0357
Deep learning radiomic nomogram can distinguish intracranial solitary fibrous tumor from angiomatous meningioma: a multicenter study1Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Lanzhou University Second Hospital, Lanzhou, China
Synopsis
Keywords: Tumors (Pre-Treatment), Machine Learning/Artificial Intelligence
Motivation: A novel and noninvasive method for distinguishing intracranial solitary fibrous tumor (ISFT) from angiomatous meningioma (AM) and predicting patient outcomes is urgent.
Goal(s): To evaluate the value of a MRI-based deep learning radiomic nomogram (DLRN) in distinguishing ISFT from AM and predicting patient outcomes.
Approach: A MRI-based DLRN was developed on training cohort (TC). We then validated it's performance on external validation cohort (EVC). Moreover, we investigated the value of the DLRN in survival analysis.
Results: The performance of DLRN was excellent (0.86 [0.84–0.88]) on EVC. Besides, DLRN was significantly associated with the overall survival (OS) of patients (n=273).
Impact: The proposed DLRN can potentially provide a noninvasive method for neurosurgeon to offer decision support for developing personalized treatment plans and predicting patient outcomes.
Introduction
Intracranial solitary fibrous tumor (ISFT) and angiomatous meningioma (AM) have significant differences in biological behavior, surgical plan (such as operate as soon as possible to get gross total resection and preoperative tumor vascular embolization for ISFT patients) and patient prognosis. However, it may be difficult to distinguish them using conventional imaging diagnosis methods due to the similar imaging manifestations.Methods
A total of 1090 patients (including 449 patients with ISFT and 641 patients with AM) from Beijing Tiantan Hospital, Capital Medical University and 131 patients (including 50 patients with ISFT and 81 patients with AM) from Lanzhou University Second Hospital were used as primary cohort (PC) and external validation cohort (EVC), respectively. The patients from PC were divided into training cohort (TC) and internal validation cohort (IVC) at a ratio of 7:3. A DLRN was developed based on MRI on the TC for preoperatively distinguishing ISFT from AM. We then tested the DLRN on the IVC and EVC and compared it with the clinical model (CM). Moreover, we investigated the value of the DLRN in survival analysis.Results
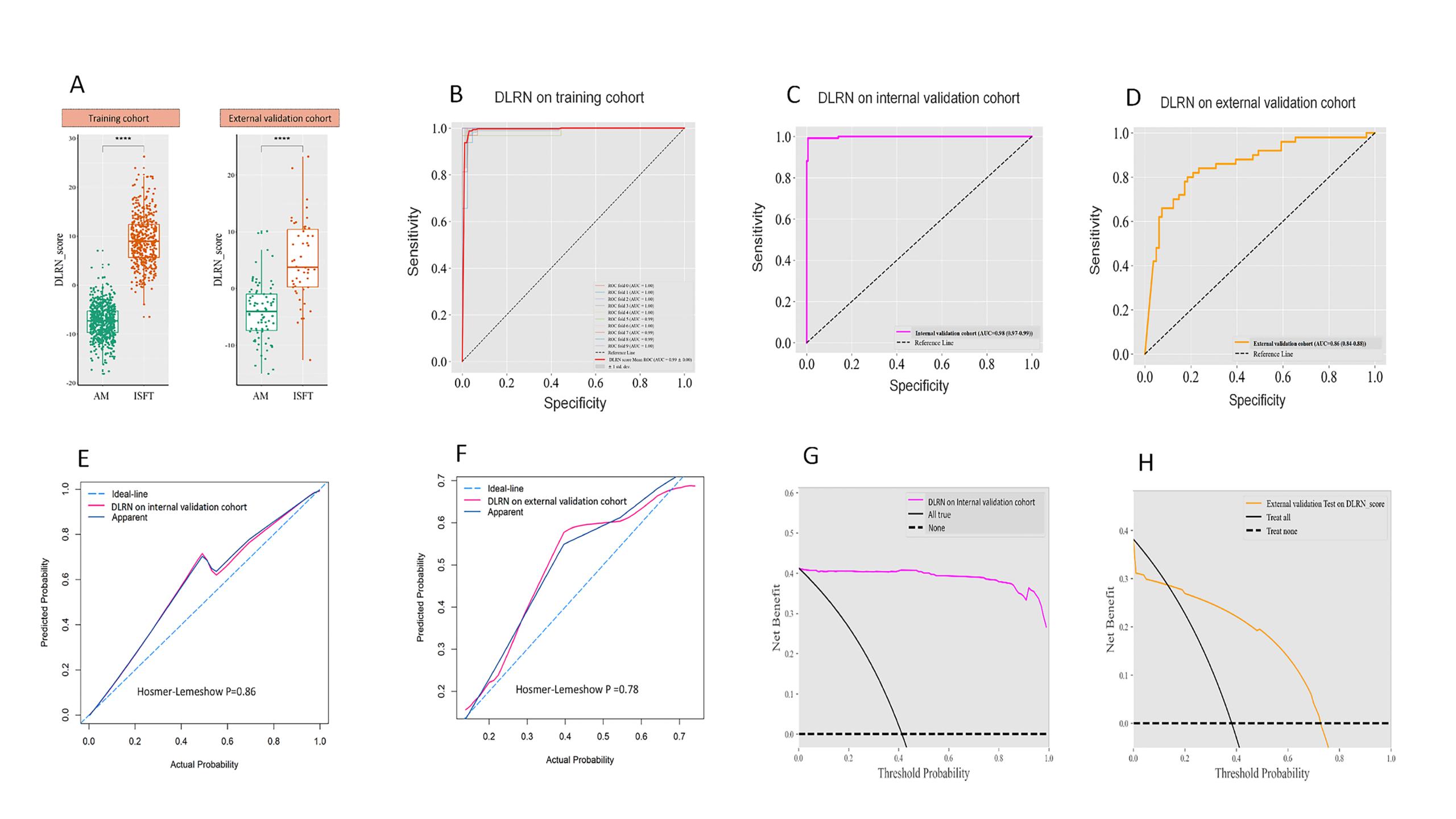
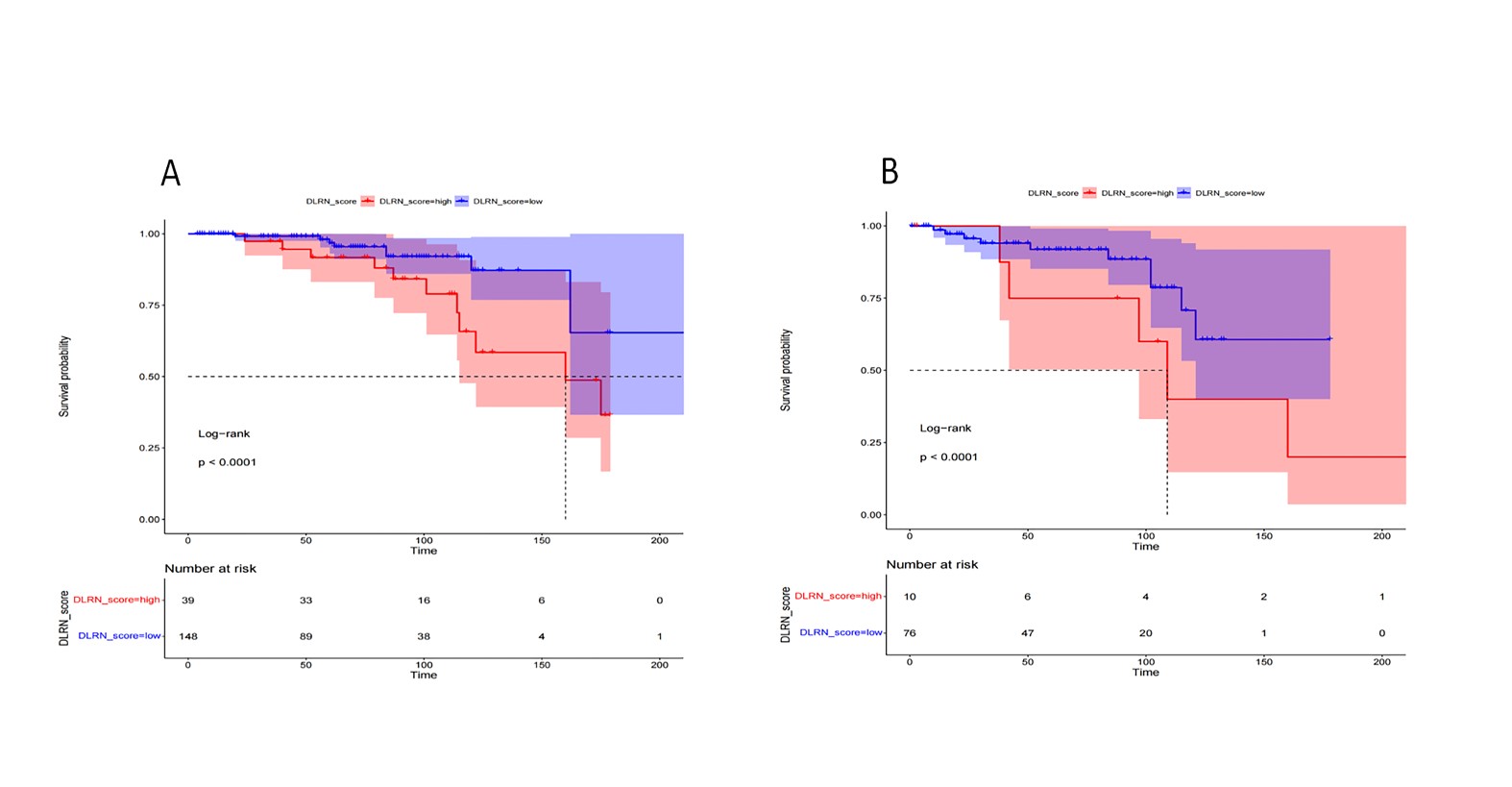
The performance of DLRN on the TC was excellent and stable. The DLRN performed significantly better than the routinely used CM (AUC (95% confidence interval, CI): 0.86 [0.84–0.88] for DLRN and 0.70 [0.67–0.72] for CM, P<0.001) on the EVC. Besides, DLRN was significantly associated with the overall survival (OS) of patients (n=273).Discussion
The proposed DLRN performed good performance than CM in our study. We speculate that this may be due to the addition of radiomic signature (including deep learning and hand-crafted features) to DLRN, which can more fully reflect the characteristics of the tumor that can not seen by the naked eyes. Two of nine selected features in the three signatures were DL features, indicating that the Deep Convolutional Neural Network (DCNNs) could extract correlative quantitative representation reflecting the different tumors. Besides, the global texture features were also adopted in the radiomic signatures (including GLCM, GLRLM and GLSZM), which might reflect the heterogeneity of the tumor.A previous study has reported that machine-learning model based on fusion features can distinguish ISFT from AM in the internal test (0.950) (1). Dong et al. (2) showed that the combined sequence model (AUC: 0.939) showed the best performance, followed by the T2WI model (AUC: 0.864), T1WI model (AUC: 0.830), and T1WI CE model (AUC: 0.772). Li et al. (3) showed that the enhanced T1WI-based classifier have the best performance (AUC: 0.90), followed by T2-FLAIR-based and DWI-based classifiers (AUC: 0.77 and 0.73). Fan et al. (4) showed that a fusion radiomic model (AUC: 0.900) and clini-radiomic model (AUC: 0.910) both can perform the differential diagnosis of ISFT and AM. All these results indicated that the machine learning model have an important role in distinguishing ISFT from AM. The performance of our proposed DLRN perform better than the above four studies on the IVC (the AUC of our DLRN was 0.980), which may have something to do with the fact that we are adding deep learning features to the model. In addition, our DLRN model also have good performance on EVC (AUC: 0.860), which demonstrated that it is of great value in distinguishing ISFT from AM.
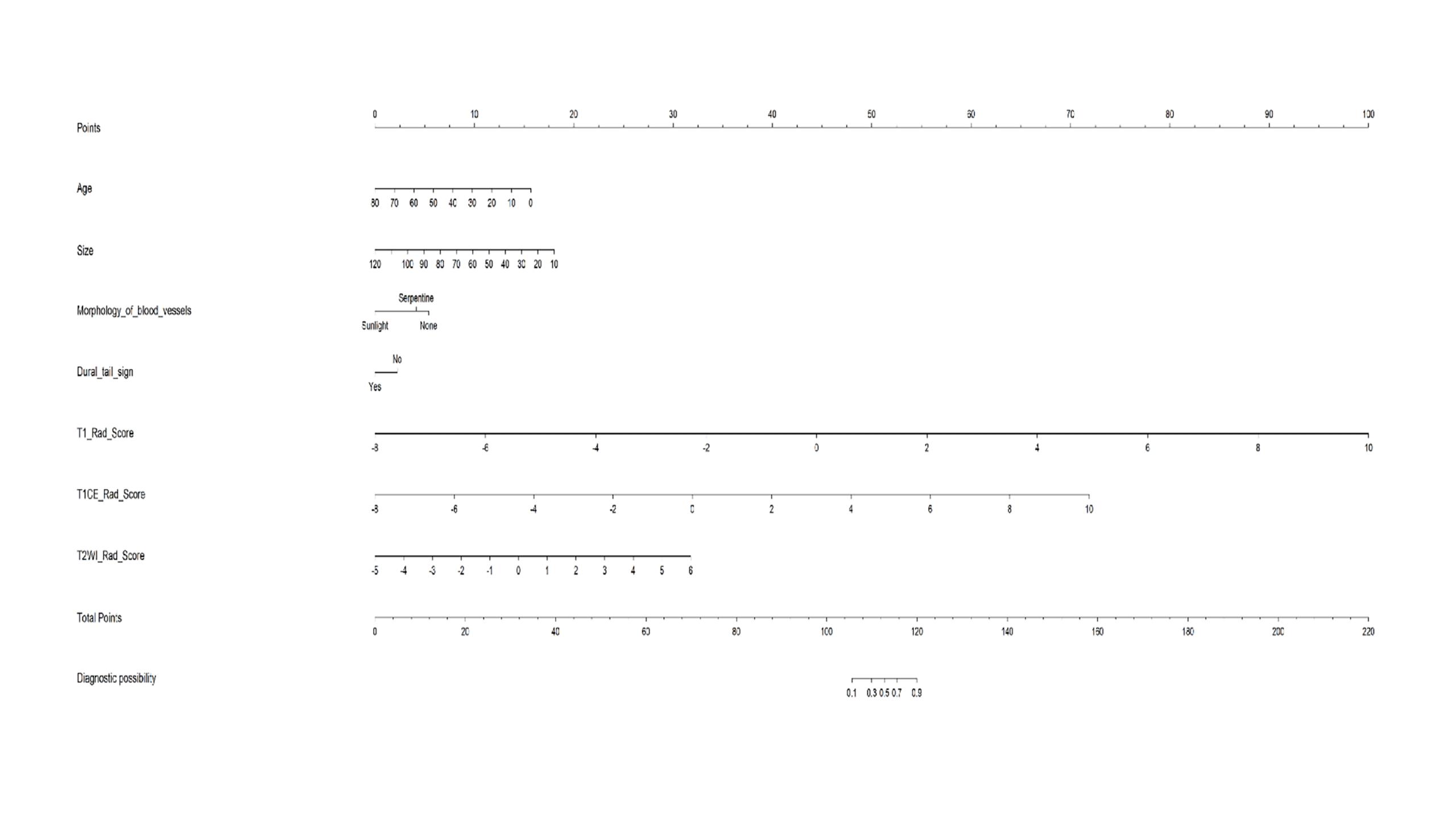
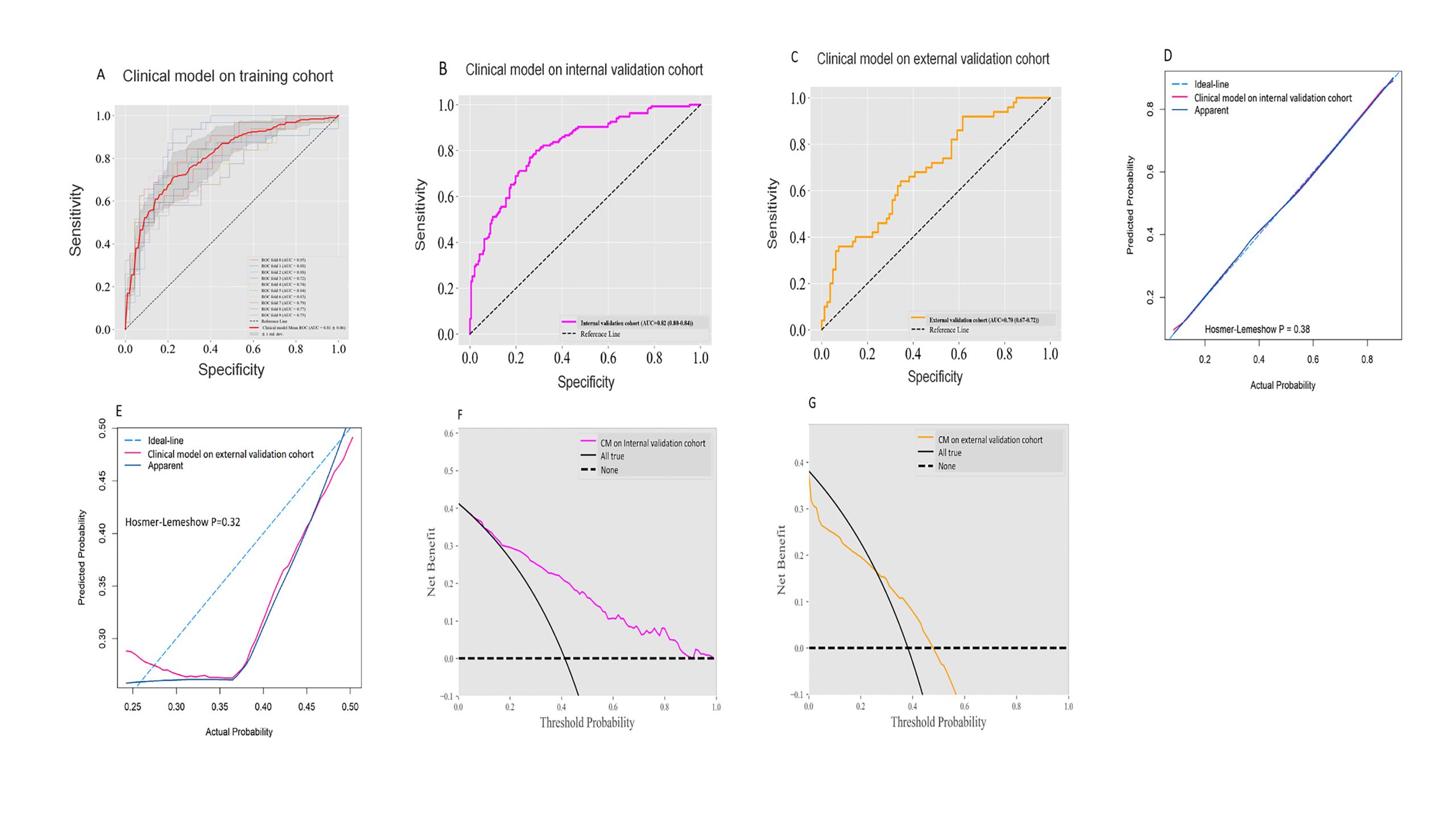
In our study, we incorporated 4 clinical characteristics (including age, size, morphology of tumor blood vessel and dural tail sign ) in our CM, and our model had good performance on the IVC (AUC: 0.820), which is similar to previous study (1). However, our model does not perform well on EVC (AUC: 0.70). Although some studies have demonstrated that some clinical features have certain value in distinguishing ISFT from AM, no model has been established (5–8). Compared with CM, DLRN significantly improved the diagnostic performance, which confirmed the contribution of radiomics to the model.
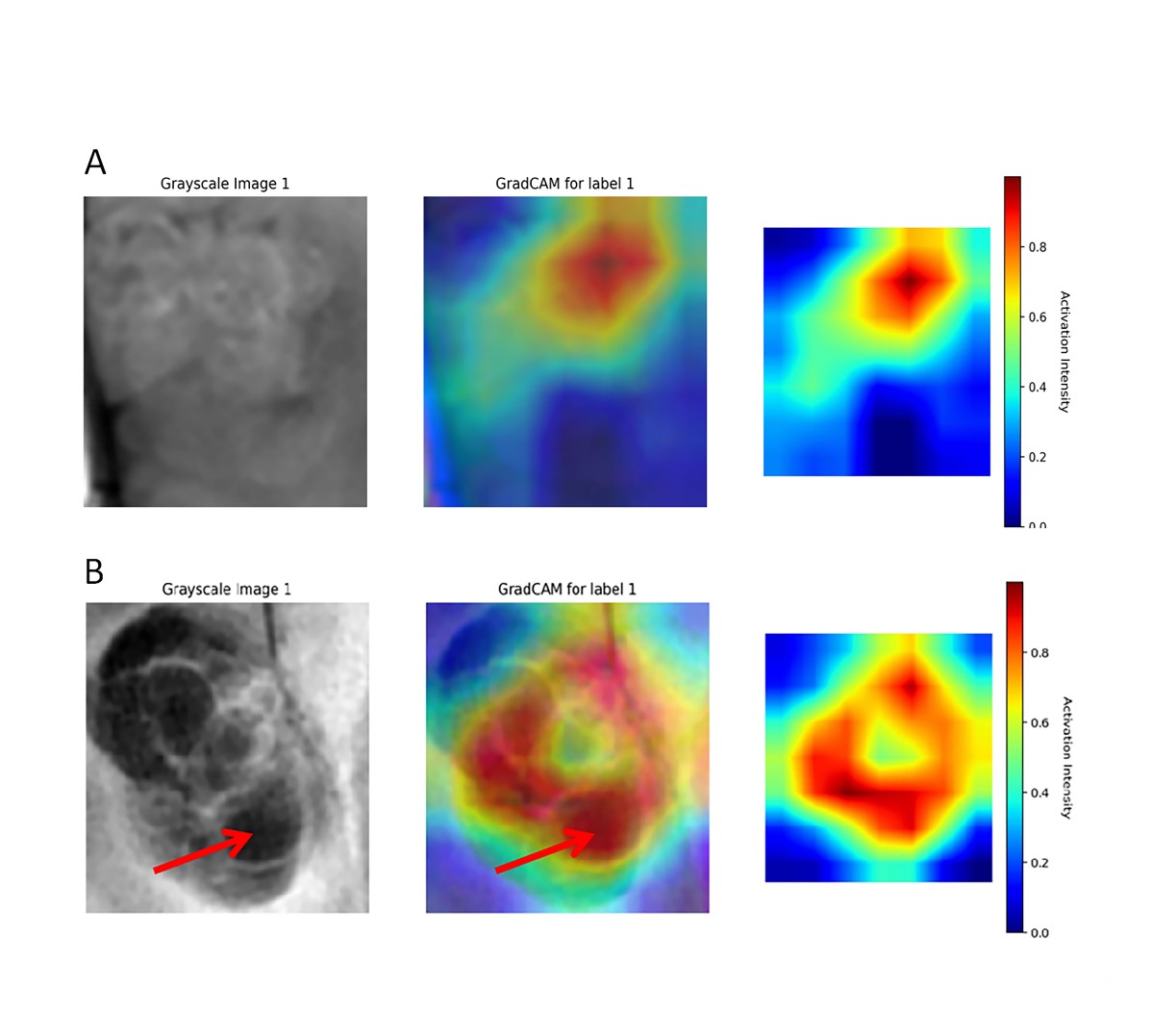
Another finding was that our DLRN was significantly associated with the OS of patients. There was a significant positive correlation between DLRN score and tumors. Our results also show that the DLRN score of ISFT was higher than that of AM, as shown in Figure 2A. Patients with high DLRN score displayed worse OS in both GTR group and STR group. All these results confirm our hypothesis. Thus, DLRN can determine the prognosis for patients. We suspect that the more highlighted regions in the activation maps may be relevant to worse prognosis, as shown in Figure 5.
Conclusion
The proposed MRI-based DRNL could be used as a powerful approach for distinguishing ISFT from AM and predicting patient outcomes.Acknowledgements
This work was supported by the The National Natural Science Foundation of China (Grant number: 82071872, 82371914), The Science and Technology Program of Gansu Province (Grant number: 21YF5FA123, 21JR11RA105), The China International Medical Foundation (Grant number: Z-2014-07-2101). We would also like to express our special thanks of gratitude to Dr. Xiping Shen for his statistical advice.References
1. Kong X, Luo Y, Li Y, et al. Preoperative prediction and histological stratification of intracranial solitary fibrous tumours by machine-learning models. Clin Radiol. 2023; 78(3):e204–e213.
2. Dong J, Yu M, Miao Y, et al. Differential Diagnosis of Solitary Fibrous Tumor/Hemangiopericytoma and Angiomatous Meningioma Using Three-Dimensional Magnetic Resonance Imaging Texture Feature Model. Biomed Res Int. 2020.
3. Li X, Lu Y, Xiong J, et al. Presurgical differentiation between malignant haemangiopericytoma and angiomatous meningioma by a radiomics approach based on texture analysis. J Neuroradiol. 2019; 46 (5): 281–287.
4. Fan Y, Liu P, Li Y, et al. Non-Invasive Preoperative Imaging Differential Diagnosis of Intracranial Hemangiopericytoma and Angiomatous Meningioma: A Novel Developed and Validated Multiparametric MRI-Based Clini-Radiomic Model. Front Oncol. 2022.
5. Wang C, Xu Y, Xiao X, et al. Role of intratumoral flow void signs in the differential diagnosis of intracranial solitary fibrous tumors and meningiomas. J Neuroradiol. 2016; 43 (5):325–30.
6. Meng Y, Chaohu W, Yi L, et al. Preoperative radiologic characters to predict hemangiopericytoma from angiomatous meningioma. Clin Neurol Neurosurg. 2015;138: 78–82.
7. He L, Li B, Song X, et al. Signal value difference between white matter and tumor parenchyma in T1- and T2- weighted images may help differentiating solitary fibrous tumor/hemangiopericytoma and angiomatous meningioma. Clin Neurol Neurosurg. 2020.
8. Chen C, Ren CP. Value of Apparent Diffusion Coefficient (ADC) and Dynamic Contrast-Enhanced Magnetic Resonance Imaging (DCE-MRI) in Differentially Diagnosing Angiomatous Meningiomas and Solitary Fibrous Tumors/Hemangiopericytomas. Med Sci Monit. 2019; 11 (25): 5992–5996.
Figures