0395
Motion resolved rapid 3D multiparametric brain mapping with self-navigation1Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States, 2Department of Radiology, Harvard Medical School, Boston, MA, United States, 3Department of Radiology, Juntendo University, Tokyo, Japan, 4Department of Radiology, The University of Tokyo, Tokyo, Japan, 5Key Laboratory for Biomedical Engineering of Ministry of Education, Department of Biomedical Engineering, College of Biomedical Engineering & Instrument Science, Zhejiang University, Zhejiang, China, 6Fetal-Neonatal Neuroimaging & Developmental Science Center, Boston Children’s Hospital, Boston, MA, United States, 7Harvard/MIT Health Sciences and Technology, Massachusetts Institute of Technology, Cambridge, MA, United States
Synopsis
Keywords: Quantitative Imaging, Neuro
Motivation: While 3D multiparametric mapping acquisitions can provide rich and quantitative information, their long acquisition time renders them susceptible to motion.
Goal(s): To develop a rapid, multiparametric technique for motion-robust brain mapping.
Approach: 3D-QALAS acquisition with Cartesian variable-density sampling was implemented to achieve self-navigation while maintaining high scan efficiency. Brain position was estimated for each TR and incorporated in the reconstruction’s forward model.
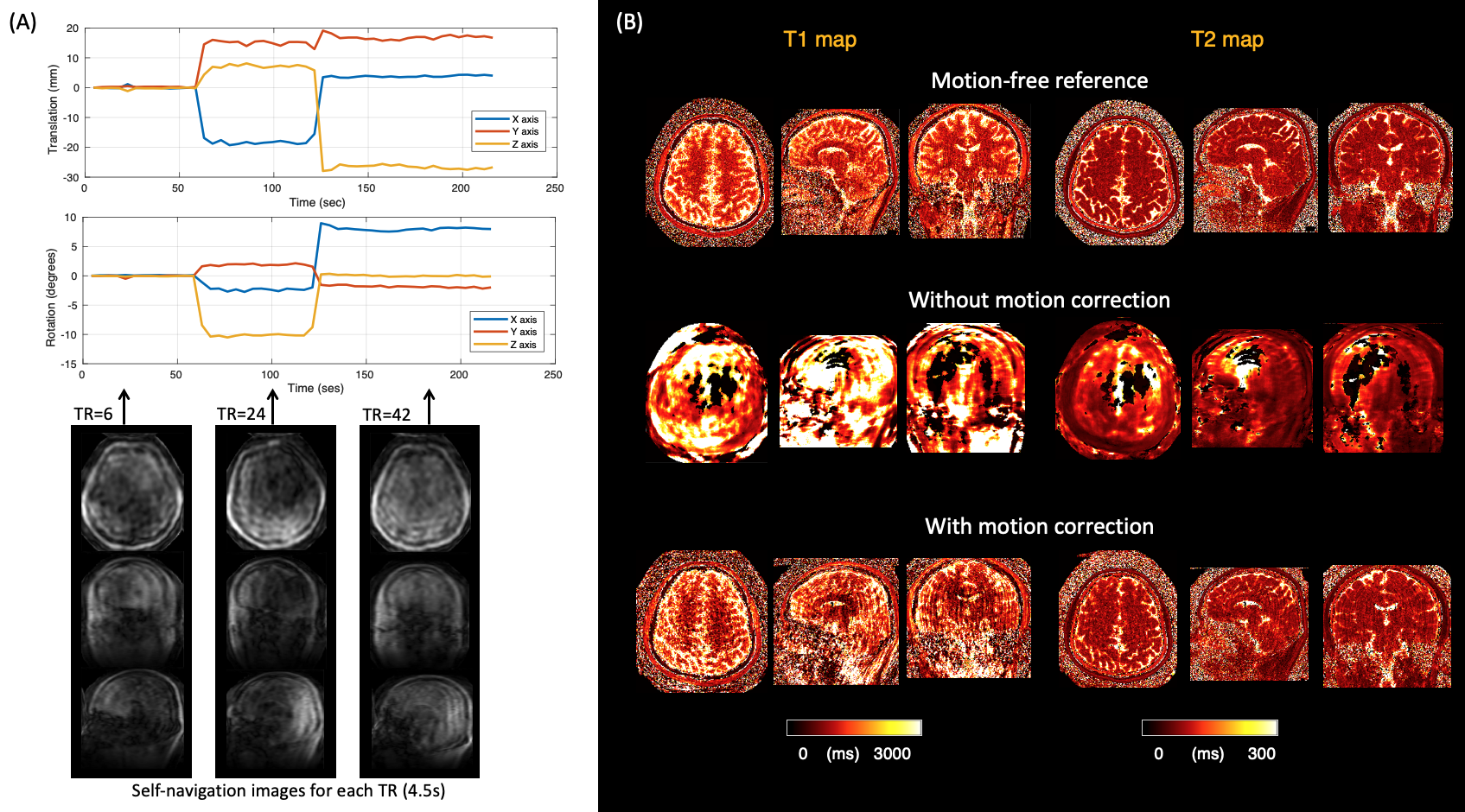
Results: The proposed method enabled reconstruction of motion-resolved datasets at a time resolution of 4.5s with tracking accuracy of <0.2 degrees and <0.5mm, providing T1 and T2 maps with significantly reduced artifacts and improved agreement with measurements from motion-free scans.
Impact: We propose an efficient, whole-brain quantitative scan at 1mm3 resolution in 3:36min and incorporate self-navigated motion-correction, thereby obviating the need for navigators or external hardware. This benefits clinical translation especially for imaging unsedated children in clinical and research settings.
Introduction
Motion presents a significant challenge in MRI exams, as it can lead to artifacts and image degradation1. This issue is particularly acute for 3D multiparametric mapping techniques that typically require long scan times. While several techniques to address this have been demonstrated2–6, they typically necessitate additional hardware or modifications to the sequence, such as extra scans and/or navigators.In this context, we propose a motion-resolved rapid 3D multiparametric brain mapping technique using Cartesian variable-density sampling7, 8. Our technique does not require additional scans, navigators, or external hardware. With the time-efficient acquisition, whole-brain T1 and T2 maps with 1mm isotropic resolution was acquired in ~3.5 minutes.
Methods
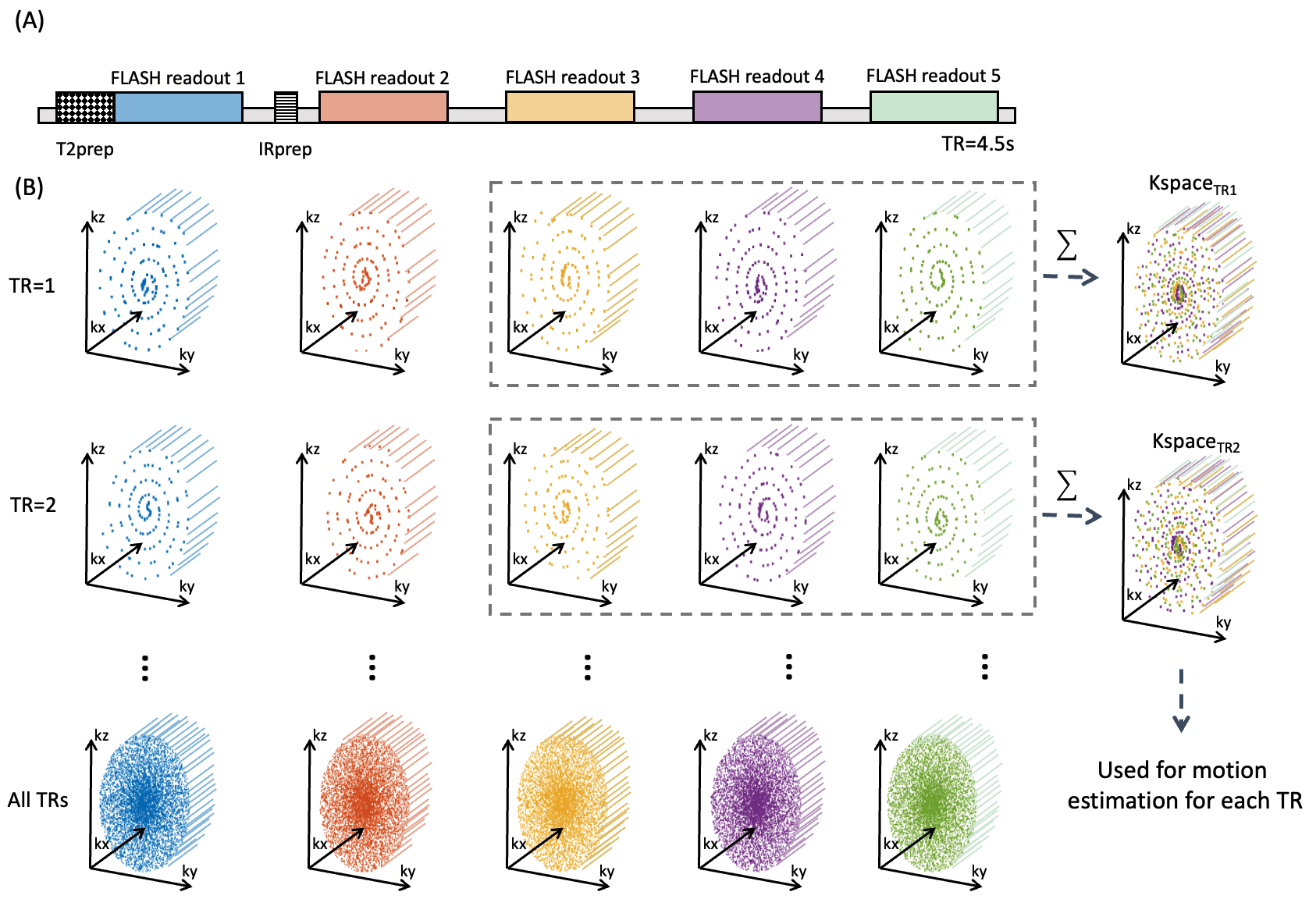
Sequence designThe proposed acquisition scheme is illustrated in Figure 1. The acquisition is based on 3D-quantification using an interleaved Look–Locker acquisition sequence with a T2 preparation pulse (3D-QALAS)9, 10, as shown in the upper part of Figure 1. Acquisition was based on 3D Cartesian sampling with spiral-like variable-density sampling7, 8. The sampling strategy involves center-out sampling with each spoke acquired according to the golden-ratio angle. This ensures each FLASH readout to sample different k-space lines within each TR. To capture low-frequency information, low-frequency points are sampled multiple times. This trajectory strategy provides incoherent sampling artifacts for the different motion-resolved images. For each TR, k space data of the last 3 FLASH readouts are used for motion estimation. This is because the latter 3 readouts have similar (T1-weighted) contrasts. Sequence was implemented in Pulseq (v1.4.0) and executed with interpreter11.
Motion estimation and Reconstruction
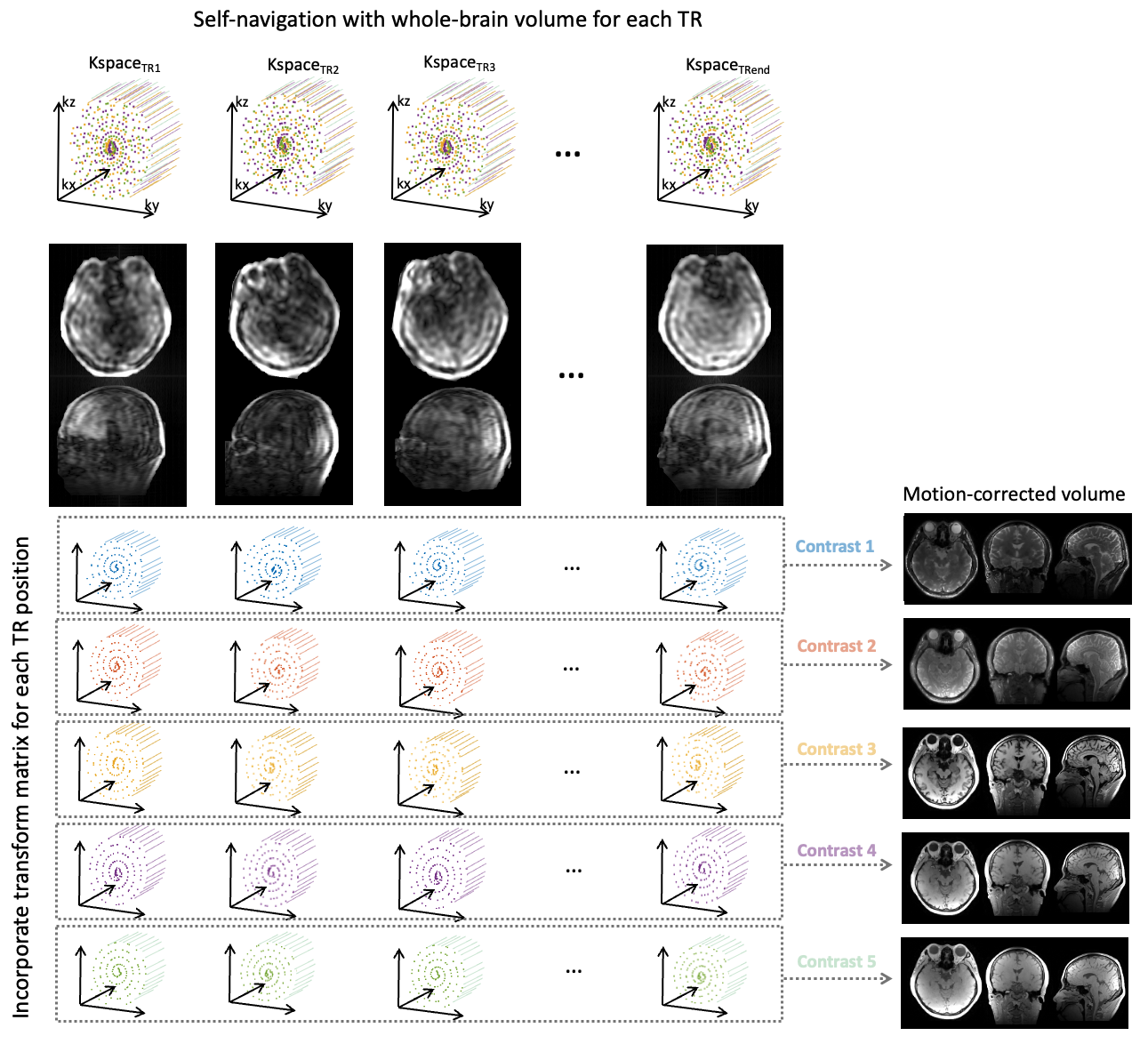
The proposed pipeline of motion estimation and reconstruction framework is shown in Figure 2. K-space data from each TR is reconstructed with SENSE12. These time-resolved data are used for estimating rigid 3D head motion by calculating the transformation for each volume to the reference state. This transformation $$$T$$$ is incorporated to the following forward model: $$x=\arg\min\sum_{t}^{}\left\|FCT_{t}x-k_{t} \right\|^{2}_{2}+\lambda\cdot{TV(x)}$$
Here, $$$x$$$ represents the image to be reconstructed, $$$t$$$ represents the time point, $$$k_{t}$$$ represents the acquired multicoil k-space at time point $$$t$$$, $$$T_{t}$$$ represents the transformation matrix of the 3D head position at time point $$$t$$$ relative to reference position, $$$F$$$ represents the Fourier transformation operator, $$$C$$$ represents the coil-sensitivity profiles, and $$$TV$$$ is the temporal total-variation operator, with regularization parameter $$$𝜆$$$.
Parameter map estimation
The reconstructed five source images were passed to voxel-wise Bloch simulations with B1 correction and inversion efficiency estimation, and the T1 and T2 values were obtained for each voxel.
Experiments
All data was acquired on a 3T MRI system (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany) with 32-channel receiver coil in NIST/ISMRM phantom and a healthy volunteer in sagittal orientation with 1mm iso tropic resolution with the following parameters: FOV,224x224x192; matrix, 224x224x192; TR, 4500ms; TE, 2.29ms; TI, 110/1010/1910/2810/3710ms; echo spacing, 5.8 ms; flip angle, 4 degrees; echo train length, 127; spiral segments, 58; acceleration, R≈7; bandwidth, 372 Hz/px, acquisition time, 3min36s. A reference scan was used to estimate sensitivity coil maps with ESPIRiT after coil-compression to 20 virtual coils13.
Phantom test: To evaluate the effect of motion correction on quantitative mapping, NIST/ISMRM phantom was scanned in two different positions (approximately 5 degrees rotated) without motion. To evaluate the effect of motion correction on the quantitative values, k-spaces of different positions were retrospectively concatenated to create a synthetic motion-corrupted data.
In vivo test: A healthy volunteer was instructed to move head positions when the MRI operator announced to approximate a clinical motion-corrupted data.
Evaluation
Circular ROI was placed for each sphere of the NIST/ISMRM phantom. Bias was evaluated using motion-free data without any motion correction as reference.
Results
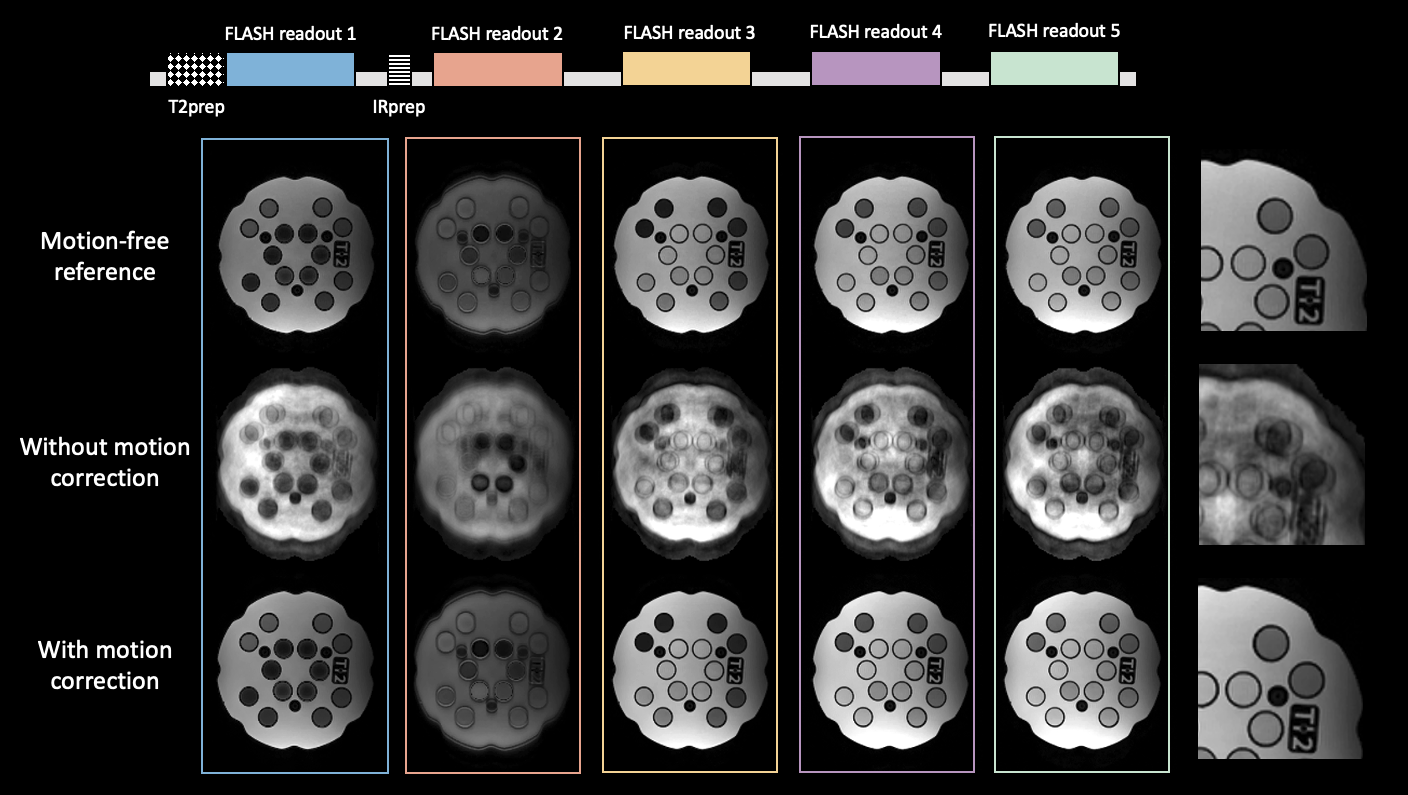
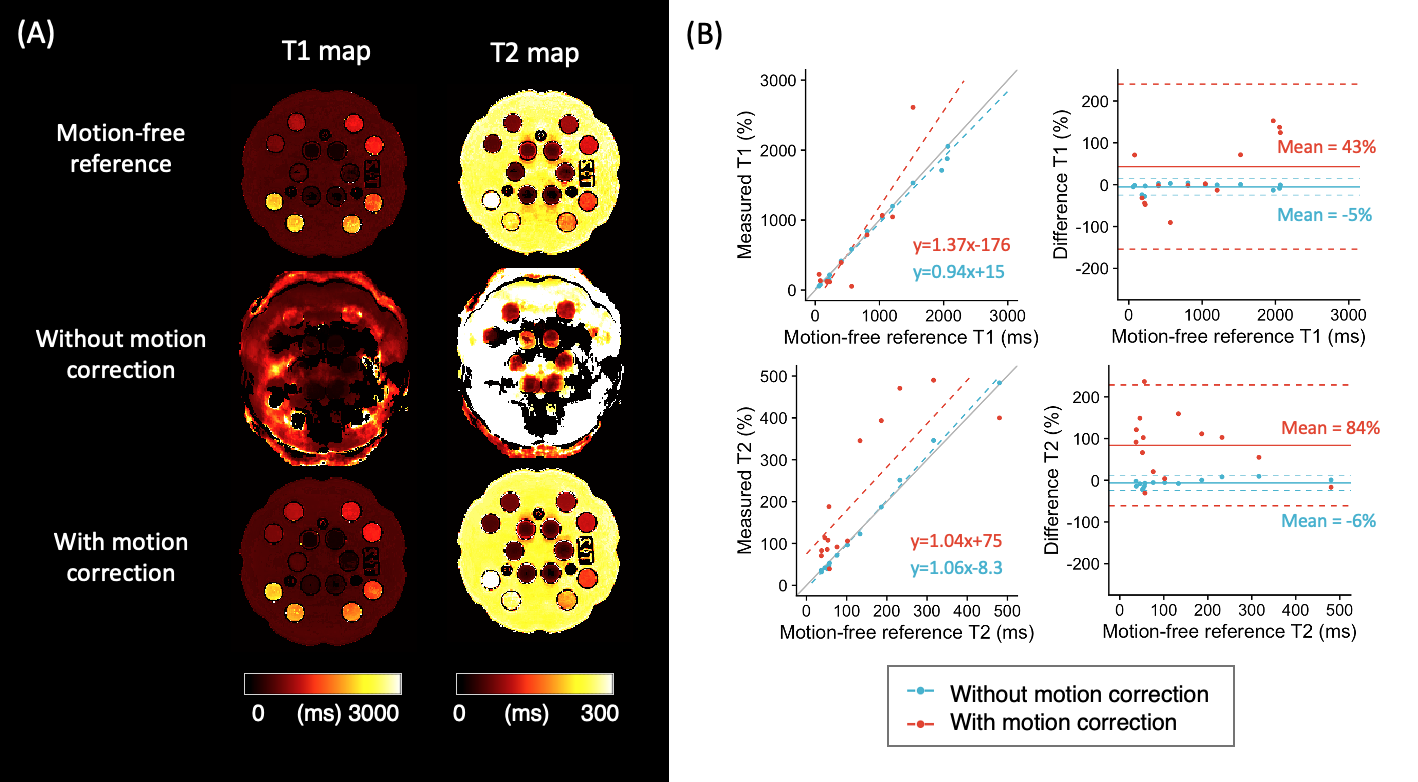
Figure 3 shows the NIST/ISMRM phantom results obtained with and without the motion correction. Each contrast of motion corrected reconstruction are visually similar to reference motion-free acquisition. The T1 and T2 values measured from the motion-corrected scans were closer to the reference values obtained from the motion-free scans (i.e., higher accuracy) and less standard deviation of difference between reference (i.e., higher precision) (Figure 4). Figure 5 shows in vivo results. The standard deviation of the rotation and translation of a subject keeping still was 0.17 degree and 0.48 mm, indicating a tracking accuracy <0.2 degree and <0.5 mm.Discussion and Conclusion
We developed a motion-robust 3D multiparametric mapping approach based on self-navigation to improve motion robustness without prolonging the scan time. This study demonstrated that the image quality and accuracy of quantitative maps were improved with a self-navigation reconstruction pipeline.Acknowledgements
This work was supported by research grants NIH R01 EB028797, U01 EB025162, P41 EB030006, U01 EB026996, R03 EB031175, R01 EB032378, UG3 EB034875, and NVidia Corporation for computing support.References
- Zaitsev M, Akin B, LeVan P, Knowles BR: Prospective motion correction in functional MRI. Neuroimage 2017; 154:33–42.
- Kecskemeti S, Alexander AL: Three-dimensional motion-corrected T1 relaxometry with MPnRAGE. Magn Reson Med 2020; 84:2400–2411.
- Cruz G, Jaubert O, Schneider T, Botnar RM, Prieto C: Rigid motion-corrected magnetic resonance fingerprinting. Magn Reson Med 2019; 81:947–961.
- Callaghan MF, Josephs O, Herbst M, Zaitsev M, Todd N, Weiskopf N: An evaluation of prospective motion correction (PMC) for high resolution quantitative MRI. Front Neurosci 2015; 9:97.
- Fujita S, Hagiwara A, Takei N, et al.: Rigid real-time prospective motion-corrected three-dimensional multiparametric mapping of the human brain. Neuroimage 2022; 255:119176.
- Hu S, Chen Y, Zong X, Lin W, Griswold M, Ma D: Improving motion robustness of 3D MR fingerprinting with a fat navigator. Magn Reson Med 2023; 90:1802–1817.
- Cheng JY, Zhang T, Ruangwattanapaisarn N, et al.: Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging 2015; 42:407–420.
- Prieto C, Doneva M, Usman M, et al.: Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging 2015; 41:738–746.
- Fujita S, Hagiwara A, Hori M, et al.: Three-dimensional high-resolution simultaneous quantitative mapping of the whole brain with 3D-QALAS: An accuracy and repeatability study. Magn Reson Imaging 2019; 63:235–243.
- Kvernby S, Warntjes M, Carlhäll C-J, Engvall J, Ebbers T: 3D-Quantification using an interleaved Look-Locker acquisition sequence with T2-prep pulse (3D-QALAS). J Cardiovasc Magn Reson 2014; 16:O82.
- Layton KJ, Kroboth S, Jia F, et al.: Pulseq: A rapid and hardware-independent pulse sequence prototyping framework. Magn Reson Med 2017; 77:1544–1552.
- Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P: SENSE: sensitivity encoding for fast MRI. Magn Reson Med 1999; 42:952–962.
- Uecker M, Lai P, Murphy MJ, et al.: ESPIRiT--an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med 2014; 71:990–1001.
Figures