0390
Versatile motion-corrected brain MRI leveraging ERIC-PT: Efficient, Robust and Instruction-free Calibrated Pilot Tone1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3London Collaborative Ultra high field System (LoCUS), London, United Kingdom, 4Biomedical Image Technologies, Universidad Politécnica de Madrid and CIBER-BNN, ISCIII, Madrid, Spain, 5Siemens Healthcare Limited, London, United Kingdom, 6Siemens Healthcare Limited, Frimley, United Kingdom, 7Guys and St Thomas’ NHS Foundation Trust, King's College London, London, United Kingdom
Synopsis
Keywords: Motion Correction, Motion Correction, Pilot Tone
Motivation: Robust motion correction relies on sequence modifications, either adding navigators or re-ordering the k-space sampling. These modifications might not be possible for every sequence.
Goal(s): To leverage motion-sensitive Pilot Tone (PT) signals to guide motion correction for any standard 3D acquisition.
Approach: We propose the ERIC calibration protocol, which distributes short self-navigated (DISORDER) acquisitions across the whole examination. Combined with data-driven motion correction reconstructions, we can achieve robust PT calibration.
Results: We show the potential to correct standard MPRAGE acquisitions with a linear phase encoding scheme in 4 healthy volunteers (HV) even when using 54 seconds worth of calibration data.
Impact: Correcting motion in any 3D acquisition is an unsolved problem. Combining pre-calibrated PT signals with data-driven optimizations explores a promising avenue. To this end, building a robust calibration model by acquiring ~1min worth of data would easily integrate into examinations.
Introduction
Motion causes artifacts in brain MRI, which can be corrected when motion is known1. Tracking devices obtain independent measures of motion but require dedicated equipment/calibration2-5. Data-driven approaches directly estimate motion from acquired k-space but require sequence modifications6-7. We combine both approaches by leveraging Pilot Tone (PT) as an external motion sensor natively encoded within k-space8-10. We propose ERIC, an Efficient, Robust and Instruction-free Calibration to build a PT motion model. ERIC combines data-driven motion estimation with self-navigated calibration acquisitions that make no demands on the patient. We show the potential to correct standard MPRAGE in 4 healthy volunteers (HV).Methods
Pilot Tone (PT):PT is RF signal injected into the scanner room and detected by every receiver coil without overlapping the MR signal8-10. Received PT signals, $$$\textbf{p}$$$, are acquired each readout and are sensitive to head motion11.
(PT-)alignedSENSE:
alignedSENSE12 uses data-driven optimization to jointly estimate motion states, $$$\textbf{z}$$$, and a motion-corrected image volume ($$$\textbf{x}$$$) from multi-coil data $$$\textbf{y}$$$ by dividing readouts into temporal groups (shots); $$$\textbf{y}_n$$$ for shot $$$n$$$ where each shot is assigned a different $$$\textbf{z}_n$$$:$$(\hat{\mathbf{x}},\hat{\mathbf{z}}_n)=argmin_{\textbf{x},\textbf{z}_n }\sum_{n}{||\textbf{A}_n\textbf{F}\textbf{ST}(\textbf{z}_n))\textbf{x}-\textbf{y}_n||^2_2}\ \ \ \ \ \ \ \ \ \ \ \ (1)$$where $$$\textbf{T}(\textbf{z}_n),\textbf{S},\textbf{F}$$$ and $$$\textbf{A}_n$$$ respectively represent rigid motion, coil sensitivities, Fourier operator and sampling structure. Although Eq.1 can be used for any sequence, robust performance requires the use of self-navigated sampling schemes like DISORDER6, in which each shot collects samples spanning across the full k-space.
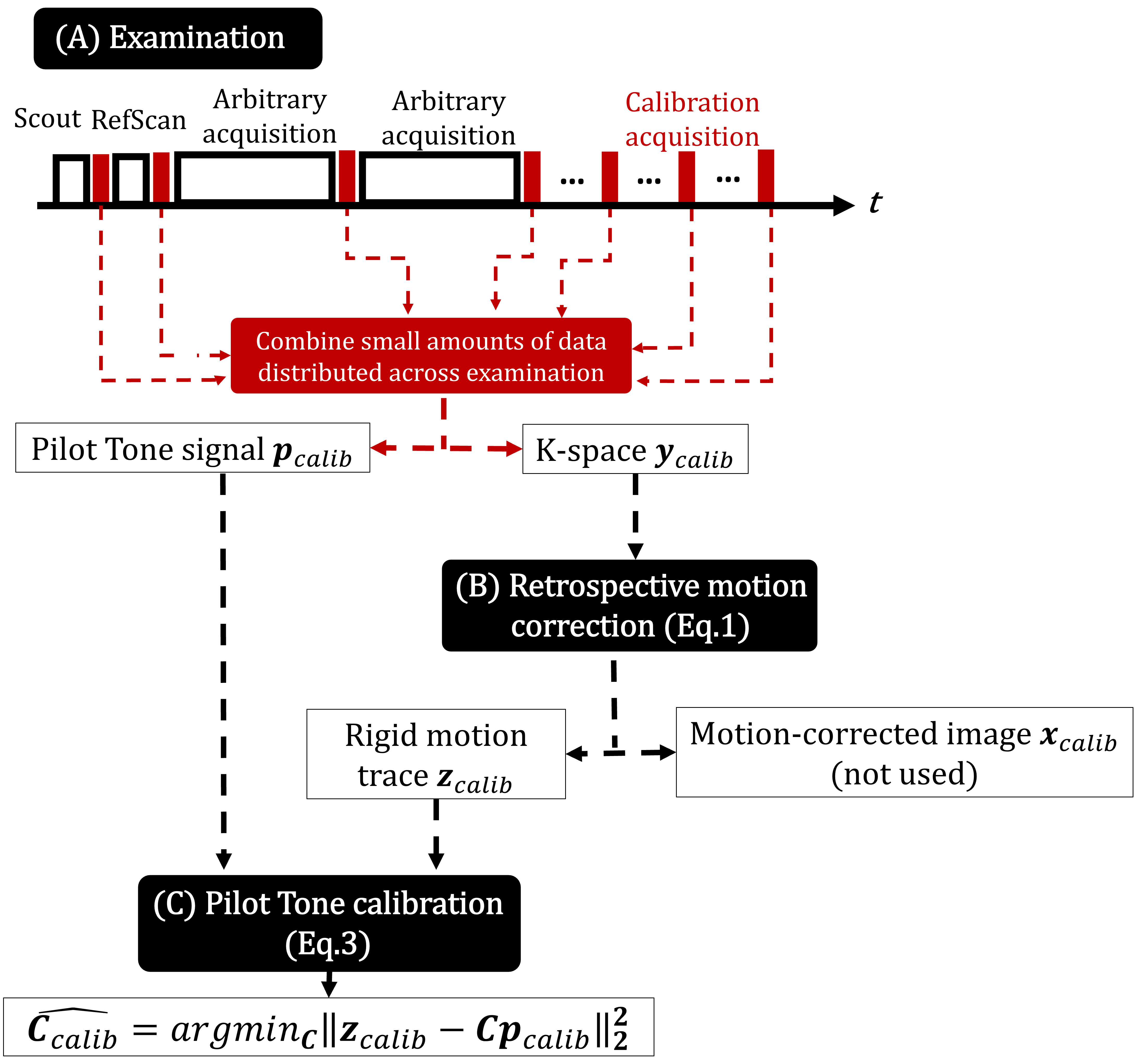
We extend our previous work combining PT with alignedSENSE (PT-alignedSENSE)13 to motion-correct any 3D acquisition. Using a linear motion model11, $$$\textbf{z}_n=\textbf{C}\textbf{p}_n$$$ where $$$\textbf{C}$$$ is a calibration matrix, we can optimize for $$$\textbf{C}$$$ and $$$\textbf{x}$$$ to maximize data consistency between PT and k-space data:$$(\hat{\mathbf{x}},\hat{\mathbf{C}})=argmin_{\textbf{x},\textbf{C}}\sum_{n}{||\textbf{A}_n\textbf{F}\textbf{ST}(\textbf{C}\textbf{p}_n)\textbf{x}-\textbf{y}_n||^2_2}\ \ \ \ \ \ \ \ \ \ \ \ (2)$$To be effective with linear sampling schemes, Eq.2 benefits from a pre-calibrated $$$\textbf{C}$$$, $$$\textbf{C}_{calib}$$$, which can be estimated given a set of known poses $$$\textbf{z}_{calib}$$$:$$\hat{\mathbf{C}}_{calib}=argmin_{{\mathbf{C}}}||\textbf{z}_{calib} - \textbf{C}\textbf{p}_{calib}||^2_2\ \ \ \ \ \ \ \ \ \ \ \ (3)$$ERIC calibration protocol:
$$$\textbf{z}_{calib}$$$ is usually obtained using a quick pre-scan whilst acquiring $$$\textbf{p}_{calib}$$$14,15 at the start of the examination during which deliberate patient movement is required to obtain enough variation in motion parameters to fit $$$\hat{\mathbf{C}}_{calib}$$$. Instead, we propose to distribute self-navigated calibration acquisitions throughout the examination. DISORDER is ideal for this purpose as its shot-based structure allows flexible interspersed layout in time, either during allocated time slots or sequence dead time. This is the ERIC protocol (Fig1), which can be integrated into standard examinations, but also benefits from the natural tendency of compliant subjects to slightly move as examinations progress.
Experiments
In-vivo data acquisition:We scanned 4 HVs at 7T (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany). For each HV, we acquired 6 calibration GREs across the examination (3x3x3mm3,TE/TR=1.93/3.8ms,FA=8°,FOV=240×212×240mm3,$$$\,$$$acceleration$$$\,$$$R=1x1,$$$\,$$$acquisition$$$\,$$$ time$$$\,$$$TA=27sec,$$$\,$$$TAshot=0.33sec) and 3 fully-sampled MPRAGEs (1x1x1mm3,$$$\,$$$TE/TRshort/TRlong=1.48/2.96/3000ms,$$$\,$$$inversion$$$\,$$$time$$$\,$$$TI=1400ms,FA=8°,FOV=240×210×256mm3,$$$\,$$$R=1x1,TA=10min35sec). The first MPRAGE was acquired with DISORDER sampling, yielding ground truth (GT) image and motion after alignedSENSE correction. Other MPRAGE acquisitions used a linear sampling scheme.
Calibration validation:
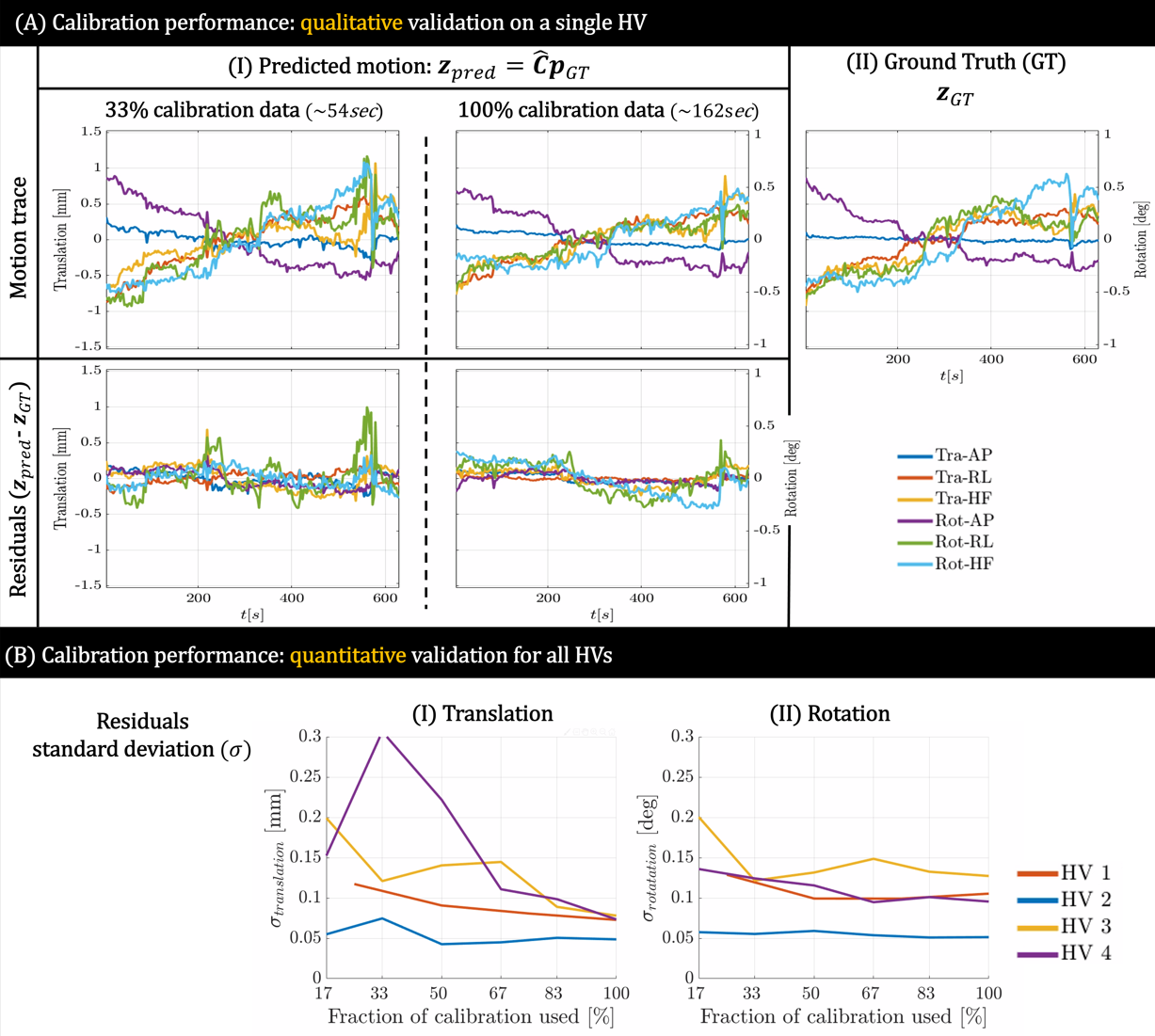
To test our hypothesis, synthetic k-space data was created by extracting 33/67/100% of the calibration acquisitions distributed across time, corresponding to a TA=54/108/120sec. For each synthetic dataset, $$$\textbf{z}_{calib}$$$ was estimated by performing alignedSENSE and used to construct $$$\hat{\textbf{C}_{calib}}$$$ (Eq.3). We validated the calibration fit by predicting motion parameters for the DISORDER MPRAGE.
Image reconstruction:
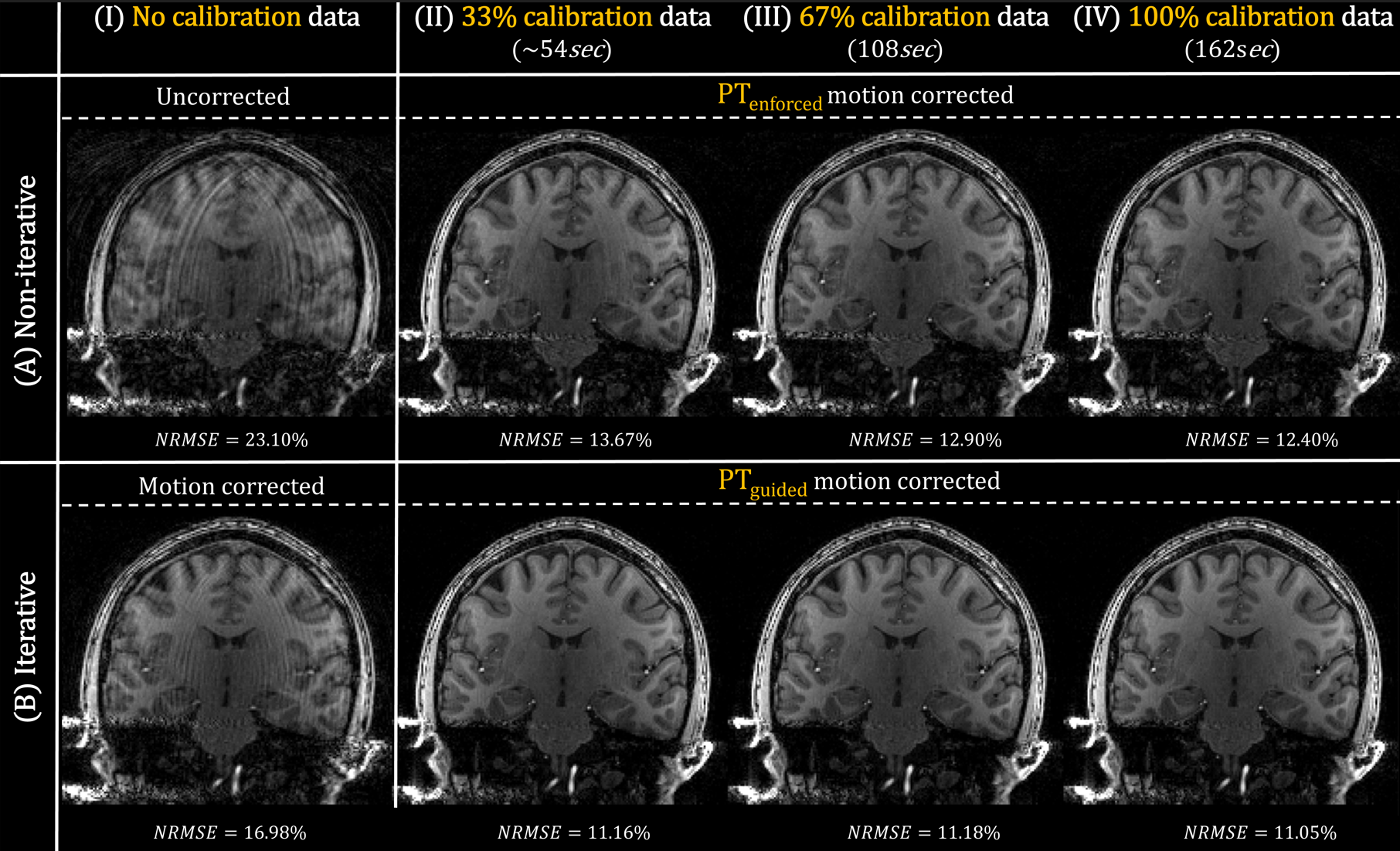
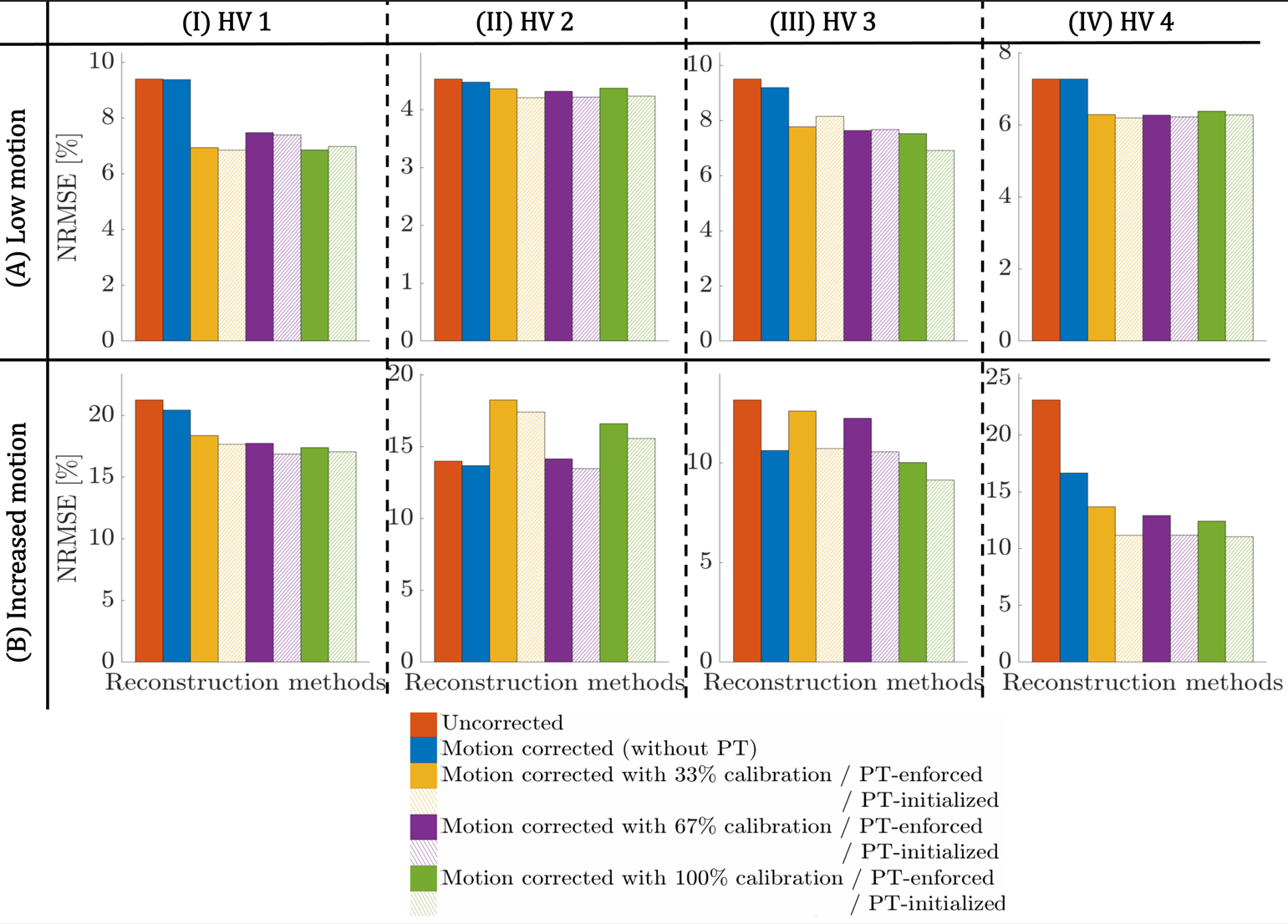
Standard linear MPRAGE data was reconstructed without correction, with alignedSENSE correction, with correction using motion states predicted by $$$\hat{\textbf{C}_{calib}}$$$ (PTenforced-alignedSENSE), and with the proposed calibration refinement using Eq.2 (PTguided-alignedSENSE). Image quality is quantified using normalized root-mean-squared errors (NRMSE)16 relative to the motion-corrected DISORDER MPRAGE.
Results and discussion
Fig2A shows motion predictions for the DISORDER MPRAGE when using 33 and 100% of the ERIC protocol. $$$\hat{\textbf{C}_{calib}}$$$ can predict the main motion trend for both cases; better fits are obtained when more calibration data is used. Fig2B shows a relatively small standard deviation ($$$\sigma$$$) of residuals (<0.3mm/0.2deg) for all HV and confirms this observation. Fig3 shows the reconstruction of linear MPRAGE for HV4. Using $$$\hat{\textbf{C}_{calib}}$$$ only (A.II-IV) outperforms conventional correction (B.I), even when using 33% of the data. The proposed data-driven refinement achieves improved correction (B.II-IV). Finally, Fig4 shows NRMSE for all HV and correction methods. Overall, PT-alignedSENSE improves image quality. The amount of calibration data needed for improved correction depends on HV, advocating the flexible approach presented here.Conclusion
We propose ERIC, Efficient, Robust and Instruction-free Calibration that builds a PT motion model leveraging state-of-the-art motion estimation with a flexible acquisition protocol. Combining such protocol with data-driven calibration refinement on a per-scan basis can improve performance, even when using a subset of calibration data.Acknowledgements
This work was funded by the King’s College London & Imperial College London EPSRC Centre for Doctoral Training in Medical Imaging [EP/S022104/1], by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z], the Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z] and by the National Institute for Health Research (NIHR) Clinical Research Facility based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and/or the NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.References
[1] Zaitsev, Maxim et al. “Motion artifacts in MRI: A complex problem with many partial solutions.” Journal of Magnetic Resonance Imaging 42 (2015).
[2] van Niekerk, Adam et al. “Toward “plug and play” prospective motion correction for MRI by combining observations of the time-varying gradient and static vector fields.” Magnetic Resonance in Medicine 82 (2019): 1214 - 1228.
[3] Stucht, Daniel et al. “Highest Resolution In Vivo Human Brain MRI Using Prospective Motion Correction.” PLoS ONE 10 (2015)
[4] Jorge, João et al. “Tracking discrete off‐resonance markers with three spokes (trackDOTS) for compensation of head motion and B0 perturbations: Accuracy and performance in anatomical imaging.” Magnetic Resonance in Medicine 79 (2018).
[5] Laustsen, Malte et al. “Tracking of rigid head motion during MRI using an EEG system.” Magnetic Resonance in Medicine 88 (2022): 986 - 1001.
[6] Cordero-Grande, Lucilio et al. “Motion‐corrected MRI with DISORDER: Distributed and incoherent sample orders for reconstruction deblurring using encoding redundancy.” Magnetic Resonance in Medicine 84 (2019): 713 - 726.
[7] Polak, Daniel et al. “Scout accelerated motion estimation and reduction (SAMER).” Magnetic Resonance in Medicine 87 (2021): 163 - 178.
[8] Speier, Peter et al. “PTnav: a novel respiratory navigation method for continuous acquisitions based on modulation of a pilot tone in the MR-receiver.” Magn Reson Mater Phys Biol Med 28, S97–S98 (2015).
[9] Bacher, Mario et al. “Cardiac Triggering Based on Locally Generated Pilot-Tones in a Commercial MRI Scanner: A Feasibility Study.” October 2017.
[10] Ludwig, Juliane et al. “Pilot tone–based motion correction for prospective respiratory compensated cardiac cine MRI.” Magnetic Resonance in Medicine 85 (2020): 2403 - 2416.
[11] Wilkinson, Tom et al. “Motion Estimation for Brain Imaging at Ultra-High Field Using Pilot-Tone: Comparison with DISORDER Motion Compensation.” In: Proc Int Soc Mag Reson Med 30.
[12] Cordero-Grande, Lucilio et al. “Sensitivity Encoding for Aligned Multishot Magnetic Resonance Reconstruction.” IEEE Transactions on Computational Imaging 2 (2016): 266-280.
[13] Brackenier, Yannick et al. “Pilot Tone meets DISORDER: Improved data-driven motion corrected brain MRI by leveraging Pilot Tone signal variations.” In: Proc Int Soc Mag Reson Med 31.
[14] Kent, James et al. “Pilot Tone vs pTx Scattering: A Comparison between ‘RF Sensor’ Methods for Rigid Body Motion Detection of the Brain at 7T.” In: Proc Int Soc Mag Reson Med 32.
[15] Huttinga, Niek et al. “Three-dimensional rigid head motion correction using the Beat Pilot Tone and Gaussian Processes.” In: Proc Int Soc Mag Reson Med 32.
[16] McGee, Kiaran P. et al. “Image metric‐based correction (Autocorrection) of motion effects: Analysis of image metrics.” Journal of Magnetic Resonance Imaging 11 (2000).
Figures