0310
Multiparametric imaging of dopaminergic, cholinergic and noradrenergic contribution in olfactory dysfunction in Parkinson’s disease1Paris Brain Institute – ICM, MOVIT team, Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, Paris, France, 2Paris Brain Institute – ICM, Centre de NeuroImagerie de Recherche – CENIR, Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, Paris, France, 3Paris Brain Institute – ICM, Data Analysis Core, Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, Paris, France, 4Paris Brain Institute – ICM, Centre d'Investigation Clinique (CIC), Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, Paris, France
Synopsis
Keywords: Parkinson's Disease, Parkinson's Disease
Motivation: Olfactory dysfunction is an early symptom of Parkinson’s disease (PD), involving impairments of cholinergic, dopaminergic, and noradrenergic networks. Patients with idiopathic REM sleep behavior disorder (iRBD), a prodromal phase of PD, are associated with anosmia and severe noradrenergic defects.
Goal(s): This study aimed to decipher the contribution of cholinergic, dopaminergic, and noradrenergic alterations in olfactory impairments in the presence or absence of RBD.
Approach: Multiparametric imaging highlighted specific alterations of the Locus Coeruleus (LC) and Nucleus Basalis of Meynert that correlated with olfactory score
Results: Alterations were modulated by the presence of RBD, suggesting specific progression pattern.
Impact: Our results show that olfactory dysfunction originates from different altered subcortical nodes in Parkinson’s disease patients depending on the presence of sleep disorder. This suggests that patients with sleep disorder display different progression pattern of Parkinson’s disease.
Purpose
Olfactory dysfunction often begins before motor symptom onset1 in Parkinson’s disease (PD), and is also an early symptom in idiopathic rapid eye movement sleep behaviour disorder (iRBD), a prodromal phase of PD2. Olfactory function involves cholinergic neurons of the nucleus Basalis of Meynert (NBM)3, dopaminergic neurons of the substantia nigra (SN)4 and noradrenergic neurons of the locus coeruleus (LC)5. Particular alterations of noradrenergic neurons in RBD patients suggest that the LC could contribute differently to olfactory impairment in PD patients depending on the RBD status.This study aimed to investigate the respective contribution of cholinergic, dopaminergic, and noradrenergic alterations underlying olfactory impairment in PD and RBD. We hypothesized that olfactory impairments would be associated with (i) alterations in subcortical nodes of all three neurotransmission systems considering all patients, particularly in the cholinergic basal forebrain; (ii) greater defects in dopaminergic nodes for PD compared to iRBD patients, (iii) greater contribution of noradrenergic alterations in olfactory impairments in patients with RBD.
Methods
Population: Early PD (n=107, < 4 years post diagnosis without cognitive impairment), iRBD patients (n=35) and HC (n=39) had University of Pennsylvania Smell Identification Test, motor and cognitive assessments. Anosmia was defined by an UPSIT score<25. We sorted individuals in five groups (see demographics in Table 1): HC, iRBD, normosmic PD patients without RBD (PDRBD-/a-), anosmic PD patients without RBD (PDRBD-/a+), and PD patients with RBD (PDRBD+/a+).Neuroimaging: We acquired (i) 123I-Ioflupane dopamine transporter (DaT) signal in the striatum on hybrid gamma camera Discovery 670 Pro system; (ii) whole brain T1-weighted 3D MP2RAGE (TR/TE=5000/2.98ms, Resolution=1x1x1mm3, acquisition time=08:12min); (iii) T1-weighted 2D turbo spin echo (TR/TE=890/13ms, in-plane resolution=0.3x0.3mm2, 48 slices, slice thickness=3mm, acquisition time=6:55min)6,7 to obtain neuromelanin-sensitive MRI (NM-MRI) on the SN and LC (3T Siemens Prisma system).
Image analysis: We segmented and normalized T1 anatomical images using non-linear transformations8 and performed a voxel-based morphometry (VBM) analysis on grey matter probability maps using SPM12, considering anatomical priors with cortical and subcortical masks of the olfactory network. The cortical mask included frontal, fronto-orbital, cingulate, temporal, and parahippocampal cortices, amygdala, and insula. The subcortical mask included caudate, putamen, thalamus, hippocampus, cerebellum, LC and NBM. NM-MRI image was registered to the T1 image of each patient and the signal from SN and LC was extracted as previously described7,9.
Statistics: We tested group differences using ANOVA with Tukey’s post-hoc tests, including age as a covariate in the analyses. Multiple regression analysis on all patients tested the correlation between UPSIT and neuroimaging markers (p<0.05 corrected for multiple comparisons with family-wise error).
Results
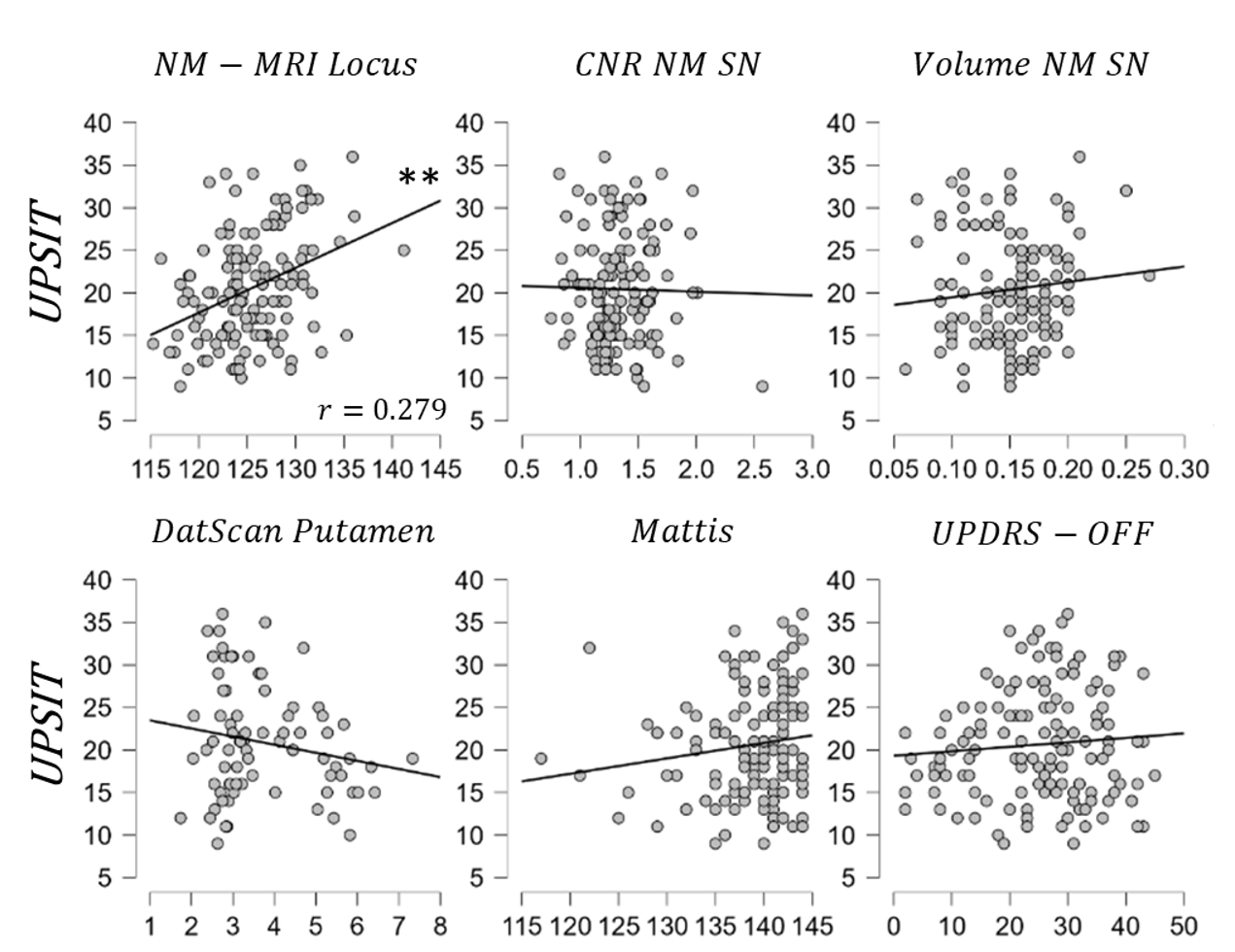
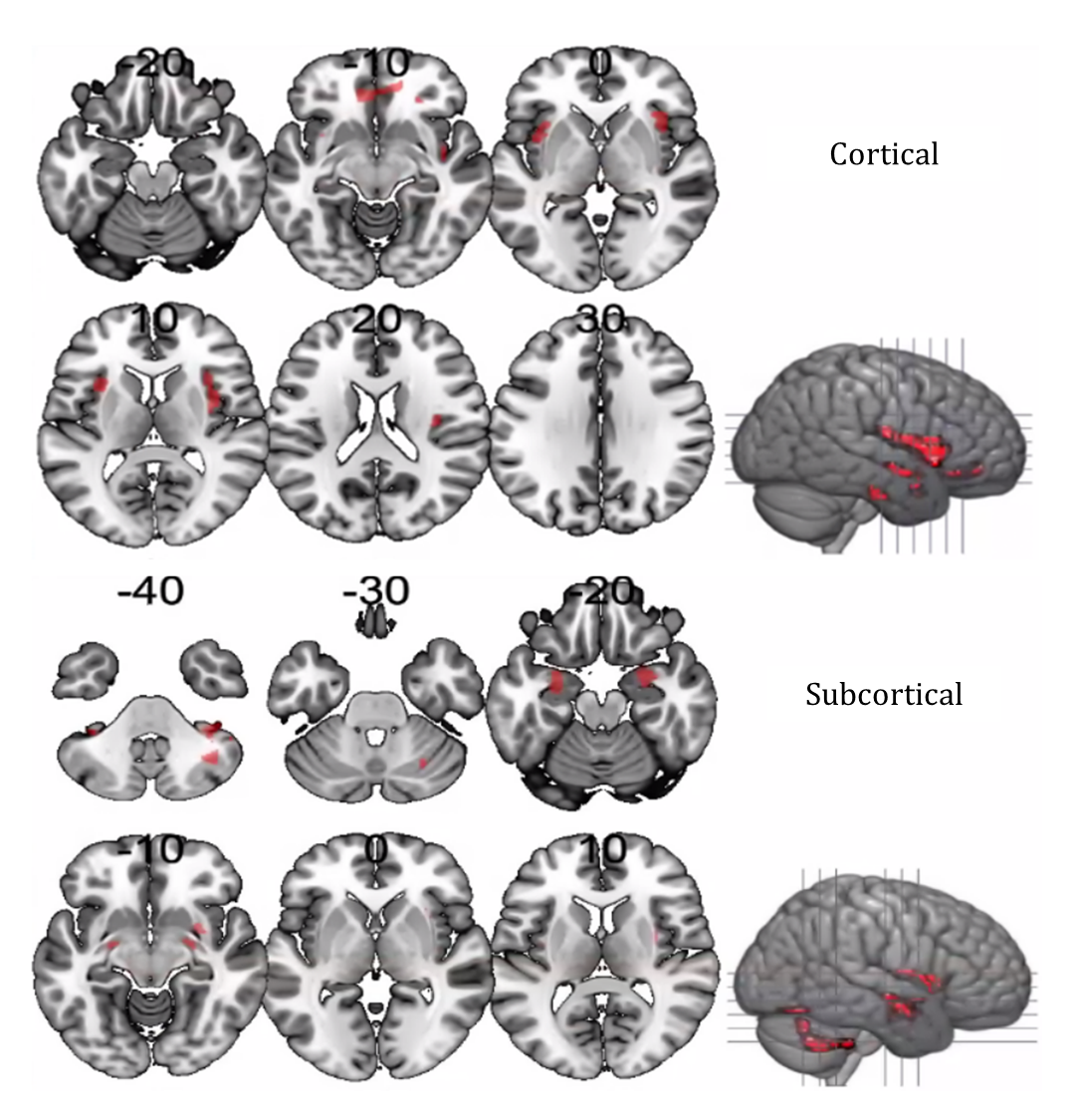
Reduction of the putaminal DaT SBR was common in PD patients, while iRBD patients displayed relatively spared SBR (Figure 1). Compared with HC, NM-MRI contrast was reduced (i) in the SN for all patients, with greater severity in the PDRBD+/a+ group; (ii) in the LC for PDRBD+/a+ and iRBD patients. Grey matter volume in the NBM was unchanged between groups.UPSIT correlated positively with NM-MRI contrast in the LC (Figure 2), but not in the SN. UPSIT correlated with grey matter volume (i) in the subcortical olfactory mask, including the NBM and cerebellum; (ii) in the cortical olfactory mask, including the insula, amygdala, anterior cingulate cortex, parahippocampal cortex, orbitofrontal cortex, and primary sensory cortex (Figure 3).
No correlation was found between UPSIT and DaT, cognitive score or motor score. Also, no correlation was found between cognitive score and grey matter volume in any region.
Discussion
Dopaminergic alterations were present in all groups but were not correlated with olfactory impairments in our cohort. Alteration of cholinergic subcortical regions correlated with UPSIT confirming the importance of this system for olfaction3. There was also a strong correlation between NM-MRI CNR in the LC and UPSIT. LC deficiency associated with anosmia was distinctive of the presence of RBD, whereas volume loss in the NBM was a common feature in all anosmic patient.The NBM has been associated with cognitive dysfunction10. However, patients had no or only mild cognitive symptoms and grey matter changes in the NBM did not correlate with cognitive scores. Therefore, the correlation observed between olfactory impairment and NBM grey matter changes were independent of cognitive disorders.
Conclusion
Our results suggest that olfactory dysfunction in PD is associated with progression patterns specific to patients with RBD involving the interplay between noradrenergic and cholinergic pathways.Acknowledgements
The ICEBERG study was funded by grants from the Investissements d'Avenir, IAIHU-06 (Paris Institute of Neurosciences – IHU), ANR-11-INBS-0006, Fondation d’Entreprise EDF, Biogen Inc., Fondation Thérèse and René Planiol, Fondation Saint Michel, Unrestricted support for Research on Parkinson’s disease from Energipole (M. Mallart), M.Villain and Société Française de Médecine Esthétique (M. Legrand)References
1. Doty, R. L. Olfactory dysfunction in Parkinson disease. Nat. Rev. Neurol. 8, 329–339 (2012).
2. Aarsland, D. et al. Cognitive decline in Parkinson disease. Nat. Rev. Neurol. 13, 217–231 (2017).
3. Doty, R. L. Olfactory dysfunction in neurodegenerative diseases: is there a common pathological substrate? Lancet Neurol. 16, 478–488 (2017).
4. Braak, H., Ghebremedhin, E., Rüb, U., Bratzke, H. & Del Tredici, K. Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 318, 121–134 (2004).
5. García-Lorenzo, D. et al. The coeruleus/subcoeruleus complex in rapid eye movement sleep behaviour disorders in Parkinson’s disease. Brain 136, 2120–2129 (2013).
6. Biondetti, E. et al. The spatiotemporal changes in dopamine, neuromelanin and iron characterizing Parkinson’s disease. Brain J. Neurol. 144, 3114–3125 (2021).
7. Nobileau, A. et al. Neuromelanin-Sensitive Magnetic Resonance Imaging Changes in the Locus Coeruleus/Subcoeruleus Complex in Patients with Typical and Atypical Parkinsonism. Mov. Disord. 38, 479–484 (2023).
8. Kötter, R. et al. A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM). Philos. Trans. R. Soc. Lond. B. Biol. Sci. 356, 1293–1322 (2001).
9. Pyatigorskaya, N. et al. Magnetic Resonance Imaging Biomarkers to Assess Substantia Nigra Damage in Idiopathic Rapid Eye Movement Sleep Behavior Disorder. Sleep 40, zsx149 (2017).
10. Ray, N. J. et al. In vivo cholinergic basal forebrain atrophy predicts cognitive decline in de novo Parkinson’s disease. Brain J. Neurol. 141, 165–176 (2018).
Figures
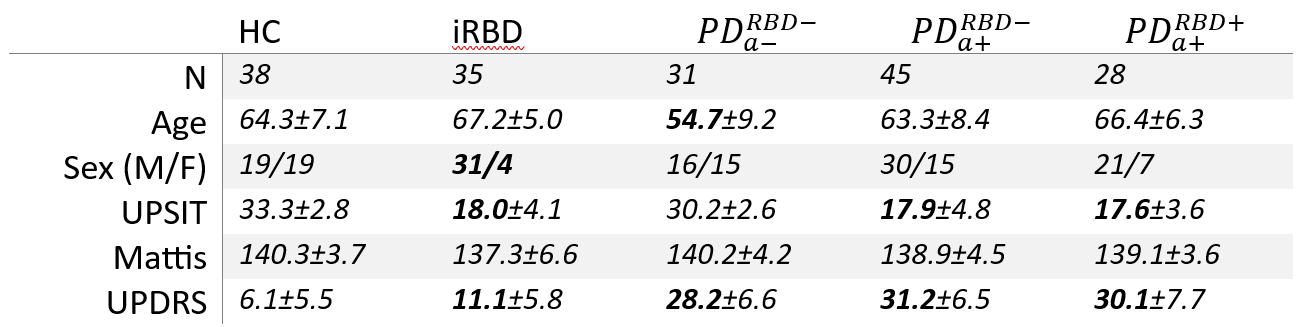
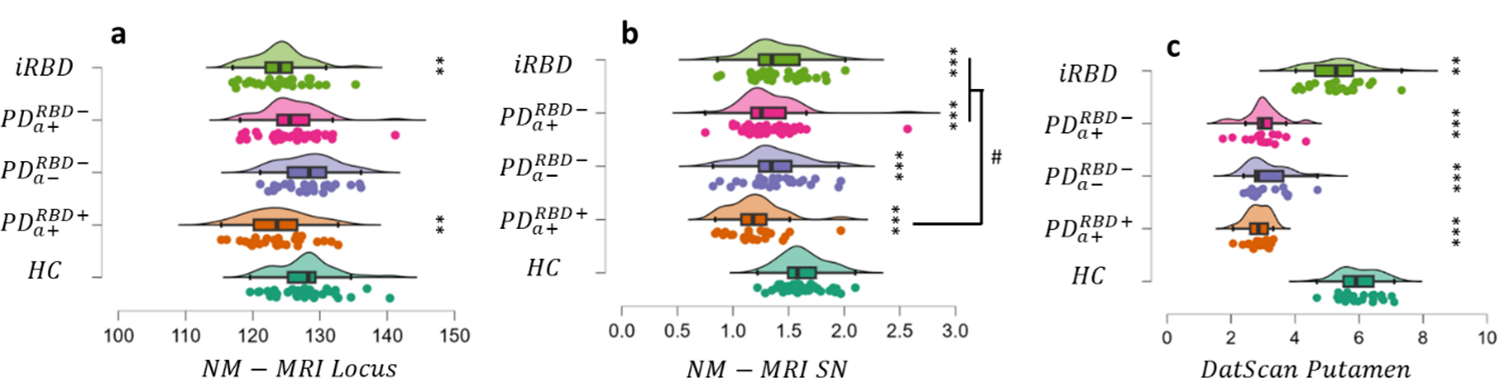
Figure 1: Group difference in multimodal MRI markers of subcortical nodes provided by ANCOVA with age as a covariate, and with Tukey’s post-hoc tests. a) NM-MRI CNR of locus coeruleus. b) NM-MRI CNR of substantia nigra. c) DaT specific binding ratio in the putamen. Significant differences with HC are highlighted *p<0.05, **p<0.01, ***p<0.001. #p<0.05 compared with PDRBD+/a+.