0298
Real-Time Imaging of Lower Airway Collapse at 0.55T1Ming Hsieh Department of Electrical and Computer Engineering, University of Southern California, Los Angeles, CA, United States, 2Children's Hospital Los Angeles, Los Angeles, CA, United States, 3National Institutes of Health, Bethesda, MD, United States
Synopsis
Keywords: Rare Disease, Low-Field MRI, Acquisition Methods, Data Acquisition, Pulse Sequence Design, Lower Airway, Tracheomalacia, Lung
Motivation: Tracheomalacia involves intermittent collapse of the lower airway and is difficult to diagnose. Currently, this condition is evaluated with invasive procedures like bronchoscopy or dynamic computer tomography (CT) which utilizes ionizing radiation.
Goal(s): To develop and optimize a high spatial and temporal resolution pulse sequence for evaluating tracheomalacia at 0.55T.
Approach: We optimize contrast (sequence, flip angle) for dynamic imaging in the lower airway for both 2D and SMS real-time imaging.
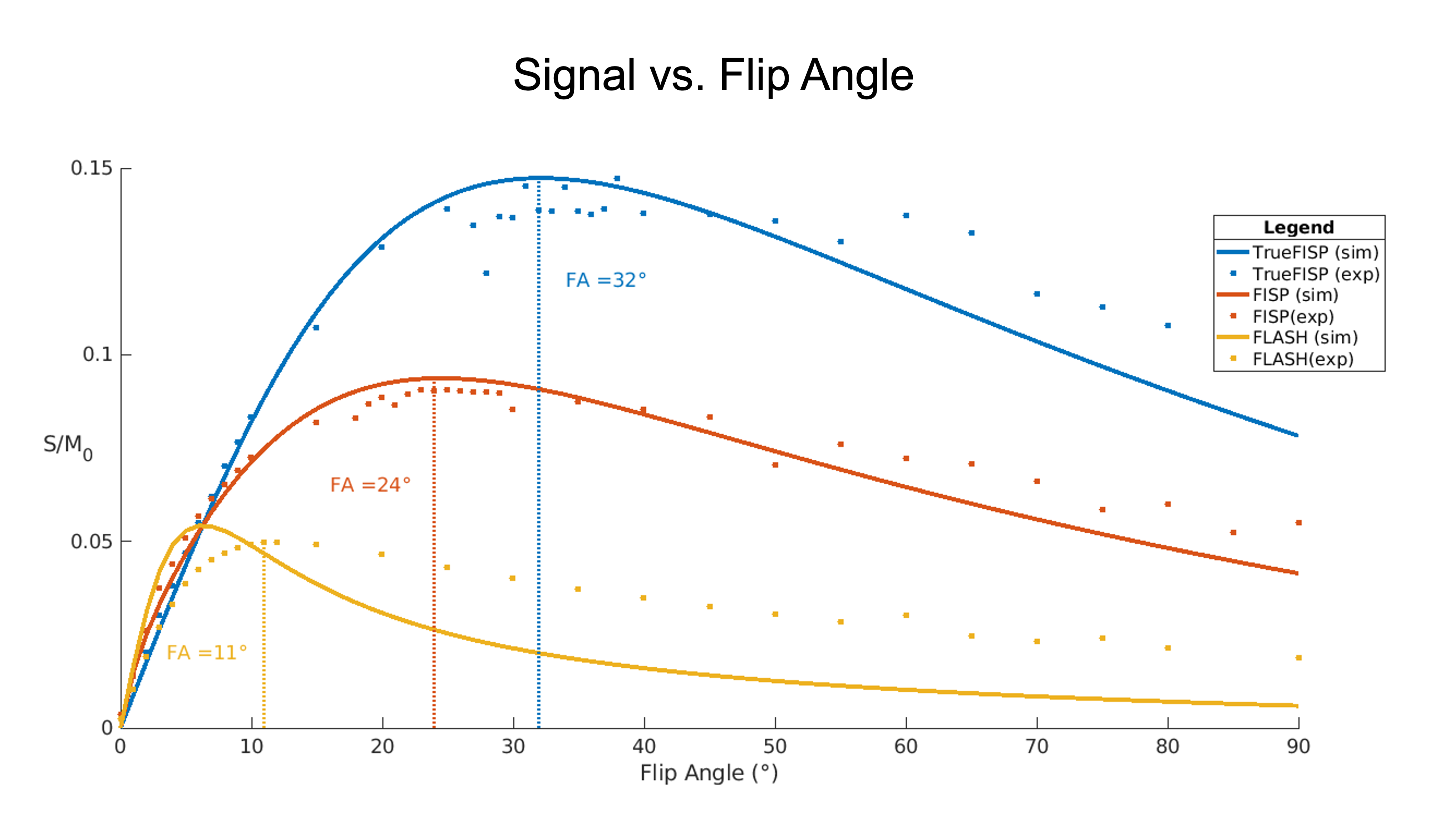
Results: Spiral acquisition achieves sufficient temporal resolution and the TrueFISP sequence (flip angle=32°) offers optimal contrast for imaging lower airway collapse.
Impact: We demonstrate the feasibility of capturing lower airway collapse with 2D and SMS real-time imaging (at 0.55T) in a way that is informative to the diagnosis and longitudinal monitoring of tracheomalacia.
Introduction
Tracheomalacia (TM) is characterized by damage to cartilaginous structures within the trachea that causes intermittent airway collapse; ultimately, this can lead to significant morbidity and mortality1. Diagnosis of TM is challenging, often necessitating invasive procedures such as bronchoscopy, which can underestimate the severity of collapse. Dynamic CT has been explored as a potential diagnostic tool for TM; however, it deposits high levels of radiation2.There is an opportunity for MRI to provide value in the evaluation of lower airway collapse patients. Additionally, the decreased susceptibility artifacts experienced at lower field strengths such as 0.55T allow for better imaging of airway dynamics3,4. We propose a protocol consisting of 2D and SMS real-time sequences that can resolve intermittent collapse with sufficient spatial and temporal resolution; this is similar to prior work at higher field strengths, but with substantially better spatiotemporal resolution5. We utilize spiral sampling and explore various sequences and flip angles (FA) to optimize the acquisition. Our primary objective is to outline the technical development required to prove that 0.55T MRI is capable of evaluating TM.
Methods
Experimental MethodsExperiments were performed using a whole body 0.55T system (prototype Magnetom Aera, Siemens Healthineers, Erlangen, Germany) equipped with high-performance shielded gradients (45 mT/m amplitude, 200 T/m/s slew rate). Seven healthy adult volunteers (age 22-30, 3F), and three patients with tracheomalacia/suspected bronchomalacia (age 6-13, M) were enrolled in this study, under a protocol approved by our Institutional Review Board and after providing written informed consent. The imaging protocol includes a real-time TrueFISP localizer, 2D real-time spiral FLASH/FISP/TrueFISP, and SMS real-time spiral TrueFISP. During the scan, patients were instructed to perform breathing maneuvers such as sustained expiration, bearing down, and repeated coughing. Total scan times were ≤1 hour.
Pulse Sequence
2D and SMS real-time spiral scans were implemented in the RTHawk (HeartVista, Inc., Menlo Park, CA) real-time interactive scanning platform6. Three different sequences were tested with golden-angle spiral trajectories: FLASH, FISP, and TrueFISP.
Evaluation
Reconstruction for spiral sequences was performed offline with GIRF corrected spiral trajectory and with spatially and temporally constrained reconstruction7-9. Online low-latency gridding reconstruction was provided to the scan operator without GIRF correction.
Results
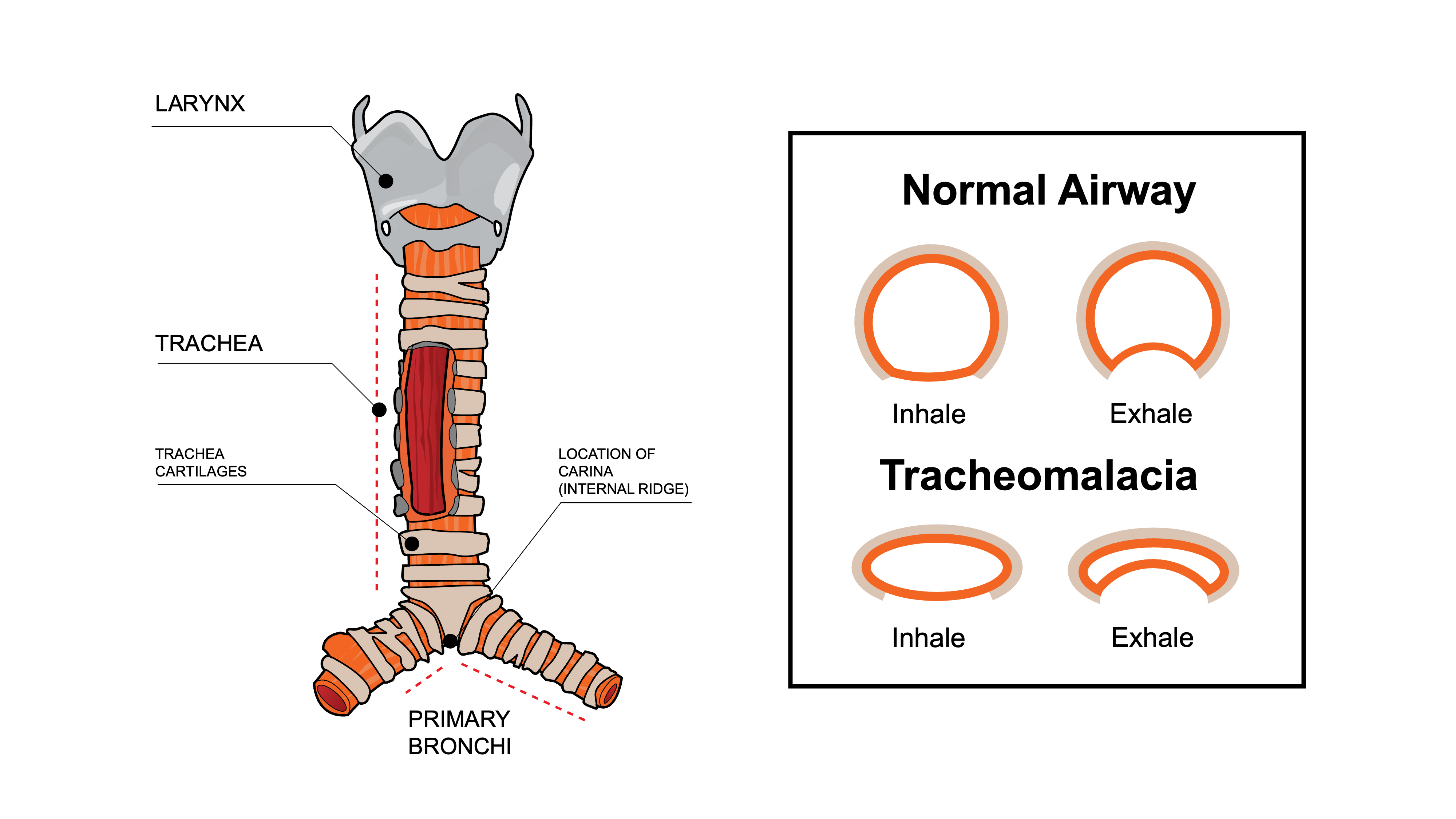
Figure 1 illustrates the airway anatomy and its important structures, such as the cartilaginous C-rings that scaffold the trachea and the smooth muscle tissue on the posterior wall10. Additionally, axial views of the airway are compared for a healthy adult and a patient with TM during inhalation and exhalation.Figure 2 shows signal intensity normalized by the proton density as a function of FA for each of the FLASH, FISP, and TrueFISP sequences. Experiment and simulation results are compared in order to identify the optimal FAs (FAFLASH=11°, FAFISP=24°, FATrueFISP=32°).
Figure 3 compares FLASH, FISP, and TrueFISP 2D real-time spiral sequences in the lower airway at 1.8x1.8x6mm3 resolution. Each was acquired at the optimal FAs identified in Figure 2. Noise dominates in the FLASH acquisition, while FISP is affected by flow artifacts. TrueFISP was identified as the optimal sequence due to its robustness to both noise and flow artifacts. SNR was calculated by performing an SNR-unit recon and estimating the noise covariance matrix from a FA = 0° acquisition11.
Figure 4 displays 2D real-time spiral scans of a patient with TM at 1.8x1.8x6mm3 spatial resolution and 146ms temporal resolution. Intermittent collapse is easily visualized and a 58% reduction in cross-sectional area was observed.
Figure 5 demonstrates that SMS real-time spiral imaging can resolve lower airway collapse along the inferior-superior axis. Depending on the placement of the slice group, airway collapse is captured in (a) a subset of the slices or (b) all three slices. This confirms that collapse severity varies along the trachea and motivates the need for monitoring collapse along the length of the airway.
Discussion and Conclusion
In this study, we demonstrate the feasibility of resolving intermittent airway collapse in the lower trachea with 0.55T MRI. 2D real-time spiral acquisition was optimized over sequence type and FA to achieve maximum SNR and contrast in the region of interest. Results indicate that TrueFISP is most robust to motion artifacts and flow, while maintaining high CNR/SNR in the lower airway. This permitted both 2D real-time and SMS real-time imaging of intermittent airway collapse in patients with TM. Future work will focus on improving the spatial and temporal resolution of the spiral trajectory scans in order to apply this work to younger patients with smaller anatomical features. Reducing flow artifacts in the SMS real-time acquisitions is also of interest in order to provide monitoring capability of the collapse along the length of the airway.Acknowledgements
We acknowledge grant support from the National Institutes of Health (U01-HL167613) and research support from Siemens Healthineers.References
[1] Aslam A, De Luis Cardenas J, Morrison RJ, et al. Tracheobronchomalacia and Excessive Dynamic Airway Collapse: Current Concepts and Future Directions. RadioGraphics. 2022;42(4):1012-1027. doi:10.1148/rg.210155
[2] Wagnetz U, Roberts HC, Chung T, Patsios D, Chapman KR, Paul NS. Dynamic Airway Evaluation with Volume CT: Initial Experience. Can Assoc Radiol J. 2010;61(2):90-97. doi:10.1016/j.carj.2009.11.007
[3] Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
[4] Lim Y, Kumar P, Nayak KS. Speech production real-time MRI at 0.55 T. Magn Reson Med. 2023;10.1002/mrm.29843. doi:10.1002/mrm.29843
[5] Wu Z, Chen W, Khoo MC, Davidson Ward SL, Nayak KS. Evaluation of upper airway collapsibility using real-time MRI. J Magn Reson Imaging. 2016;44(1):158-167. doi:10.1002/jmri.25133
[6] Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med BiolSoc. 2004;2004:1048-1051.
[7] Campbell-Washburn AE, Xue H, Lederman RJ, Faranesh AZ, Hansen MS. Real-time distortion correction of spiral and echo planar images using the gradient system impulse response function. Magnetic Resonance in Medicine. 2016;75(6):2278-2285. doi:10.1002/mrm.25788
[8] Tian Y, Mendes J, Pedgaonkar A, Ibrahim M, Jensen L, Schroeder JD, Wilson B, DiBella EVR, Adluru G. Feasibility of multiple-view myocardial perfusion MRI using radial simultaneous multi-slice acquisitions. PLoS One 2019;14(2):e0211738.
[9] Adluru G, McGann C, Speier P, Kholmovski EG, Shaaban A, Dibella EV. Acquisition and reconstruction of undersampled radial data for myocardial perfusion magnetic resonance imaging. J Magn Reson Imaging. 2009;29(2):466-473. doi:10.1002/jmri.21585
[10] Digital art, Hariadhi, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons.
[11] Kellman P, McVeigh ER. Image reconstruction in SNR units: a general method for SNR measurement [published correction appears in Magn Reson Med. 2007 Jul;58(1):211-2]. Magn Reson Med. 2005;54(6):1439-1447. doi:10.1002/mrm.20713
Figures