0374
Radiomics for predicting Grades, IDH mutation and MGMT promoter methylation of Adult Diffuse Gliomas: Combination of structural MRI, ADC and SWI1Department of Radiology, Department of Radiology, The Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing University, Nanjing, China
Synopsis
Keywords: Tumors (Pre-Treatment), Tumor, Glioma; SWI; ADC; Machine learning
Motivation: WHO Grade, IDH mutation and MGMT promoter methylation are important for precise diagnosis and treatment plans for diffuse glioma patients.
Goal(s): This study aimed to investigate the predictive value of radiomics features extracted from Structural MRI, ADC and SWI.
Approach: Radiomic features were extracted from T1WI, T2WI, T1CE, FLAIR, ADC and SWI. Analysis of variance F-test were used for feature selection. 11 classifiers were utilized for model establishment.
Results: For WHO Grade task, the highest AUC was 0.990; for IDH mutation task, the highest AUC was 0.947. All the constructed models failed to predict MGMT promoter methylation status efficiently.
Impact: This work will help neuro-oncologists better understand the radiological manifestation of gliomas.
Intraduction
Gliomas are the most common type of primary intracranial tumors among the world1. Susceptibility-weighted imaging (SWI) is a useful MRI sequence to depict tumor microvasculature and microhemorrhage2. SWI can hemi-quantitatively assess tu-mor vessels and blood products through intra-tumoral susceptibility signals (ITSS).Right now, there is no research investigating the value of radiomic features extracted from SWI in predicting grade, IDH mutation and MGMT promoter methylation status, which deserves further exploration. The purpose of this study is to investigate the value of conventional structural MRI, ADC and SWI radiomic features, especially SWI radiomic features to predict glioma grade and molecular marker.
Materials and Methods
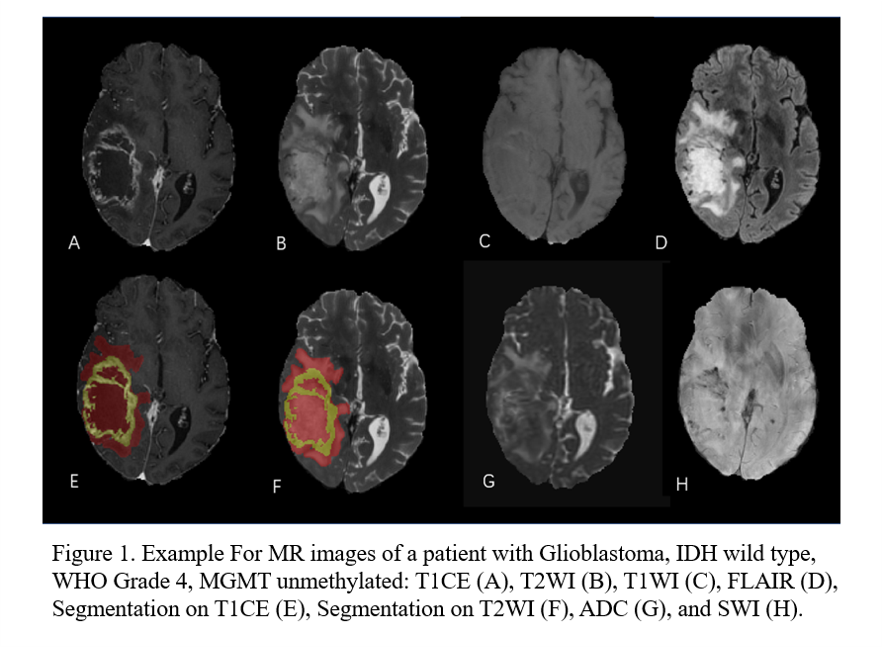
The public retrospective dataset the University of California San Francisco Pre-operative Diffuse Glioma (UCSF-PDGM) were used in this paper.The Grade of tumors analyzed in this study were histopathologically confirmed according to 2021 WHO CNS5. Grade 2 and 3 patients are defined as “low grade” while Grade 4 patients were defined as “high grade”. All the patients’ tumor samples resected from surgery were tested for IDH1 and IDH2 mutation by either next-generation genetic sequencing (NGS) or conventional (Sanger) sequencing. If any mutation was detected on IDH1 R132 or IDH2 R172, the IDH label would be defined as “IDH-mutant”. Otherwise, the IDH label would be defined as “IDH-negative”. For all grade 3 and 4 patients, MGMT promoter methylation was tested by quantitative methylation polymerase chain reaction assay. If two or more methylation sites were detected, the MGMT label would be defined as “methylated”. Otherwise, the MGMT label would be defined as “unmethylated”.
All preoperative MRI data analyzed in this present research was acquired with a 3.0T MRI scanner (Discovery 750; GE Healthcare) with eight-channel head coil (In Vivo). The Sequences used in this study Included T1WI, T2WI, T1CE, FLAIR, ADC and SWI. Each sequence was registered and resampled to a 1×1×1mm voxel resolution.
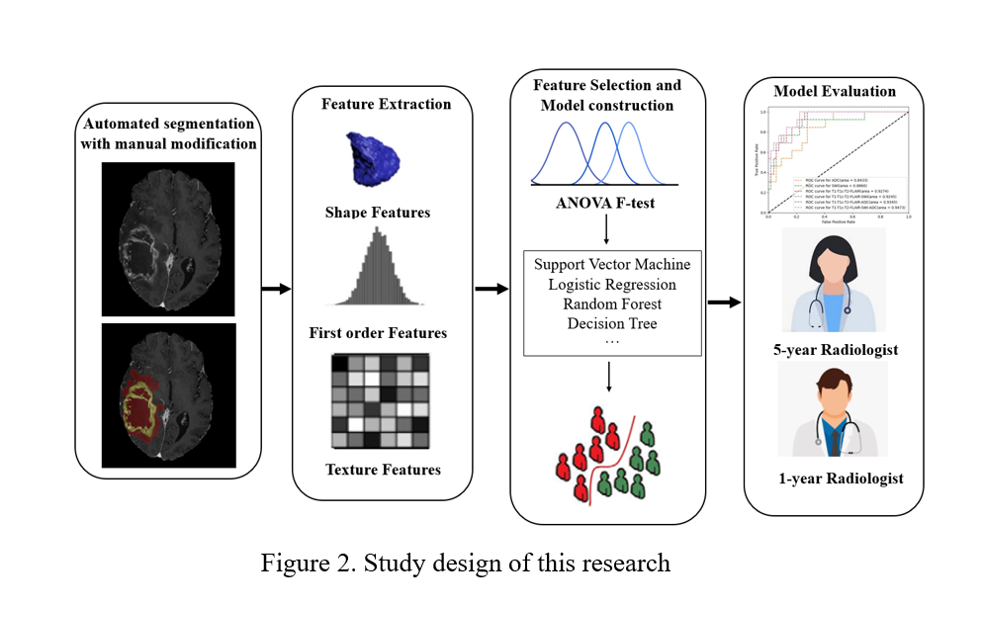
We defined 2 ROI in this research. Tumor Core (TC) consists of enhancing tumor parenchyma, non-enhancing tumor parenchyma and necrosis area. Whole Tumor (WT) consists of TC and surrounding edema area. WT was delineated on T2WI. We extracted radiomic features utilizing Pyradiomics. Analysis of variance F-test were used for feature selection. 11 classifiers were utilized for model establishment. ROC curves were used to evaluate the predictive performance. We also compared the performance of Radiomics models with a 5-year radiologist and a 1-year radiologist.
Results
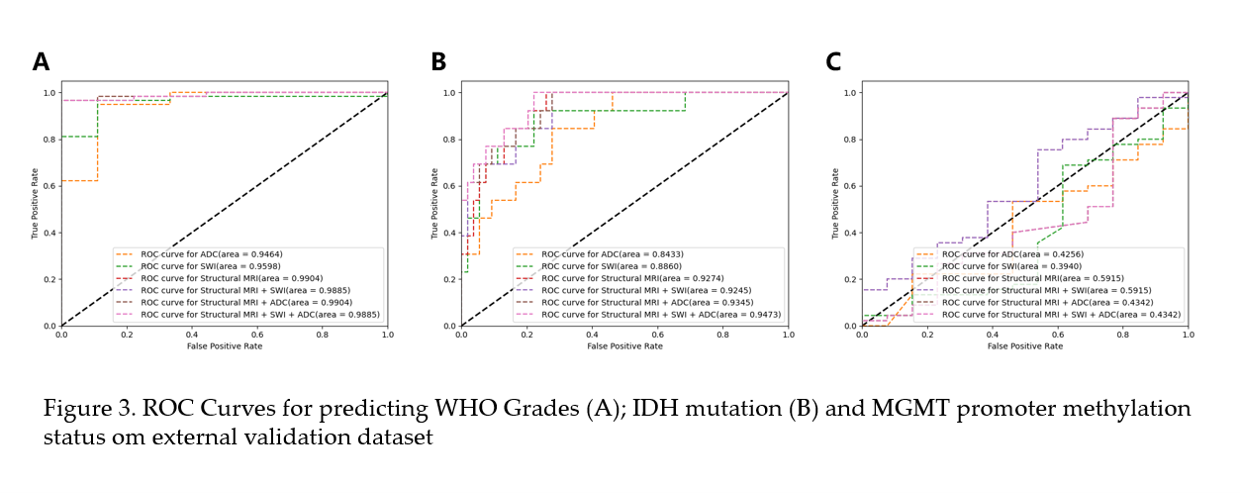
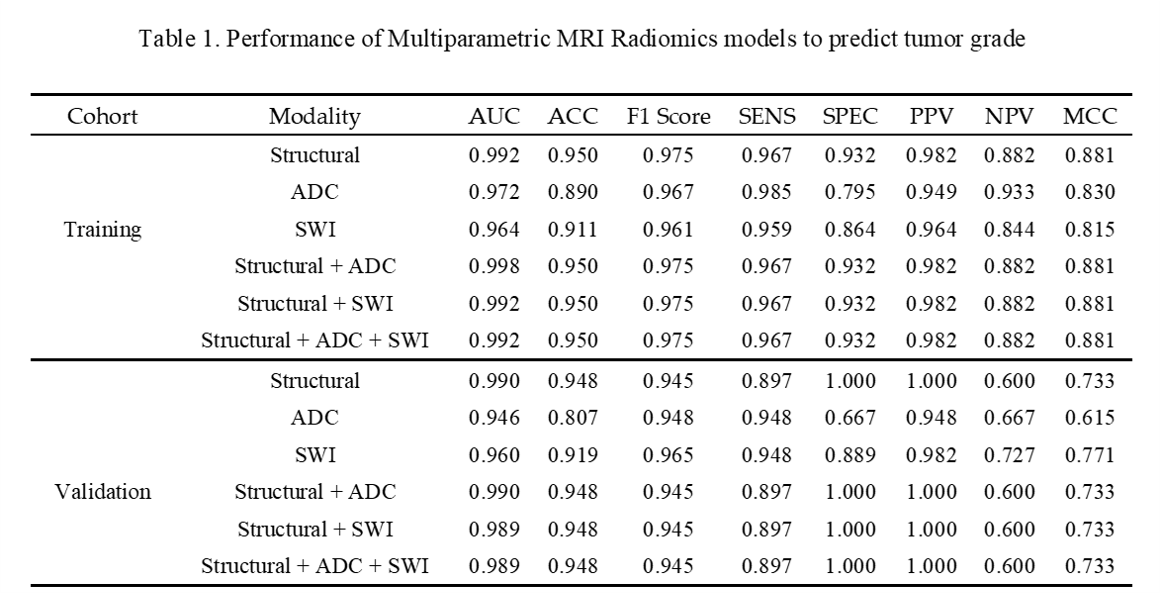
A total of 426 patients with complete MRI imaging data who didn’t receive pre-operational biopsy were enrolled in the training cohort to establish radiomics models. The other 67 patients who received burr-hole biopsy before MRI imaging were enrolled in the external validation cohort to evaluate the efficacy and performance of models.For WHO grades prediction task, logistic regression achieved the highest efficacy. The modality Structural plus ADC exhibited the highest AUC on both training cohort (0.998) and external validation cohort (0.990). The accuracy of 5-year radiologist and 1-year radiologist were 0.866 and 0.761 separately.
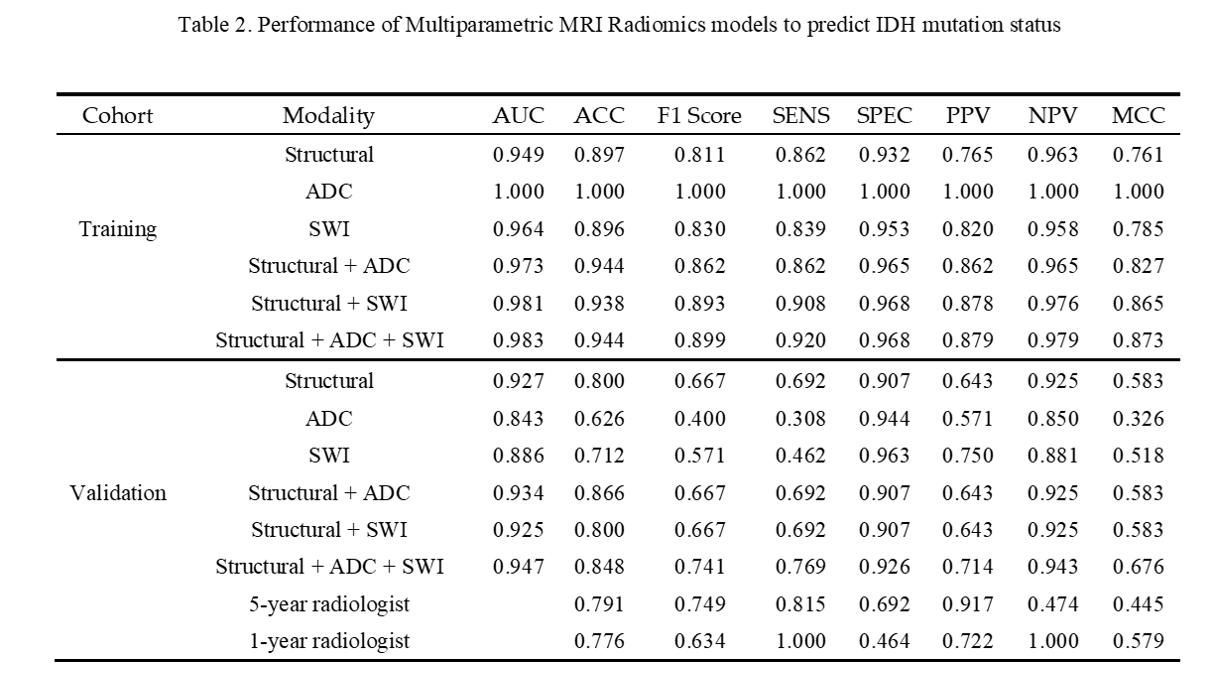
For IDH mutation prediction task, SVM achieved the highest efficacy. The modality ADC exhibited the highest AUC on the training cohort (1.000) and the modality Structural plus ADC plus SWI exhibited the highest AUC on external validation cohort (0.947). The accuracy of 5-year radiologist and 1-year radiologist were 0.791 and 0.776 separately.
For MGMT promoter methylation prediction task, The modality Structural plus ADC and Structural plus ADC plus SWI exhibited the highest AUC on the training cohort (0.545) and the modality Structural and Structural plus ADC plus SWI exhibited the highest AUC on external validation cohort (0.591). The accuracy of 5-year radiologist and 1-year radiologist were 0.672 and 0.552 separately.
Discussion
To the best of our knowledge, this is the first research investigating the value of SWI radiomics features in predicting WHO grades, IDH mutation and MGMT promoter status of adult diffuse gliomas. In previous study, researches tried to apply ITSS, which is a semi-quantitative metric depicting the vasculature and micro-hemorrhage within the tumor to evaluate the grade and IDH mutation3.High-grade gliomas appear to have more neovascularization than low-grade gliomas, which is reflected by more foci of susceptibility within the tumor on SWI sequences. In this study, SWI radiomics model illustrated good efficacy to predict high-grade glioma and low-grade glioma.
IDH wild type glioblastomas also tend to have more micro-hemorrhage foci within the tumor parenchyma, resulting in high ITSS on SWI. SWI can provide valuable extra microstructural information compared with Structural MRI and ADC, elevating the performance and efficacy of radiomics models to predict IDH mutation status.
Acknowledgements
No acknowledgement found.References
1. SHOBEIRI P, SEYEDMIRZAEI H, KALANTARI A, et al. The Epidemiology of Brain and Spinal Cord Tumors [J]. Adv Exp Med Biol, 2023, 1394: 19-39.
2. SAINI J, GUPTA P K, SAHOO P, et al. Differentiation of grade II/III and grade IV glioma by combining "T1 contrast-enhanced brain perfusion imaging" and susceptibility-weighted quantitative imaging [J]. Neuroradiology, 2018, 60(1): 43-50.
3. KONG L W, CHEN J, ZHAO H, et al. Intratumoral Susceptibility Signals Reflect Biomarker Status in Gliomas [J]. Sci Rep, 2019, 9(1): 17080.
Figures