0345
Model-Assisted Deep Learning-Based Reconstruction of Accelerated Golden-Angle Radial Data for Free-Breathing Dynamic Contrast-Enhanced MRI1Siemens Healthineers, Princeton, NJ, United States, 2Siemens Healthineers AG, Erlangen, Germany, 3Siemens Industry Software România, Brasov, Romania, 4Department of Radiology, University Hospital Basel, University of Basel, Basel, Swaziland
Synopsis
Keywords: AI/ML Image Reconstruction, Image Reconstruction
Motivation: GRASP allows for free-breathing DCE-MRI with high spatial and temporal resolution. However, the current 4D iterative reconstruction is slow and still suffers from streaking artifacts, limiting clinical use.
Goal(s): Develop a DL solution that significantly reduces the reconstruction time and improves image quality.
Approach: A model-assisted DL reconstruction combining a sparsity model with an efficient 3D spatiotemporal network for fast and robust reconstruction of accelerated scans with high resolution.
Results: A sparsity-constrained DL-based can provide robust and fast reconstructions with improved image quality, evidenced by the superior quantitative metrics and the qualitative analysis of cases under-represented in the training data.
Impact: GRASP offers high-resolution 4D free-breathing DCE-MRI; however, it still suffers from under-sampling artifacts and long reconstruction times. A model-assisted DL reconstruction can reduce the reconstruction time, improve image quality, and increase system robustness—essential in translating to clinical practice.
Introduction
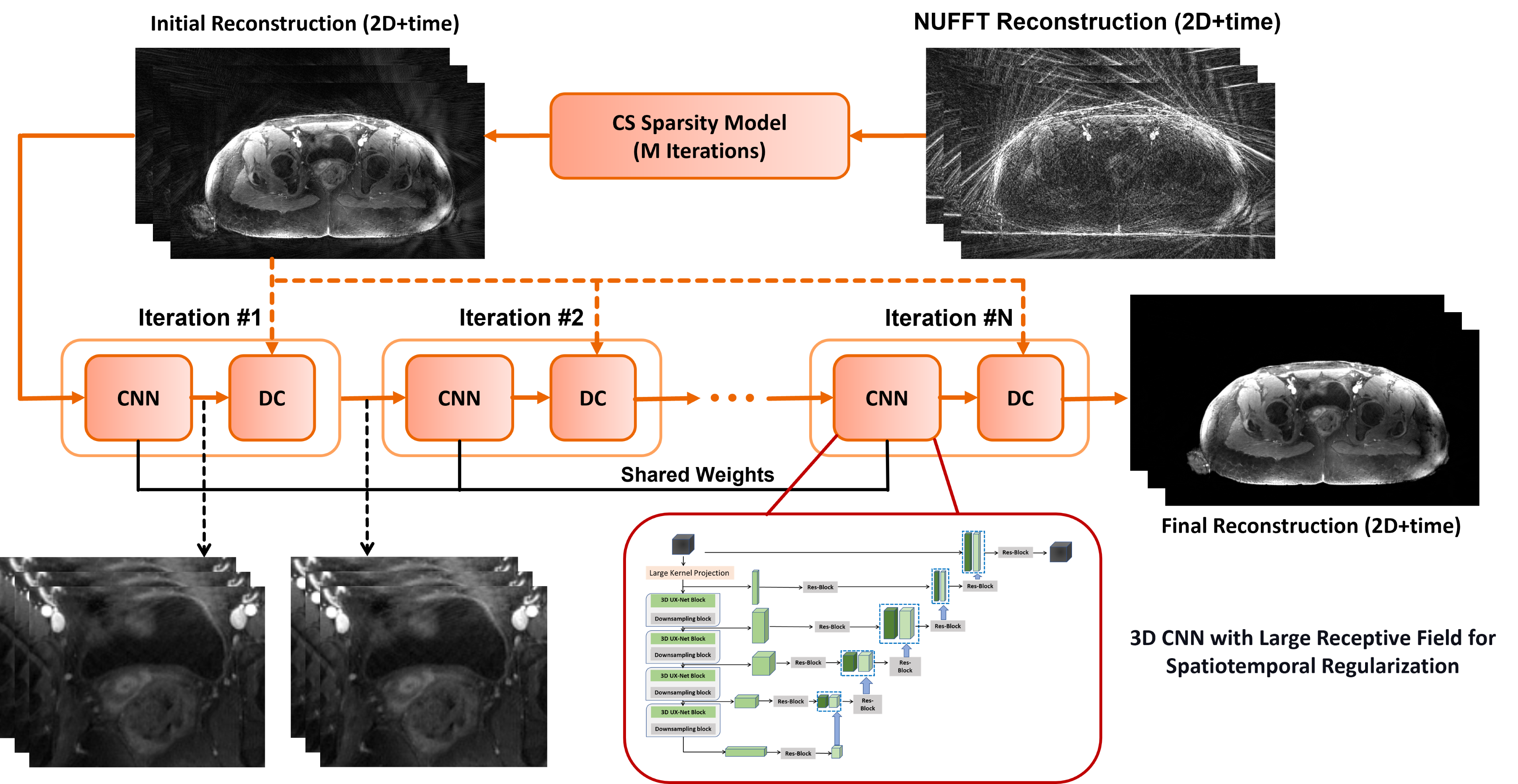
GRASP is a novel technique where a golden-angle radial VIBE sequence is combined with temporal compressed sensing (CS) to allow for free-breathing dynamic contrast-enhanced (DCE)-MRI with high spatial and temporal resolution [1,2]. However, 4D GRASP reconstruction is performed with an iterative algorithm, resulting in long reconstruction times limiting clinical use. Moreover, at higher accelerations and increased resolutions, reconstructions still suffer from increased under-sampling (streaking) artifacts. Deep learning (DL) techniques were proposed to tackle such problems [3]; however, they operate entirely in the image domain and do not use data consistency (DC), increasing the hallucination risk due to poor generalization [4]. We propose a model-assisted DL solution for GRASP reconstruction combining a classical sparsity model to constrain an efficient 3D spatiotemporal network for fast reconstruction of accelerated scans with high resolution and improved generalization capability.Methods
We propose a model-assisted DL-based reconstruction for accelerated GRASP DCE-MRI scans. For such an ill-posed problem with a limited amount of training data, there is a need to avoid DL methods' sensitivity to data perturbations and poor generalization [5]. We emphasize the role of the model in providing a priori information/constraints to DL components. As shown in Figure 1, starting from a nonuniform FFT (NUFFT)-reconstruction of the under-sampled time-resolved images, a CS iterative reconstruction procedure is performed (few iterations M) with a sparsity enforced by applying undecimated Haar wavelet constraints. Optimization is performed with the FISTA algorithm [6], with a high-pass filter preconditioner applied to the gradients to improve convergence speed. The CS sparsity model is then used to initialize/constrain a plug-and-play efficient and flexible DL reconstruction.The proposed DL reconstruction relies upon an N iterations of computationally light CNN and a subsequent DC that can be applied only at test time or jointly trained end-to-end. Recent 3D medical vision transformers achieve state-of-the-art performances on several 3D volumetric data benchmarks [7], driven by the large receptive field for non-local self-attention and the large number of model parameters. However, adopting such methods for the spatiotemporal CNN block would be impractical because of long inference times. Hence, we propose a lightweight 3D CNN with large kernel depth-wise convolution (3D LK CNN) to simulate hierarchical transformer behavior while also using pointwise depth-wise feature scaling to control the model parameters. The DC layers are implemented as a finite number of iterations of the conjugate gradient (CG) method [8], solving the given system:
$$Hx=b$$ $$H= A^H A+ λI$$ $$b= A^H Dy+ λx_{prior}$$
Where $$$A^H$$$ and $$$A$$$ operators incorporate computationally expensive NUFFT operations, the density compensation function $$$D$$$ is optionally used for preconditioning the linear system to be solved. The regularization parameter $$$λ$$$ can also be trainable (with strictly positive constraints) for a better tradeoff between the CNN and DC layers.
Materials and Experimental Setting
Free-breathing 3D abdominal and brain imaging was performed on seventeen cancer patients with contrast injection on 1.5T and 3T scanners with standard golden-angle stack-of-stars radial scheme pulse sequence (8,692 2D+time slices for training, 720 2D+time slices for testing). The ground truth (target) data were generated by performing temporally slow CS iterative reconstruction till convergence (~70 iterations) on time-resolved data (55 spokes/time-point after sorting the continuously acquired data along with coil compression to 8 virtual coils). Retrospective under-sampling was performed to 21 spokes/time-point (acceleration factor of 2.6). The CNN networks were trained using complex-L1 loss with M randomly set to improve generalizability. The proposed 3D LK CNN is compared to a standard 3D UNET developed for similar applications [4]. The importance of incorporating classical signal models is highlighted by comparing them against models initialized using NUFFT reconstructions [3].Results
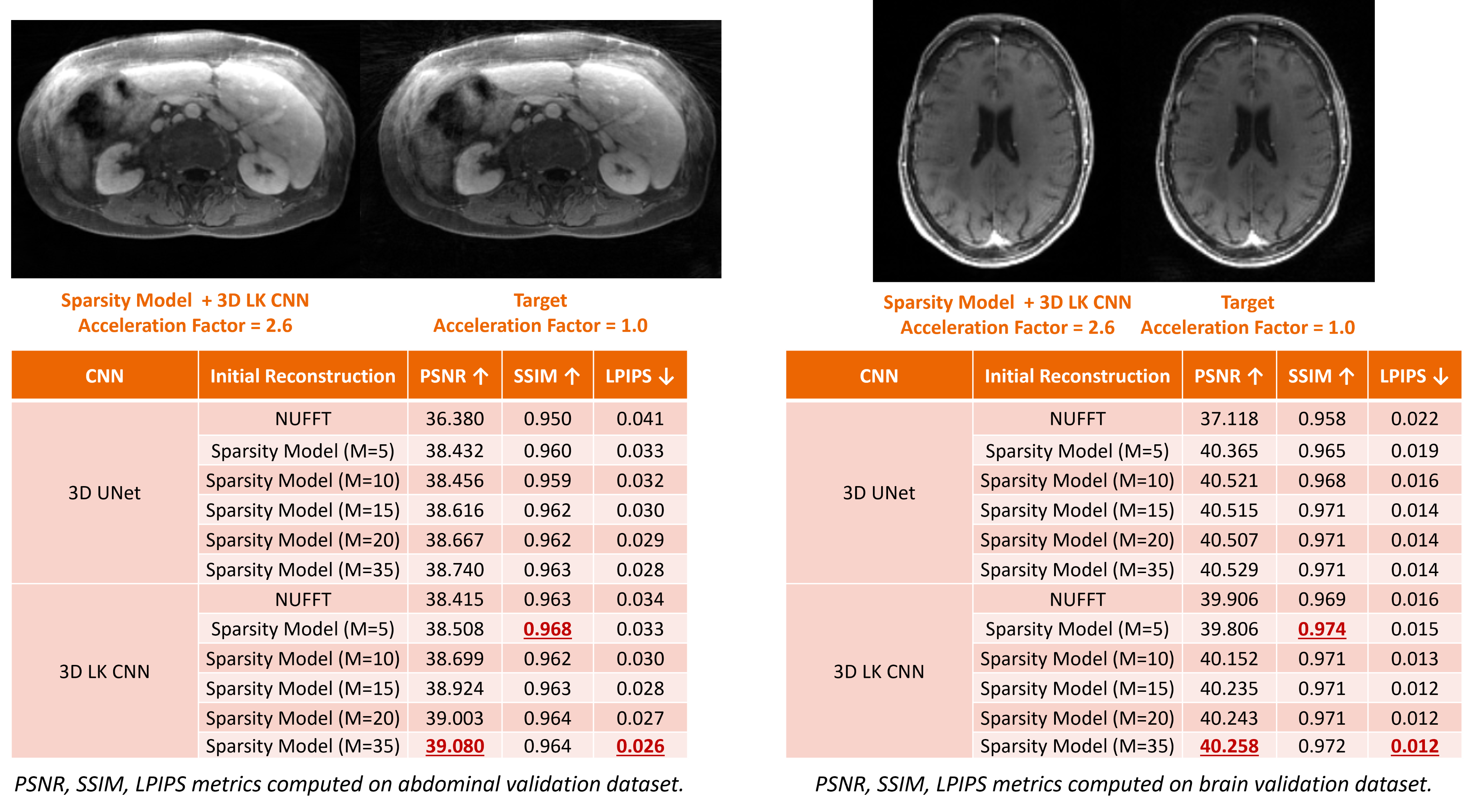
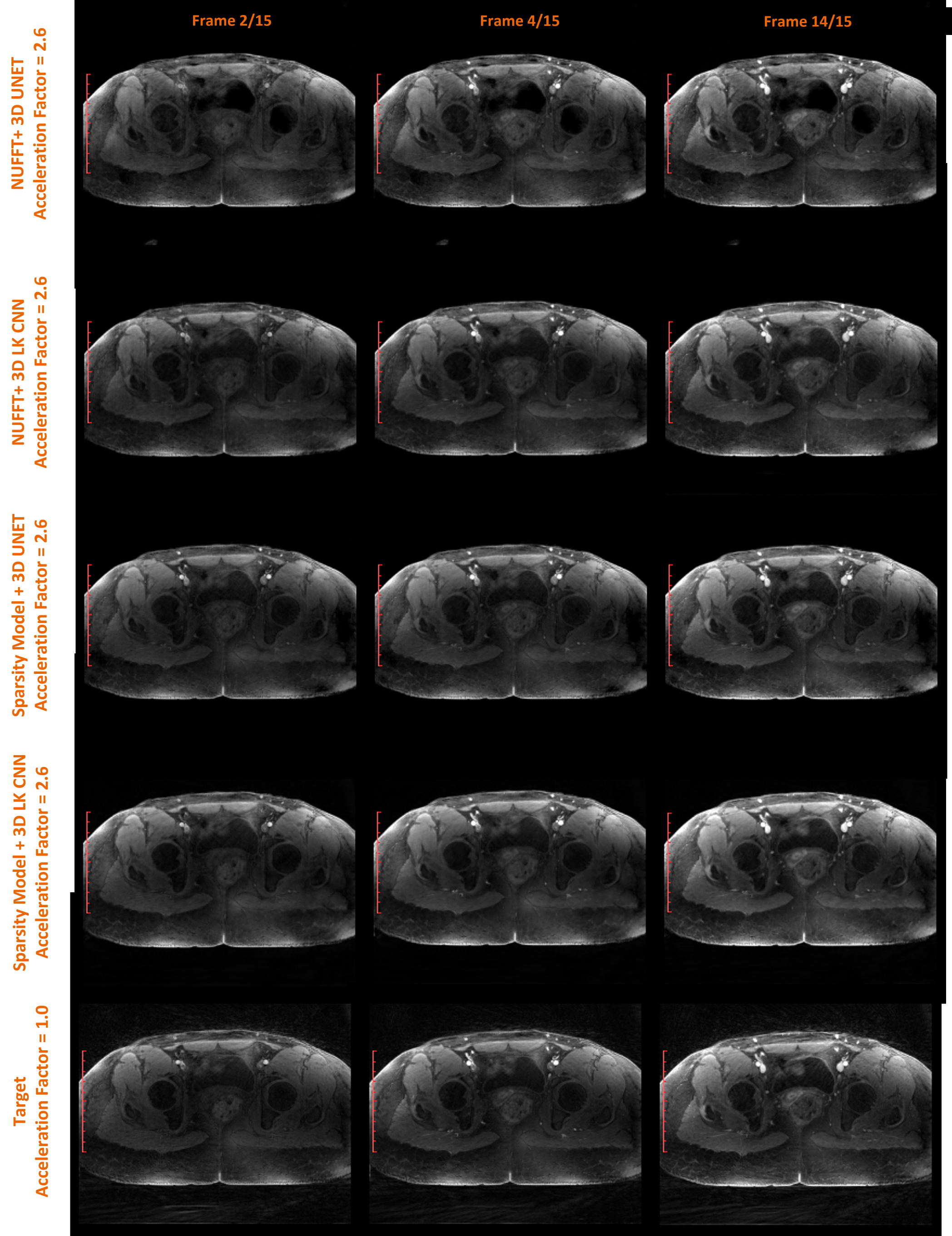
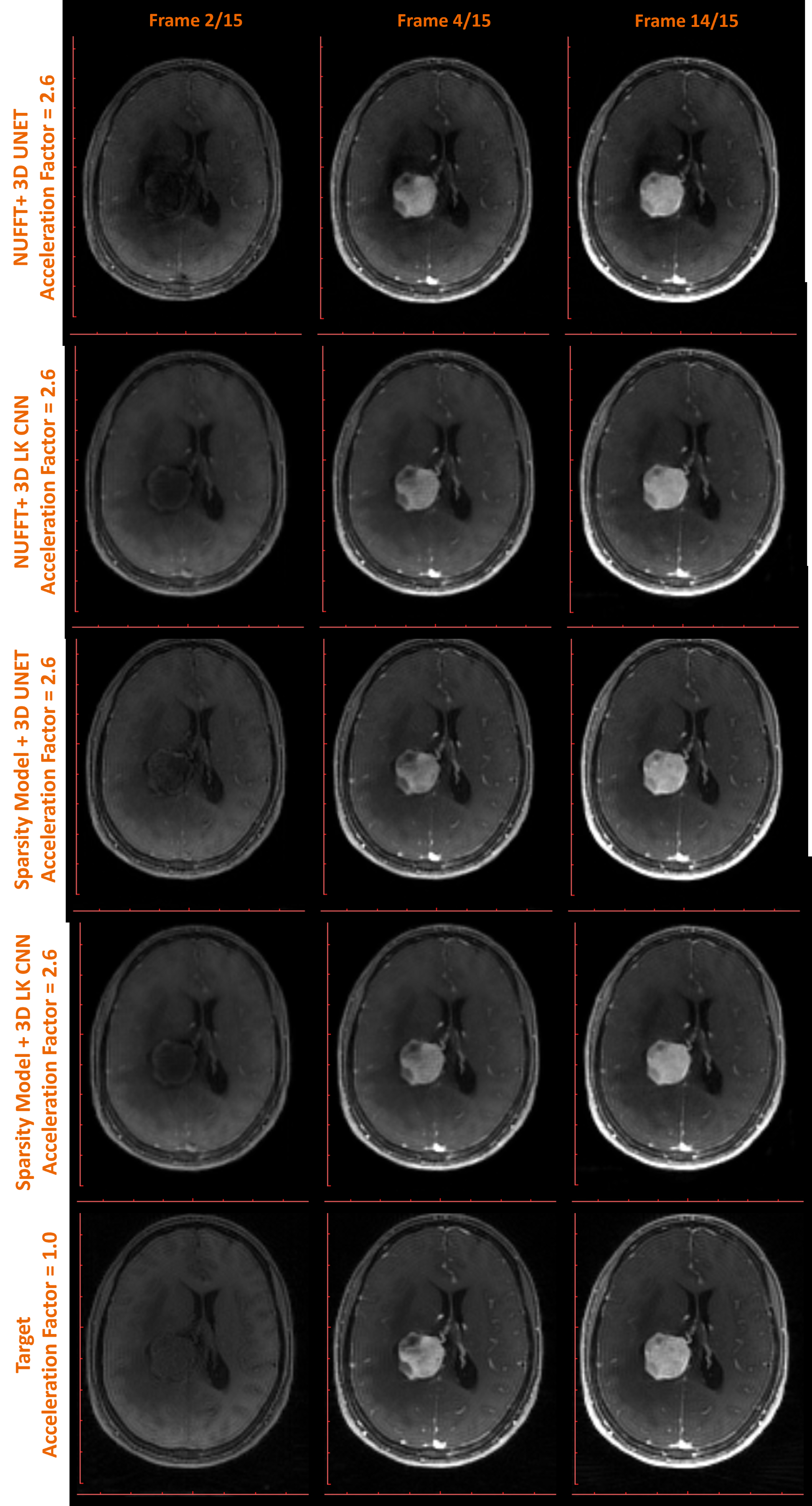
A quantitative assessment of the proposed model-assisted DL-based reconstruction using PSNR, SSIM, and LPIPS [9] metrics is provided in Figure 2. Model-assisted networks utilizing 3D LK CNN outperform competing methods, including those initialized using NUFFT reconstructions and model-assisted networks using the 3D classical 3D UNET. Similar results were obtained through qualitative visual inspection of challenging cases, as shown in Figure 3 (abdominal lesion) and Figure 4 (brain tumor). Figure 5 shows the contrast dynamics of accelerated DCE-MRI scans in selected ROIs (aorta and femoral artery) with the proposed methods (sparsity Model+3D LK CNN), providing the lowest MAE compared to the target.Conclusion
A model-assisted DL-based reconstruction can accelerate GRASP DCE-MRI scans, reduce reconstruction time, and improve image quality. Integrating classical signal models with DL for image reconstruction is necessary to ensure system robustness and generalization capability for translation to clinical practice.Disclaimer
The concepts and information presented in this abstract are based on research results that are not commercially available. Future commercial availability cannot be guaranteed.Acknowledgements
No acknowledgement found.References
[1] Block, Kai Tobias, et al. "GRASP: Tackling the challenges of abdominopelvic DCE-MRI." Magnetom Flash 5 (2014): 16-22.
[2] Feng, Li, et al. "Golden‐angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden‐angle radial sampling for fast and flexible dynamic volumetric MRI." Magnetic resonance in medicine 72.3 (2014): 707-717.
[3] Jafari, Ramin, et al. "GRASPNET: Fast spatiotemporal deep learning reconstruction of golden‐angle radial data for free‐breathing dynamic contrast‐enhanced magnetic resonance imaging." NMR in Biomedicine 36.3 (2023): e4861.
[4] Kofler, Andreas, et al. "An end‐to‐end‐trainable iterative network architecture for accelerated radial multi‐coil 2D cine MR image reconstruction." Medical Physics 48.5 (2021): 2412-2425.
[5] Guan, Yue, et al. "Subspace Model-Assisted Deep Learning for Improved Image Reconstruction." IEEE Transactions on Medical Imaging (2023).
[6] Beck, Amir, and Marc Teboulle. "A fast iterative shrinkage-thresholding algorithm for linear inverse problems." SIAM journal on imaging sciences 2.1 (2009): 183-202.
[7] He, Yufan, et al. "SwinUNETR-V2: Stronger Swin Transformers with Stagewise Convolutions for 3D Medical Image Segmentation." International Conference on Medical Image Computing and Computer-Assisted Intervention. Cham: Springer Nature Switzerland, 2023.
[8] Hestenes, Magnus R., and Eduard Stiefel. "Methods of conjugate gradients for solving linear systems." Journal of research of the National Bureau of Standards 49.6 (1952): 409-436.
[9] Zhang, Richard, et al. "The unreasonable effectiveness of deep features as a perceptual metric." Proceedings of the IEEE conference on computer vision and pattern recognition. 2018.
Figures