0365
Personalized Radiotherapy Clinical Target Volume from a novel DTI-derived Tumour Spread Index (TSI) map1Physics and Astronomy, University of Manitoba, Winnipeg, MB, Canada, 2Paul Albrechtsen Research Institute, CancerCare Manitoba, Winnipeg, MB, Canada, 3Radiology, University of Manitoba, Winnipeg, MB, Canada, 4Radiation Oncology, CancerCare Manitoba, Winnipeg, MB, Canada, 5Medical Physics, CancerCare Manitoba, Winnipeg, MB, Canada, 6Internal Medicine, University of Manitoba, Winnipeg, MB, Canada
Synopsis
Keywords: Tumors (Pre-Treatment), Radiotherapy, Glioblastoma
Motivation: GBM patients suffer from poor treatment outcome. The current radiotherapy planning (i.e. GTV, CTV, PTV) does not adjust the CTV margin to account for the microscopic spread of the glioma tumour cells along white matter fiber tracts.
Goal(s): Utilizing DTI MRI to tailor the CTV margin to each patient's unique tumour progression pathway.
Approach: Pre-surgical DTI-based tractography was used to quantify tumor spread probability, producing the Tumour Spread Index (TSI) map, which was used to generate a personalized CTV.
Results: This proof-of-concept study showed that using DTI-based tractography with a TSI map to personalize CTV improved coverage of recurrent regions in follow-up imaging.
Impact: Utilizing tractography to map the probable path of tumour spread and use this to direct radiation is a new paradigm in targeted radiotherapy which may lead to improved progression free survival in GBM patients.
Introduction
Grade IV glioma cells infiltrate healthy brain tissue by extending through white matter (WM) fiber tracts1,2. However, radiotherapy (RT) of glioblastoma (GBM), the most aggressive type of brain tumour, currently does not account for this. RT planning begins with outlining the Gross Tumour Volume (GTV), with a 15-20 mm fixed spatial margin (Clinical Target Volume - CTV) to account for potential microscopic tumour spread around GTV, and an additional 5 mm margin (Planning Target Volume - PTV) to accommodate set-up errors or patient movements during treatment3. The aim of this study was to use diffusion tensor imaging (DTI) to generate a new metric – the Tumour Spread Index (TSI) - to quantitatively define the probable path of tumour spread via white matter fiber tracts and personalize the radiation margin definition beyond GTV. We hypothesize that the TSI map can serve as a predictive tool for identifying patterns of likely recurrence in patients with GBM and therefore be used to modify the delivery of radiation treatment to proactively target regions at high risk of tumor spread.Methods
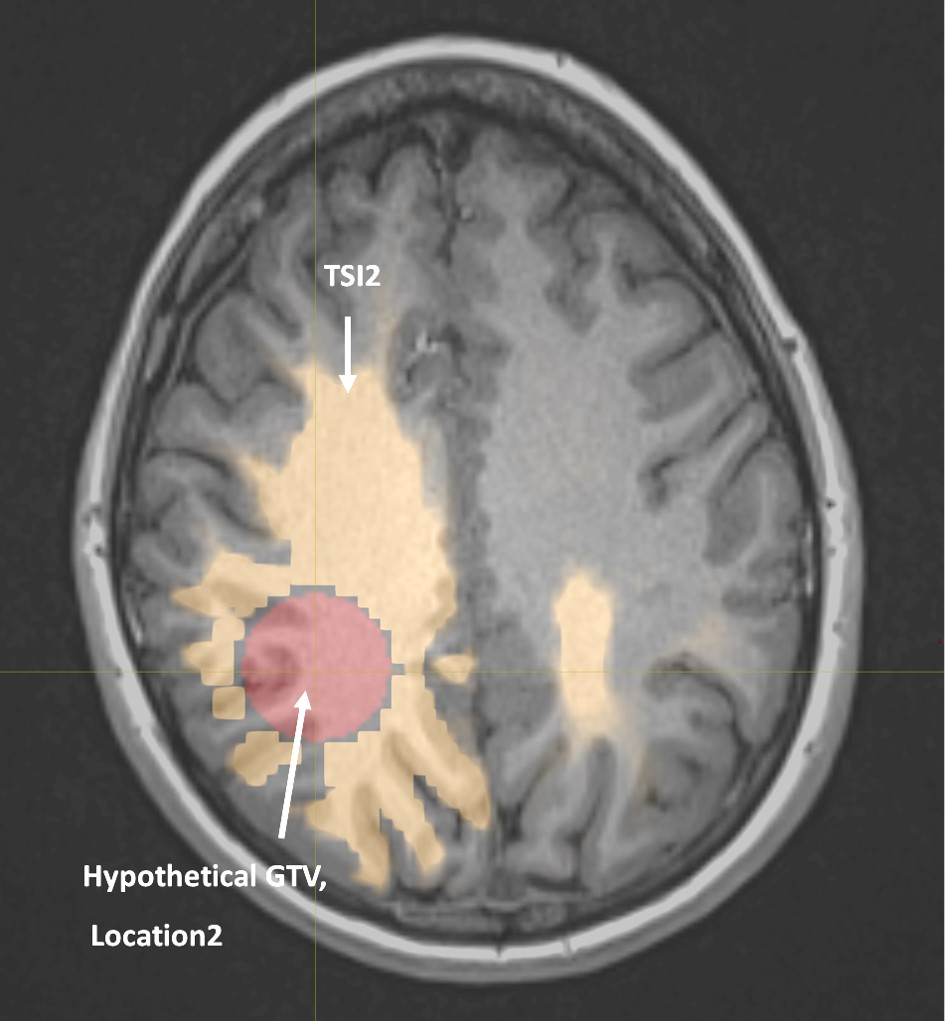
The imaging included pre-operative single shell DTI scan (single shell, b=0, b=1000 s/mm²; 30 directions; matrix 128×128; 70 slices; voxel size 2.5×2.5×2.5 mm³), and high-resolution post-contrast T1-weighted image (T1w-CE) (matrix 256×256; 208 slices; voxel size 0.98×0.98×0.98 mm³). MRtrix34, a widely-used open-source software, was utilized for the pre-processing steps and performing probabilistic tractography. In-house MATLAB code was used to calculate $$TSI = \sum_{i=1}^n\frac{D_i\times W_i}{L_i^2}$$ Where ‘i’ is the fiber tract index within the voxel of interest, ‘n’ represents the number of fiber tracts connecting to the tumor per voxel, ‘D’ represents the mean axial diffusion rate along each tract, ‘W’ represents the fiber density correction weighting factor, and ‘L’ represents the fiber length from the voxel of interest to the tumour surface. The resulting TSI map was thresholded to create an adaptable-width personalized Clinical Target Volume (pCTV) margin encompassing the tumor. A modified Volumetric Modulated Arc Therapy (mVMAT) treatment plan was then developed using the pCTV margin and compared to the original VMAT plan. The pPTV, derived from the pCTV margin, was subsequently compared to the original PTV. An 8-month post-surgery MRI was used to assess TSI map's predictions accuracy by overlaying treatment plans and evaluating radiation doses in areas of recurrence.Additionally, advanced DTI imaging from a healthy volunteer was obtained to explore how TSI could predict tumor growth patterns based on eight independent hypothetical GTV shapes and positions in the brain. We aimed to identify the relationship between tumor location and different shapes and the potential pathway of microscopic tumor cells and assess TSI value variations. The imaging included a multi-shell DTI dataset (b=1000, b=2000 s/mm2; 45 directions, matrix 128×128; 75 slices; voxel size 2×2×2 mm³, A-P and P-A phase encoding directions), and T1w data (matrix 256×256; 208 slices; voxel size 0.98×0.98×0.98 mm³).
Results
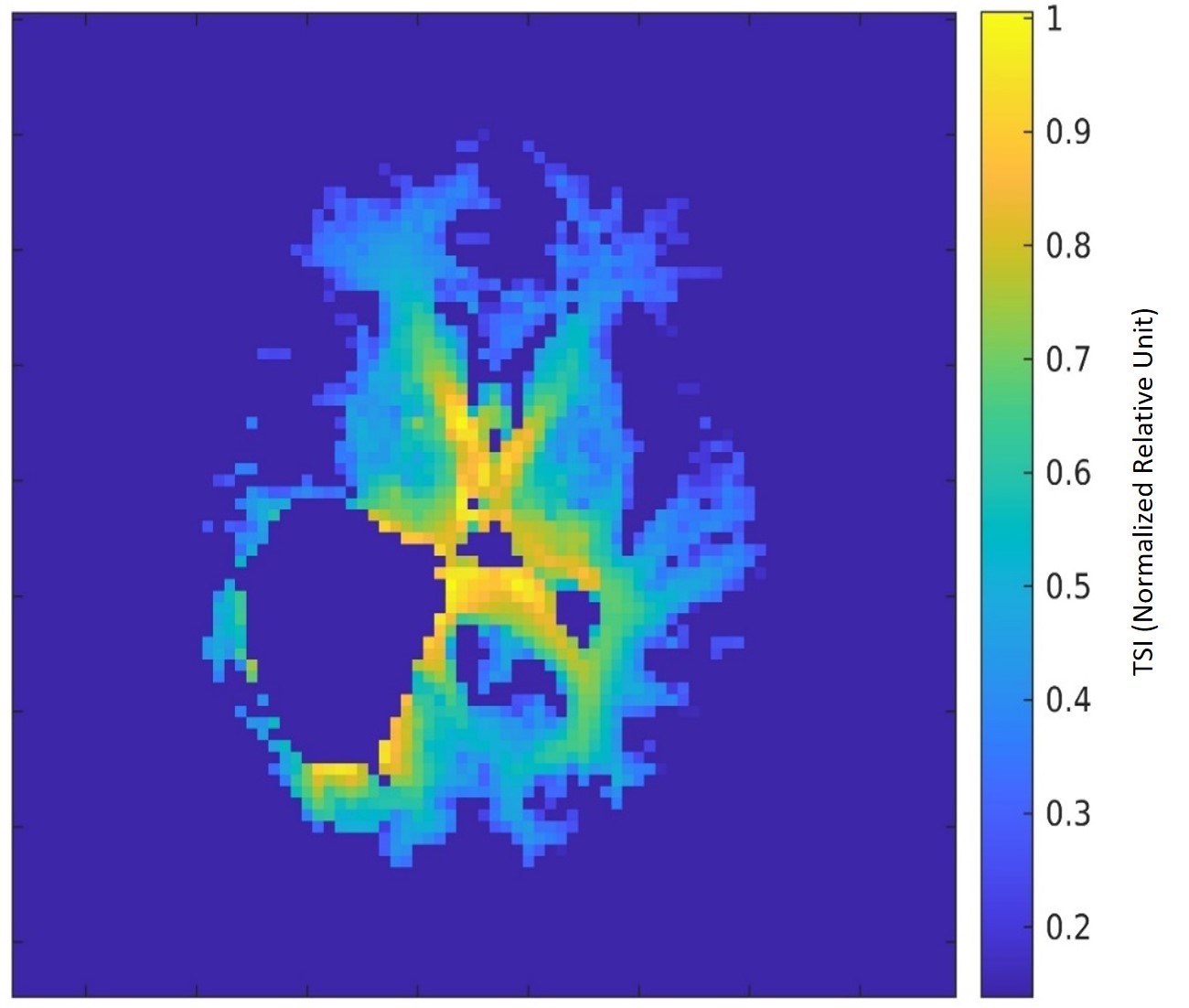
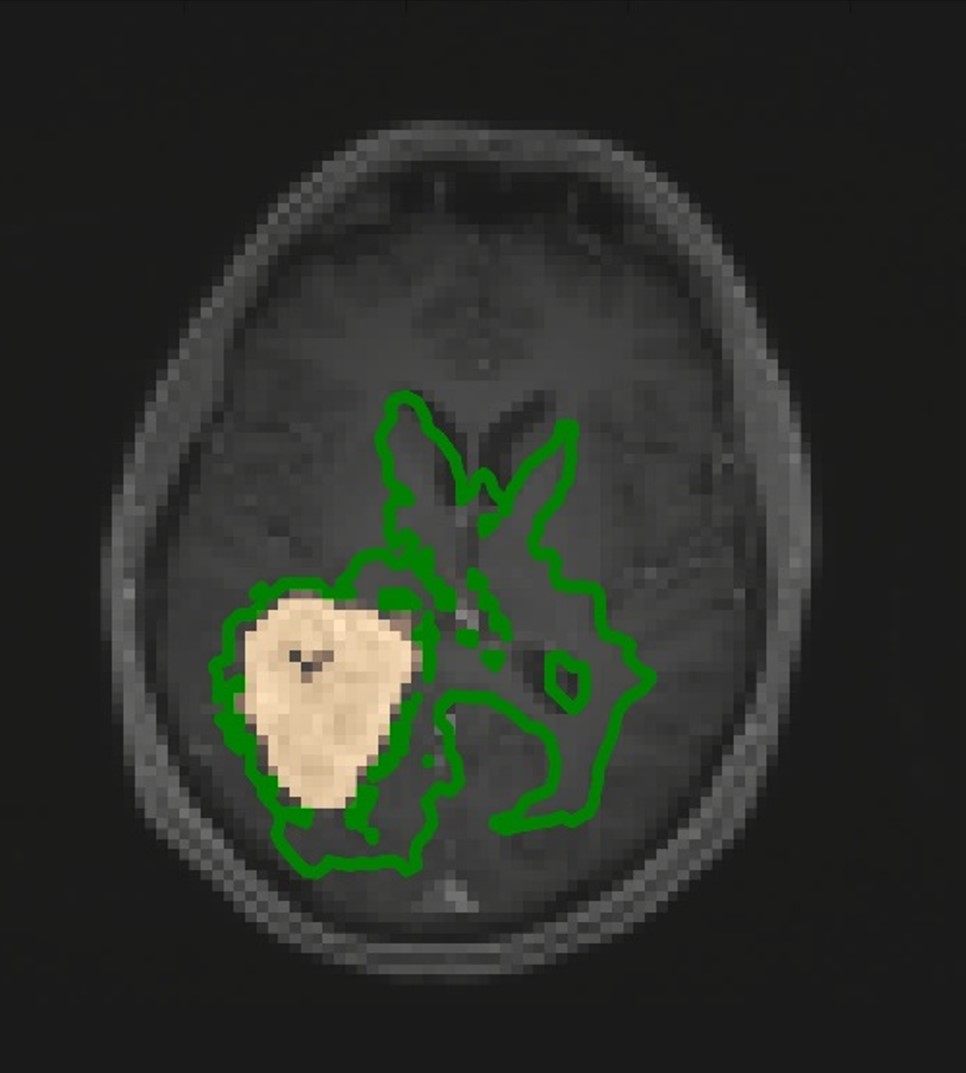
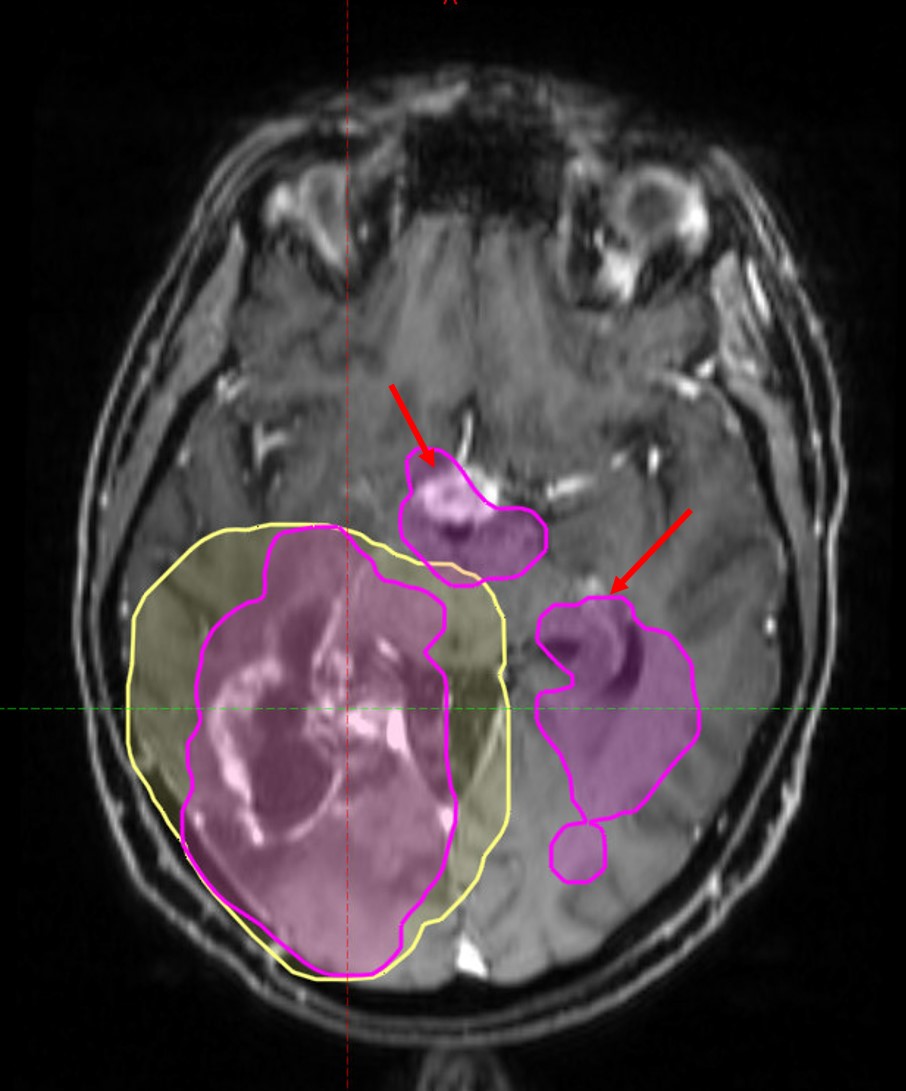
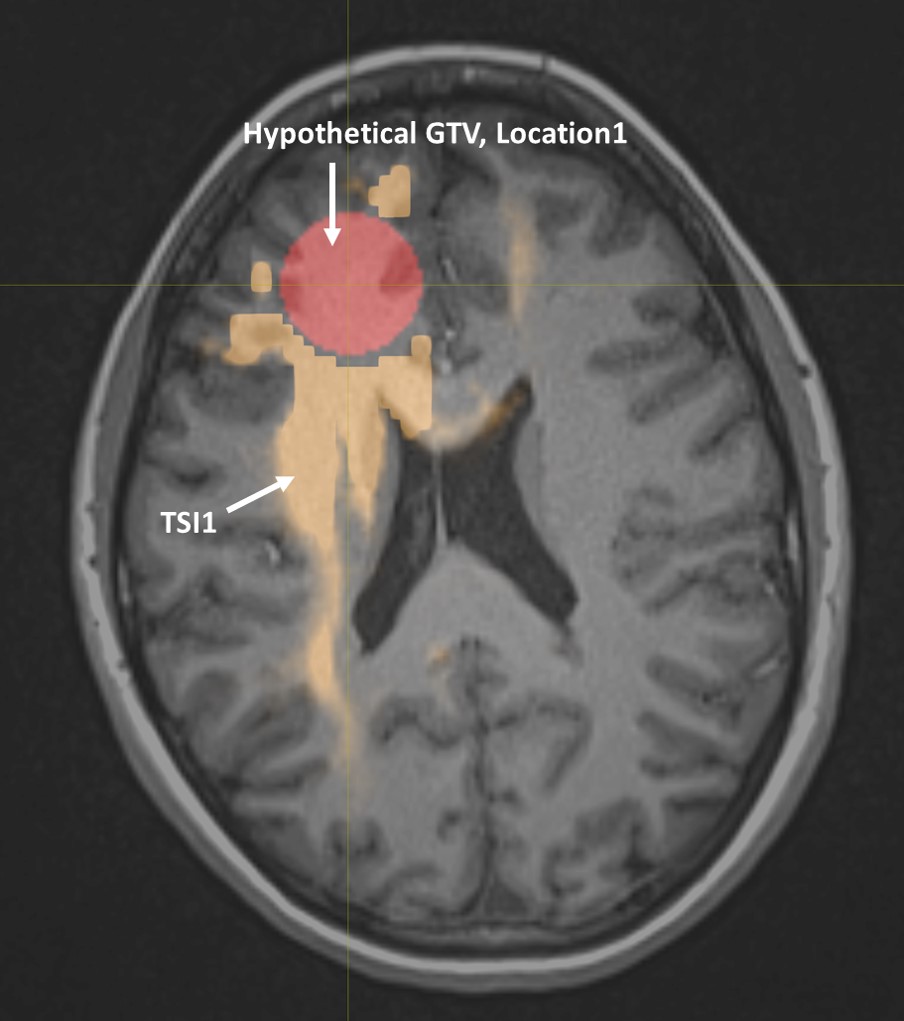
Figure 1 shows the TSI map result of the central slice through the tumour. The generated TSI map represents relative values, with yellow indicating a greater likelihood of microscopic tumor cells spread and blue indicating a relatively lower probability of spread. This map was thresholded to generate a pCTV contour, figure 2. Analysis of the GBM patient dataset revealed that pCTV extended beyond the CTV margin in some regions (by 21% of the original CTV volume) and reduced below the CTV margin in other regions (by 42% of the original CTV volume), resulting in a net 21% decrease in PTV. In the follow-up MRI, the mVMAT and original VMAT plans administered an average mean dose of 80% and 63% of the prescribed dose to the recurrent areas, respectively, figure 3. This suggested that the mVMAT plan may have better controlled the recurrence. Additionally, the volunteer dataset showed TSI variations dependent on the location and shape of GTV within the brain, figures 4-5.Conclusion
A novel MRI-based quantitative metric - Tumour Spread Index (TSI) - was developed to investigate the possibility of personalizing the radiotherapy Clinical Target Volume (CTV) based on probabilistic tractography. The predictive capability of the TSI map was investigated by examining the actual tumour recurrence in the 8-month post-surgery MRI images. The result from this proof-of-concept study demonstrated the potential value of the TSI map in personalizing CTV and predicting recurrence locations. Additionally, the dataset from the volunteer demonstrated that TSI would vary depending on the shape and location of GTV within the brain. Further research with a larger cohort is warranted to validate these findings and explore the clinical implications, potentially paving the way for more personalized and effective treatment strategies in GBM patients.Acknowledgements
This work was supported by the CancerCare Manitoba Foundation and the University of Manitoba Graduate Fellowship, Winnipeg, MB, Canada.
References
1. Stroebe H. Ueber Entstehung und Bau der Gehirngliome. Beitr Pathol Anat Allg Pathol. 1895;19:405-486.
2. Scherer H. The forms of growth in gliomas and their practical significance. 1940;63:1-35.
3. Niyazi M, Brada M, Chalmers AJ, et al. ESTRO-ACROP guideline “target delineation of glioblastomas.” Radiotherapy and Oncology. 2016;118(1):35-42.
4. Tournier JD, Smith R, Raffelt D, et al. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. NeuroImage. 2019;202:116137-116137.
Figures