0362
Feasibility of 3D APT and NOE mapping using extrapolated semi-solid magnetization transfer reference fitting in brain tumors1Department of Molecular Imaging & Diagnosis, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Philips Research, Hamburg, Germany, 3Division of Radiology, Department of Medical Technology, Kyushu University Hospital, Fukuoka, Japan, 4Department of Clinical Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan
Synopsis
Keywords: Tumors (Pre-Treatment), CEST & MT
Motivation: Currently, APT and NOE imaging with extrapolated semi-solid magnetization transfer reference (EMR) fitting has been performed with single-slice acquisition.
Goal(s): To demonstrate the feasibility of 3D APT and NOE imaging with EMR fitting using the 3D CEST sequence with CS-SENSE in patients with brain tumors.
Approach: 3D CEST imaging with CS-SENSE was adjusted to clinical scan. EMR fitting was performed on the 3D data.
Results: 3D APT and NOE mapping was feasible in all patients with brain tumors by using the 3D CEST imaging with CS-SENSE within a clinically acceptable acquisition time.
Impact: The feasibility of 3D APT and NOE mapping using 3D CEST imaging with CS-SENSE was demonstrated. Quantitative evaluation of APT and NOE on multiple slices allows for the quantitative assessment for the entire tumor area.
Introduction
Chemical exchange saturation transfer (CEST) imaging is based on chemical exchange between free bulk water and solute protons and is influenced by direct water saturation (DS), semi-solid macromolecular magnetization transfer (MT) and nuclear Overhauser enhancement (NOE). The usefulness of glioma grading using amide proton transfer (APT)-weighed imaging with MT-ratio asymmetry (MTRasym) at 3.5 ppm has been reported1, but MTRasym does not reflect pure amide CEST because it can be affected by NOE at -3.5 ppm. A fitting approach using extrapolated semi-solid MT reference (EMR) signals has been reported to separately quantify APT (APT#) and NOE (NOE#) signals in 2D CEST imaging2, 3. EMR fitting requires a long scan time acquiring multiple frequency offsets ( -8ppm to +14 ppm) and thus, application to 3D imaging was difficult. Recently, we have developed a 3D CEST imaging scheme to acquire full z-spectra in multiple slices by combining 3D CEST imaging with compressed sensing and sensitivity encoding (CS-SENSE) in a clinically acceptable scan time (~5min)4. Here, the aim is to demonstrate the feasibility of 3D APT and NOE mapping with EMR fitting in brain tumors using CS-SENSE accelerated 3D CEST.Methods
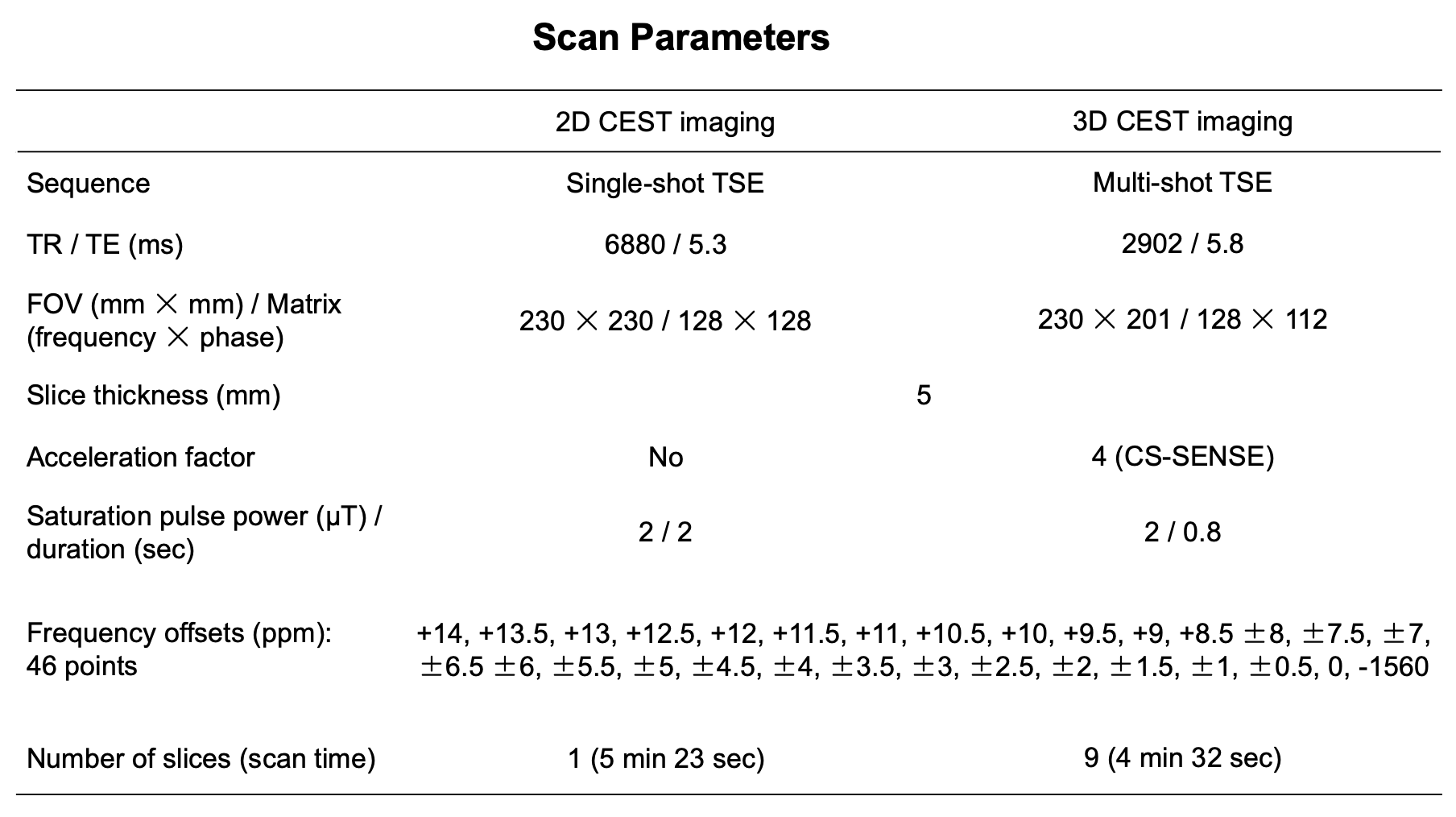
A 3.0T MRI-scanner (Ingenia, Philips, Netherlands) with 2-channel body-coil transmission and 20-channel head coil reception was used with the following parameters: CEST images (Figure 1); 3D multi-shot fast spin-echo, TR/TE = 2902/5.8ms, FOV = 230× 201mm2, voxel size = 1.8×1.8×5 mm3, CS-SENSE factor = 4, 9 slices, acquisition time 4 min 32 sec, saturation pulse power / length = 2.0μT/800ms, frequency offsets relative to water (46 points) =+14…-8 ppm (step 0.5 ppm) and -1560 ppm, B0 map; 3D fast field echo, TR/TE = 14 /7.5ms, FOV = 230×201mm2, voxel size = 1.8×1.8×5mm3, CS-SENSE factor = 2, 9 slices, acquisition time = 45 sec. For comparison, single-slice 2D CEST imaging was performed using the parameters shown in Figure 1.All image data were analyzed using the software program ImageJ (ver. 1.52a; U.S. National Institutes of Health, Bethesda, MD). A dedicated plug-in was created using Lorentzian-Gaussian EMR background fitting5 (4 parameters: Amplitude A; Gauss/Lorentz relative weights we; Gaussian width w1; Lorentzian width w2) on 18 frequencies (±6.0,±1.22,±1.0,±0.47,0,+7, +8…+14ppm) after interpolation-based B0 correction to assess APT# and NOE# (fit residuals) as well as MTRasym at 3.5 ppm. APT#, NOE# and MTRasym at 3.5 ppm were measured on manually drawn ROIs in the FLAIR hyperintense lesion and normal appearing white matter (NAWM) in patients #1 and #2 and in the enhancing lesion and NWAM in patient #3.Three patients with diffuse gliomas (patient #1, oligodendroglioma, 1p19q-codeleted, CNS WHO grade 2; patient #2, astrocytoma, IDH-mutant, CNS WHO grade 3; patient #3, glioblastoma, IDH-wildtype, CNS WHO grade 4) were scanned with the 3D CEST sequence with CS-SENSE (IRB approved study and informed consent obtained).
Results
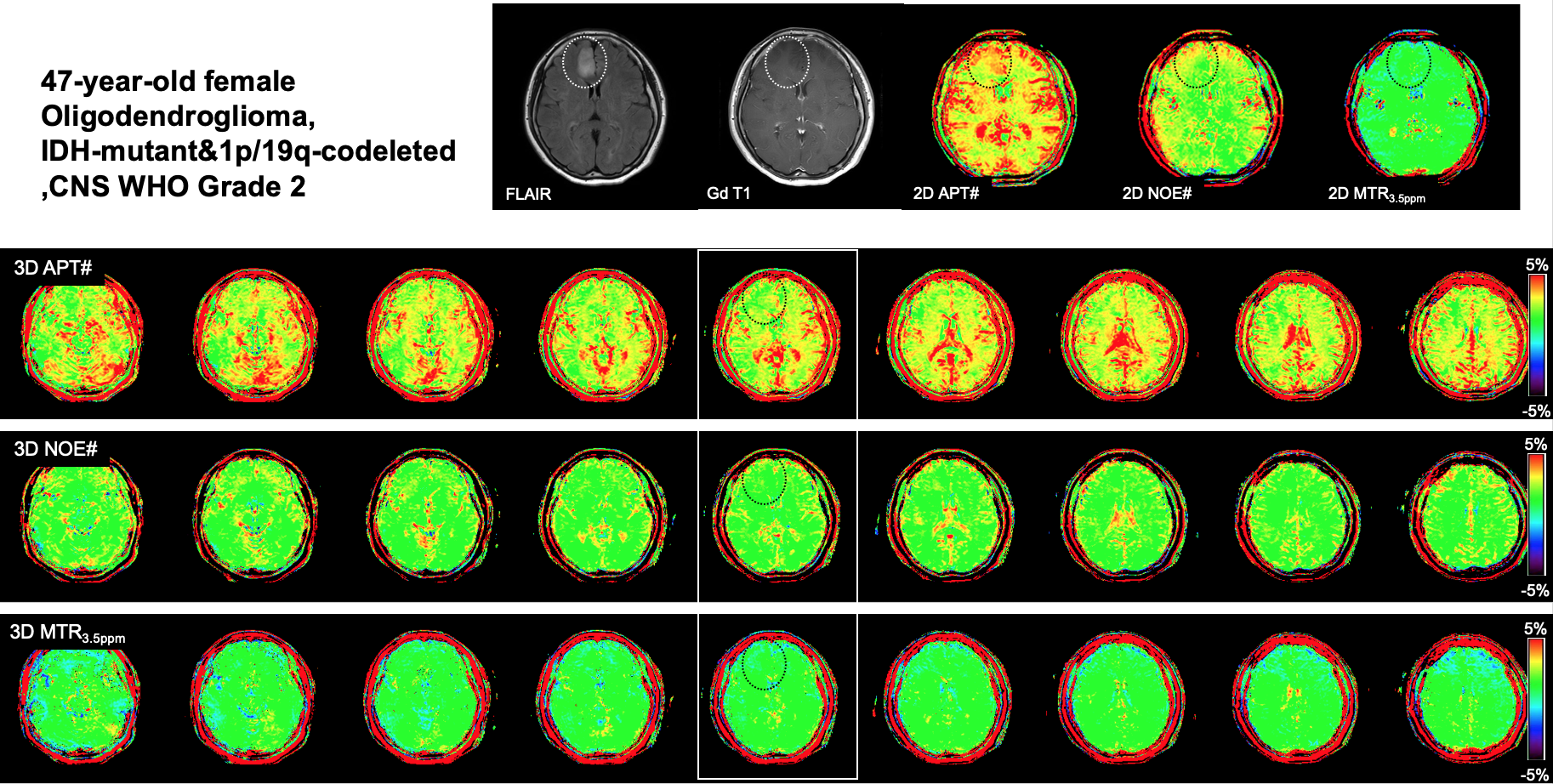
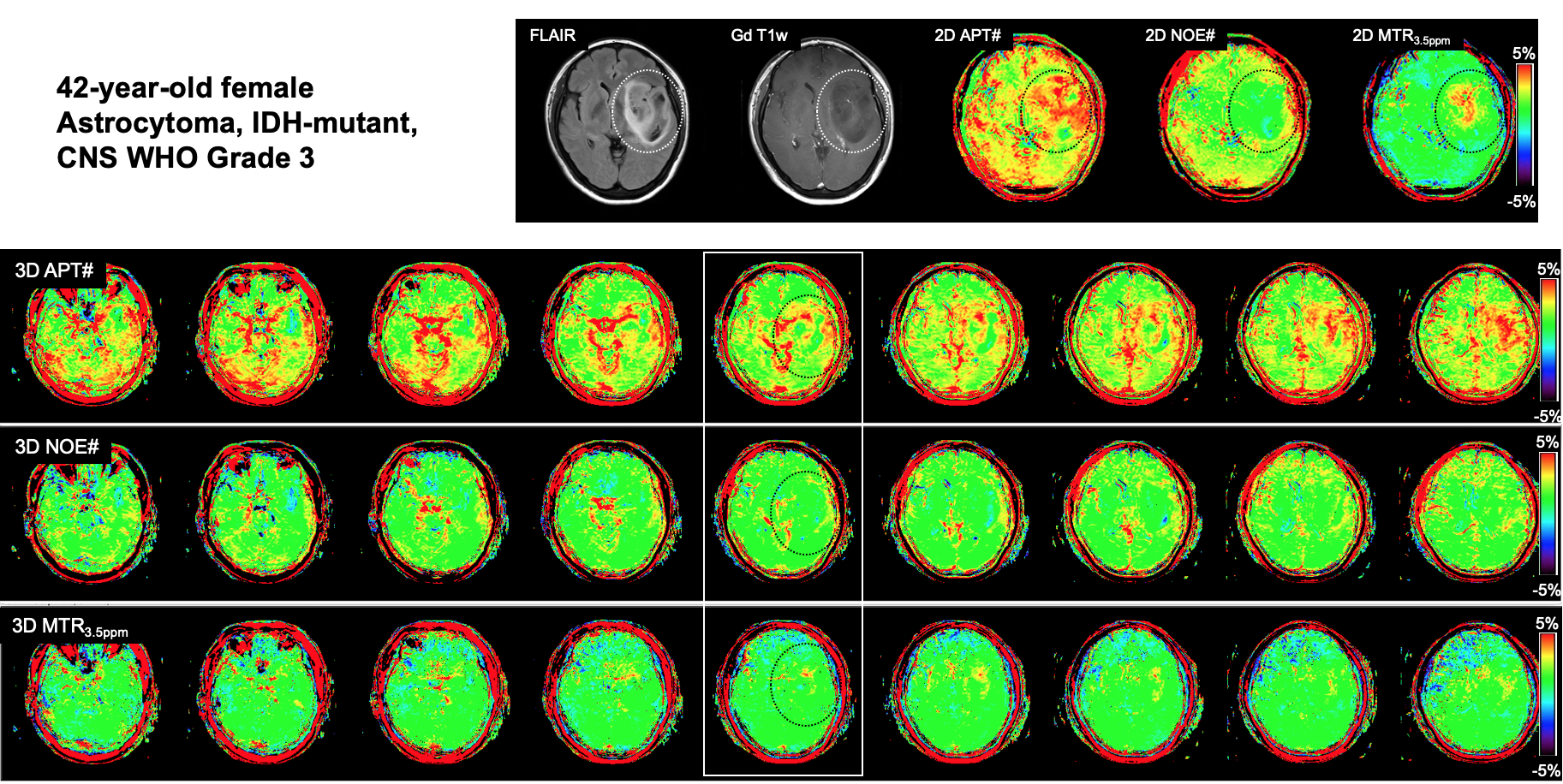
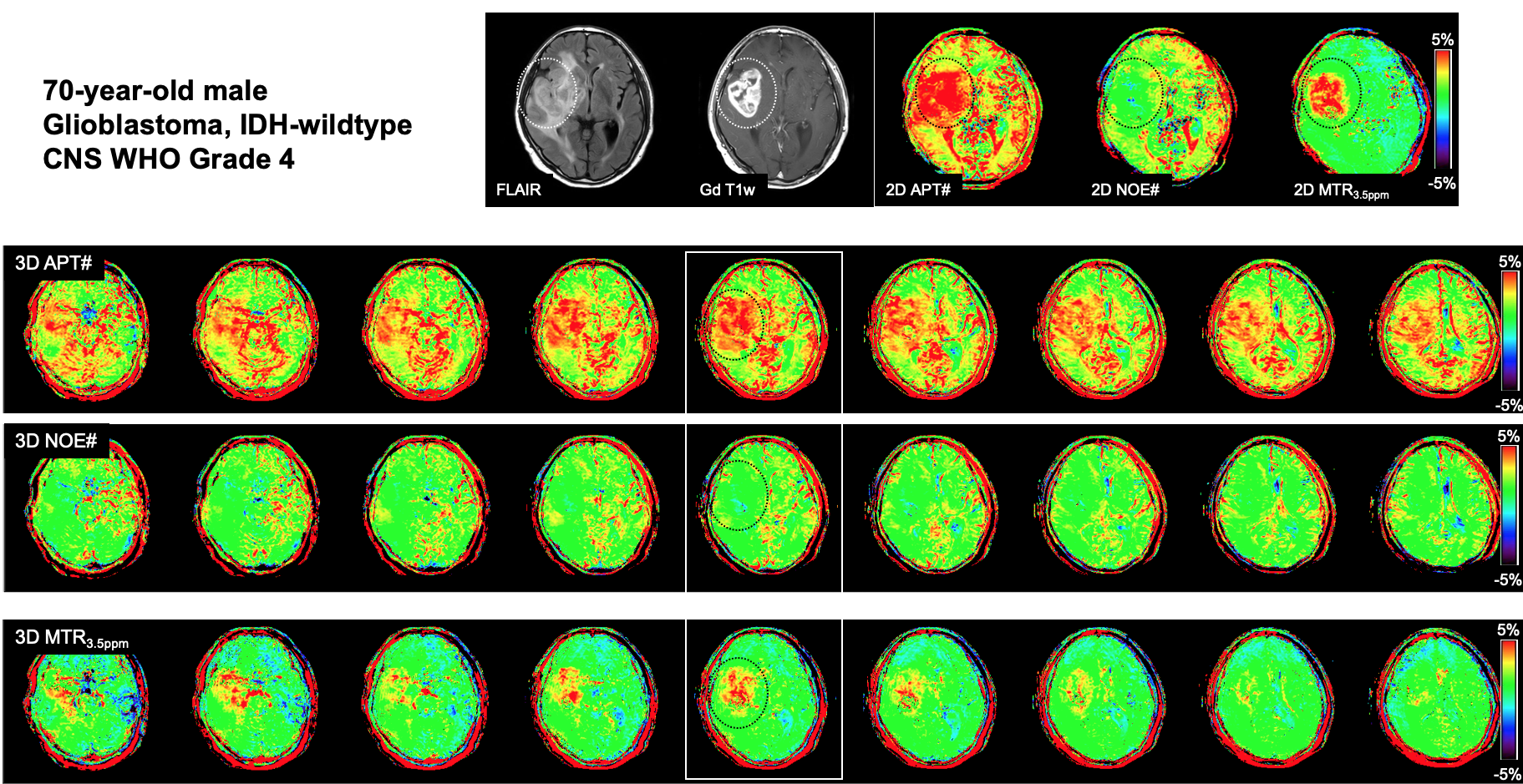
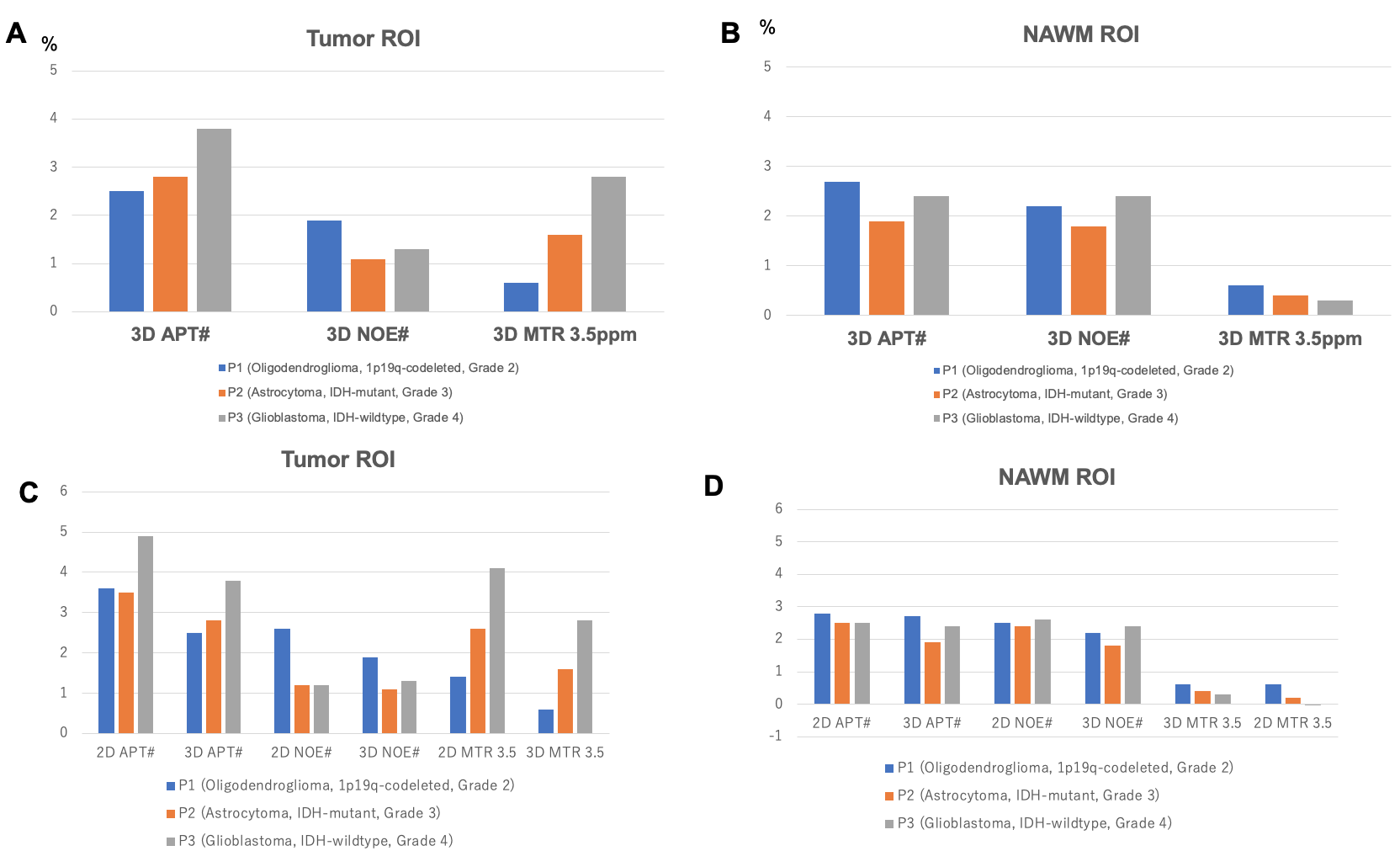
In all patients (Figure 2, 3 and 4), 3D mapping of APT#, NOE#, and MTRasym at 3.5ppm was feasible on all slices with no notable fitting errors. On visual inspection, there is almost no contrast in APT# and MTRasym at 3.5ppm between tumor and NAWM in the patient with an oligodendroglioma (grade 2, Figure 2). An increase in APT# and MTRasym at 3.5ppm was observed in the astrocytoma (grade 3, Figure 3) and glioblastoma (grade 4, Figure 4) cases. No differences in NOE# between tumor and NAWM are observed in any patient. Figure 5 shows the quantitative measurements of APT#, NOE# and MTRasym at 3.5ppm in tumor and NAWM ROIs. The highest APT# and MTRasym at 3.5ppm in tumor ROIs were observed in the glioblastoma (grade 2), while the lowest APT# and MTRasym at 3.5ppm were observed in the oligodendroglioma (grade 4). NOE# in oligodendroglioma was higher than in the other two higher grade gliomas. In comparison with the 2D imaging, APT# and MTRasym at 3.5ppm measured with the 3D imaging tended to be lower, while no major differences were observed for NAWM.Discussion
Considering the heterogeneity within the tumor, single-slice imaging is not able to evaluate the whole tumor. Our proposed 3D CEST imaging with CS-SENSE for EMR fitting enables to obtain volumetric APT# and NOE# imaging to cover an entire tumor.Conclusion
The 3D CEST imaging combined with CS-SENSE for EMR fitting in patients with brain tumors was feasible. This scheme allows multi-slice mapping of APT# and NOE#. Quantitative assessment of these values in gliomas may provide useful information on tumor aggressiveness or patient prognosis, which should be evaluated in a large patient study in the future.Acknowledgements
No acknowledgement found.References
1. Togao O, Yoshiura T, Keupp J, et al. Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades. Neuro Oncol 2014;16:441-4482.
2. Heo HY, Zhang Y, Jiang S, et al. Quantitative assessment of amide proton transfer (APT) and nuclear overhauser enhancement (NOE) imaging with extrapolated semisolid magnetization transfer reference (EMR) signals: II. Comparison of three EMR models and application to human brain glioma at 3 Tesla. Magn Reson Med 2016;75:1630-16393.
3. Heo HY, Zhang Y, Burton TM, et al. Improving the detection sensitivity of pH-weighted amide proton transfer MRI in acute stroke patients using extrapolated semisolid magnetization transfer reference signals. Magn Reson Med 2017;78:871-8804.
4. Wada T, Tokunaga C, Togao O, et al. Three-dimensional chemical exchange saturation transfer imaging using compressed SENSE for full z-spectrum acquisition. Magn Reson Imaging 2022;92:58-665.
5. Keupp J, Togao O. Assessment of Amide Proton Transfer and Nuclear Overhauser Effects Using Long RF Saturation at 3T in Clinical Brain Tumor Applications. Proc Int Soc Magn Reson Med 2015;23:1001
Figures