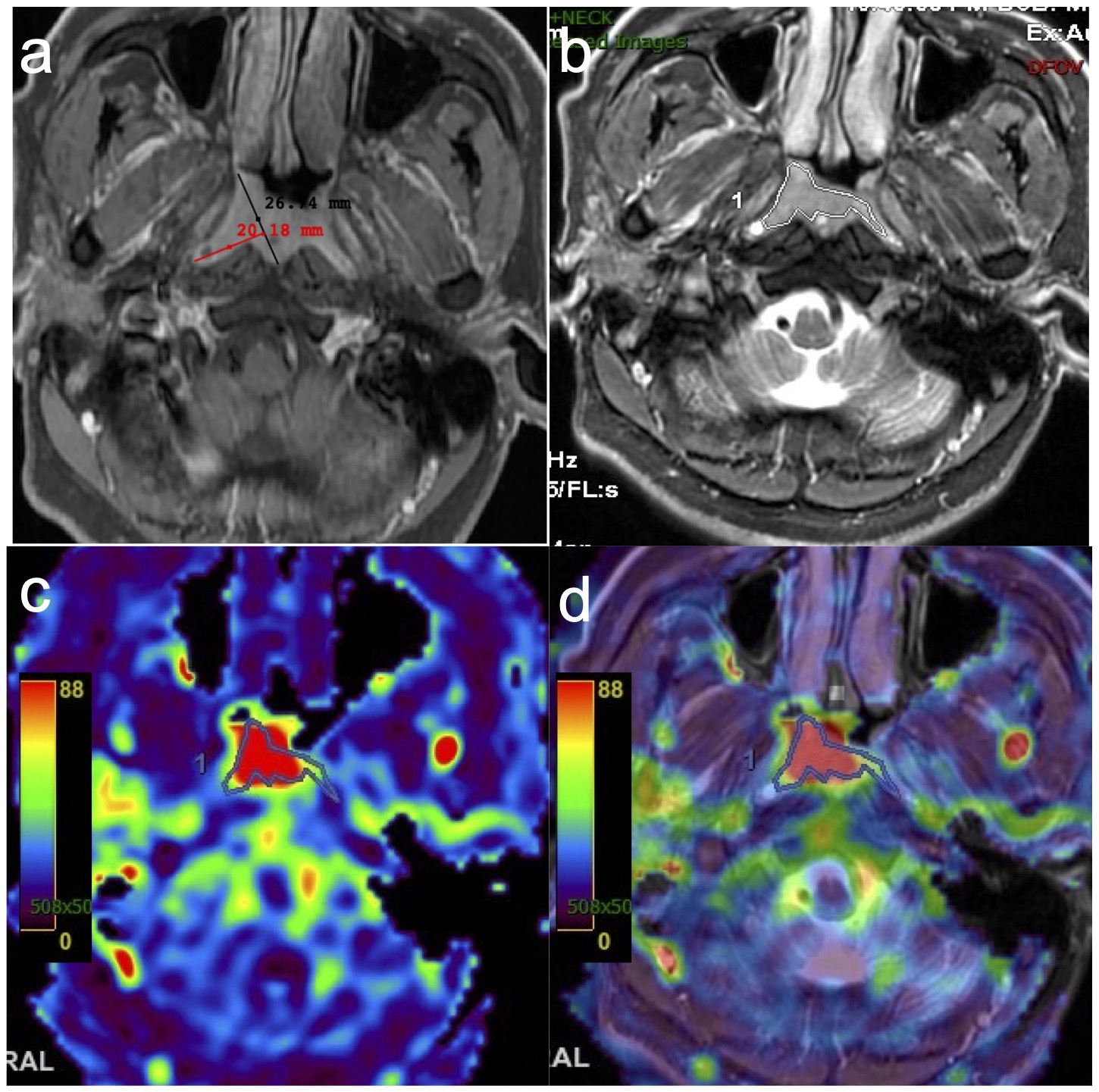
This study prospectively included 53 NPC patients who underwent conventional MRI and ASL scans from August 2018 to May 2019. Data progressing: The parameters of pseudo-continuous ASL sequence were as follows: FOV = 24cm, matrix = 288 × 192, thickness/slice gap = 3mm/0mm, ETL = 21, number of slice = 36, PLD = 1025ms, TR/TA/TE = 4326ms/262s/11.1ms, NEX = 3, band-width = 41.67. After that, an axial FRFSE T2WI sequence was performed with a uniform scan range as that of ASL (thickness/slice gap of 3/0 mm) to be fully matched with ASL. Two radiologists manually delineated the largest slice of tumor on vendor-supplied Advantage Workstation (ADW 4.7 version, GE, US), with reference to conventional MRI. A reference line connecting the front of lateral nasopharyngeal wall (or the front of tumor when it not extent beyond lateral nasopharyngeal wall) and the center of posterior nasopharyngeal wall (between bilateral longus capitis muscle). The length of inward invasion of the tumor perpendicular to the reference line was defined as DOI (Fig.1). Two radiologists independently measured DOI on contrast-enhanced T1WI3. The average value (CBF and DOI) of two radiologists was further evaluated.Treatment and follow-up: All patients underwent standard treatment and regular follow-up (every 3–4 months for the first 3 years, every 6 months during 4–5 years, then yearly). Imaging examination (CT, MRI, US, PET-CT and bone scan) and/or biopsy was routinely used. Progression-free survival (PFS) was defined as the time from the start of treatment to the date of disease progression (local-regional or distant), death, or last follow-up, whichever occurred first. The last follow-up set for July 30, 2022. Patients with disease progression within three years of treatment were categorized in the disease progression group.
Statistical analysis: A two-tailed P < 0.05 indicated statistical significance. The independent sample-t test or Mann–Whitney U test was used to compare the difference between patients with and without progression. Univariate Cox proportional hazards regression analysis was performed to assess the correlation of CBF and DOI with PFS. The survival rate was calculated by using Kaplan–Meier analysis and differences were compared using log-rank test. To explore its value in the prediction of 3-year disease progression, univariate and multivariate logistic analysis were used to construct model. The nomogram and calibration curve were constructed, and the ROC and AUC was used. The Delong-test was used to compare the model performance.
Results
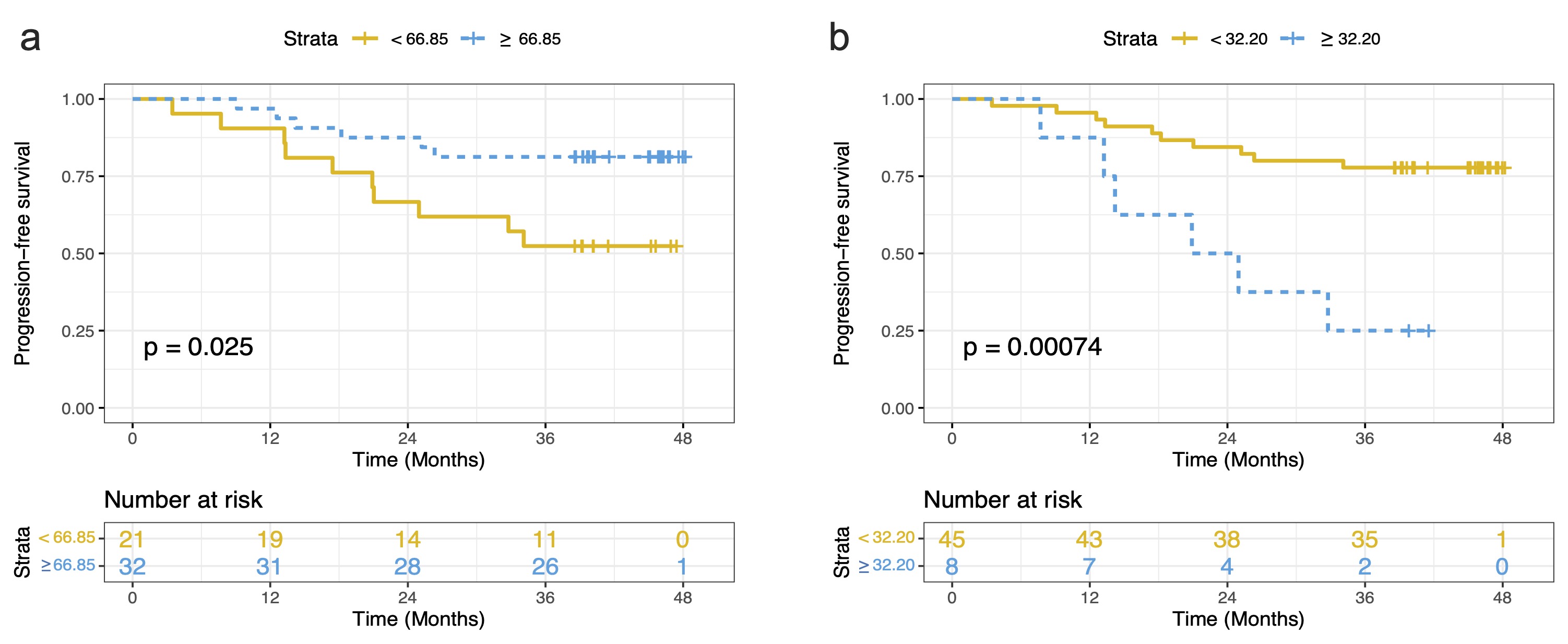
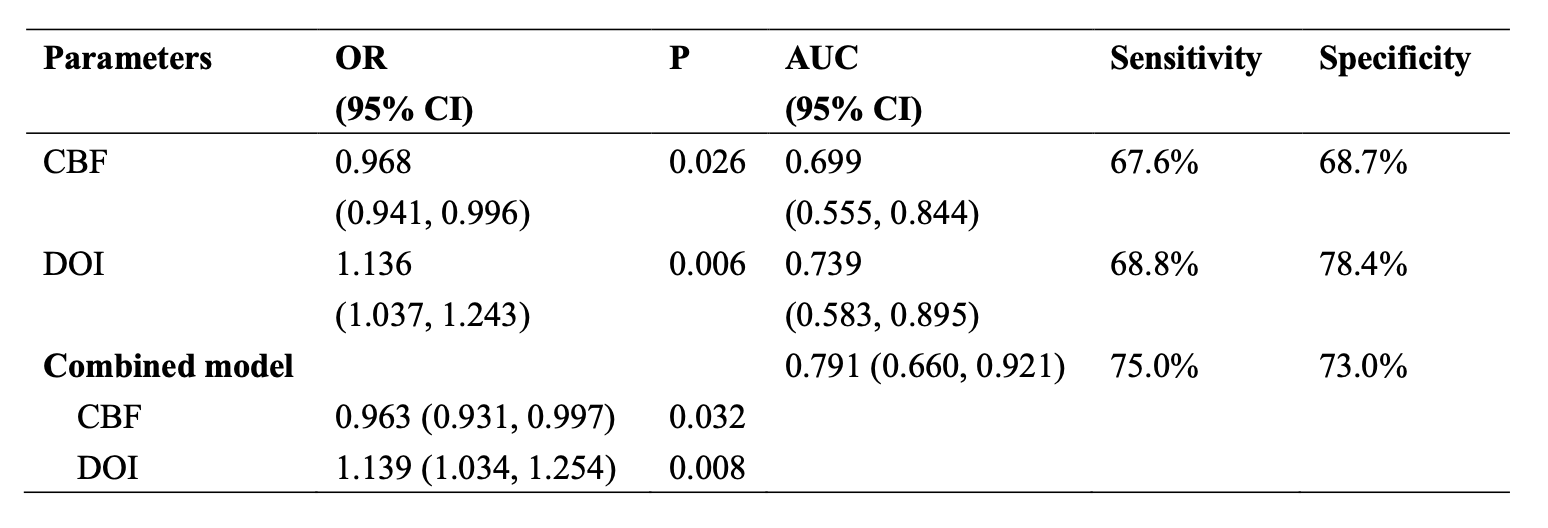
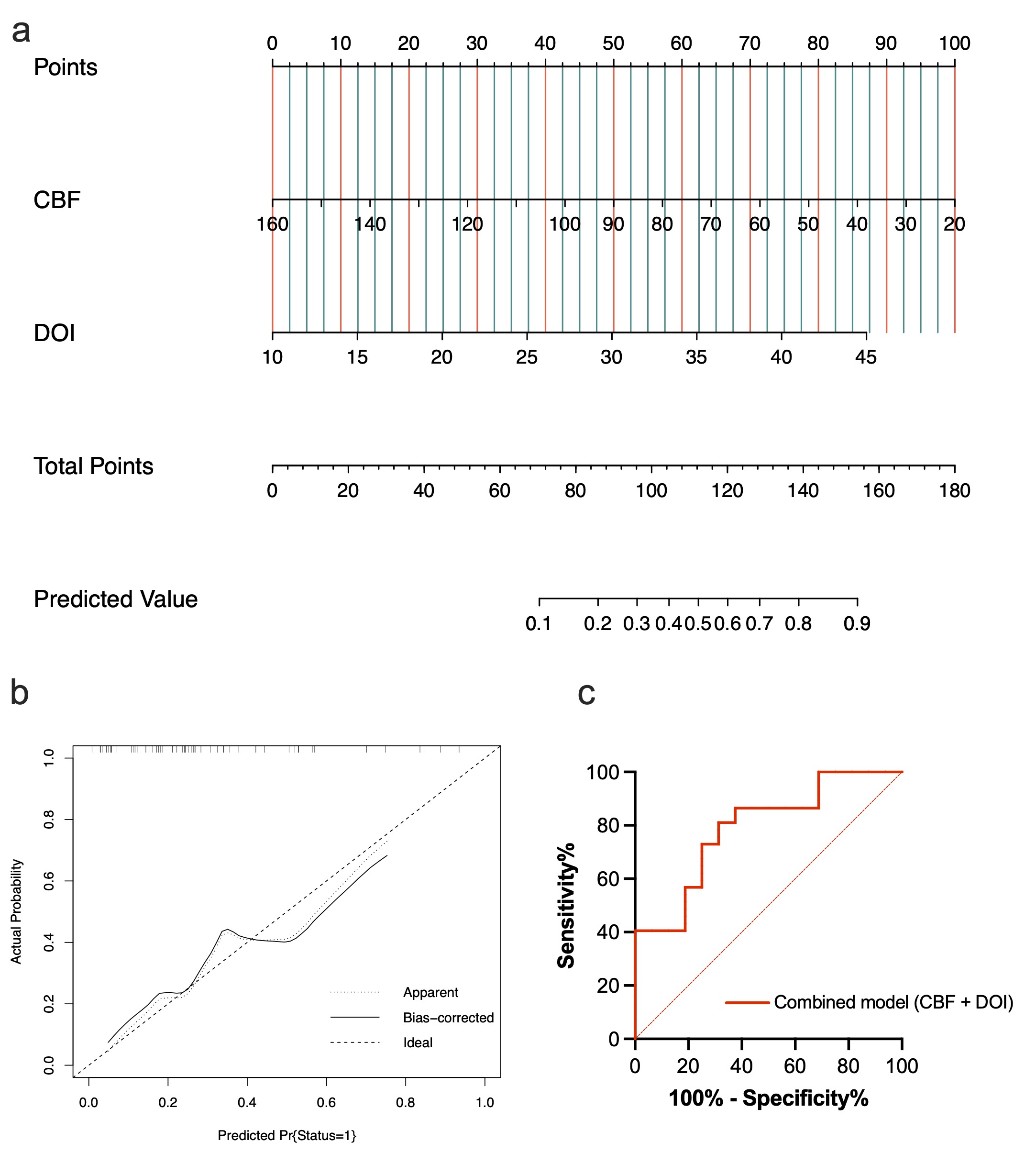
The median follow-up duration for all patients was 39.6 (3.5, 48.2) months and 16/53 (30.2%) patients were categorized in 3-year disease progression group. CBF and DOI were significantly correlated with PFS (Fig.2). Patients without disease progression have higher CBF and lower DOI than others. CBF and DOI were selected to construct combined model (Fig.3) after multivariate analysis. The AUC of combined model was 0.791 (95%CI: 0.660, 0.921), which is higher than CBF and DOI. The nomogram and calibration curves are shown in Fig.4.Discussion
To our knowledge, this is the first study to explore the value of CBF and DOI in predicting disease progression in head and neck region. Tumors with higher CBF have richer blood supply and abundant neovascularity than those with lower CBF, which are sensitive to chemotherapy or chemoradiotherapy. Moreover, the DOI of tumors could also offer prognostic information for the deeply infiltrated part of tumors may be partitioned into insufficient radiation dose, with possible recurrence at follow-up. In order to eliminate individual differences, we used the reference line. However, a large and multi-center research is needed to validate our results.Conclusion
Pretreatment CBF derived from ASL and DOI could help predicting 3-year disease progression in NPC.Acknowledgements
No acknowledgement found.References
1, Zhang L, Huang Y, Hong S, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet 2016;388(10054):1883-1892.
2, Sun Z, Hu S, Xue Q, et al. Can 3D pseudo-continuous arterial spin labeling perfusion imaging be applied to predict early response to chemoradiotherapy in patients with advanced nasopharyngeal carcinoma? Radiother Oncol 2021;160:97-106.
3, Baba A, Masuda K, Hashimoto K, et al. Correlation between the magnetic resonance imaging features of squamous cell carcinoma of the buccal mucosa and pathologic depth of invasion. Oral Surg Oral Med Oral Pathol Oral Radiol 2021;131(5):582-590.
Figures