0297
Feasibility of MRI-based lung tissue mechanics computational models of the paediatric lung1Auckland Bioengineering Institute, University of Auckland, Auckland, New Zealand, 2GE Healthcare Australia and New Zealand, Auckland, New Zealand, 3Mātai Medical Research Institute, Gisborne, New Zealand, 4Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand, 5Ngāti Porou, Ngāti Kahungungu, Rongomaiwahine, Rongowhakaata; Tūranganui-a-Kiwa, Tairāwhiti, New Zealand
Synopsis
Keywords: Lung, Lung
Motivation: There is a scarcity of personalised computational physiology models of the paediatric lung because most models have previously been derived for the adult lung from CT images.
Goal(s): We aim to derive personalised computational models of the paediatric lung from novel structure-function lung MRI techniques.
Approach: In this feasibility study, lung ZTE MR images from healthy children were used to create finite element soft tissue deformation mechanics models.
Results: Simulations of regional supine lung tissue densities were shown to be similar to lung ZTE MRI densities, demonstrating the strong potential for developing computational paediatric lung models from MR images.
Impact: A computational physiology model of soft tissue deformation was created from lung ZTE MR images of healthy children, demonstrating the potential of using novel regional lung structure-function information for personalised paediatric computational models.
BACKGROUND
Computational physiology modelling is a useful approach for understanding the underlying pathophysiology mechanisms in various stages of disease, and for guiding personalised treatment plans. There is currently a scarcity of personalised computational models of the paediatric lung because most existing models rely on CT imaging and therefore have been derived for the adult lung [1-3]. Recent advancements in MRI acquisition and analysis techniques can now provide novel regional structure-function information of the lungs, making MRI a promising clinical tool to guide paediatric lung disease management [4-5], and provides an opportunity to derive new computational structure-function models for children.In this work we aim to create an MRI-to-model platform that utilises novel zero echo time (ZTE) lung MRI to derive personalised computational models of lung tissue mechanics in a paediatric lung. The lung’s tissue density distribution under supine gravitational loading will be simulated and evaluated against approximate density values extracted from the MR images.
METHODS
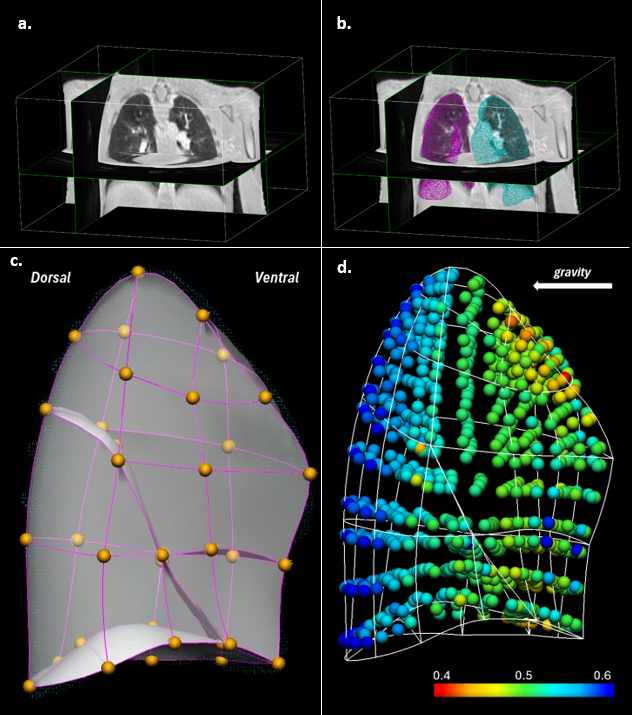
Subject information & image acquisitionNine healthy children (7 male, 2 female), with no history of respiratory disease, aged 8–11 years underwent ZTE lung MRI [6] on a GE SIGNA Premier 3T scanner in Tairāwhiti-Gisborne, New Zealand, using 20-channel anterior and 60-channel posterior array coils. Ethical approval was obtained through the New Zealand Health and Disability Ethics Committee (20/CEN/107) [7]. 3D radial ZTE lung MRI (TR: 2.5 ms; TE: 16 µs; FA: 1°; Voxel: ~1.5 mm isotropic) was acquired during 2 minutes free-breathing with prospective respiratory bellows gating on expiration (functional residual capacity, FRC) (Figure 1a).
Image Processing
The lung cavity was segmented semi-automatically from ZTE lung MRI using ITK-Snap software (Figure 1b). Larger airways were manually removed from the segmentation. MRI intensity values within the lung cavity were normalised to the chest muscle signal and the resultant values were assumed to be an approximation of true density [8].
Finite element modelling
Only the left lung geometry was considered for finite element (FE) modelling using in-house code (https://github.com/LungNoodle/lungsim). A cubic Hermite FE mesh geometry was fitted to the segmented left lung (Figure 1c) to give a curvilinear surface mesh with derivative continuity at the mesh nodes. The fitting process was semi-automated, requiring user interaction to manually edit some nodes and derivatives to achieve best fit (mesh fit RMS error <5mm). The mesh was then converted to quadratic Lagrange for simulation of soft tissue deformation mechanics that was previously established for a CT-based modelling workflow [3]. The distribution of tissue volumes, stress, and strain at FRC in the supine posture was simulated. The tissue mechanics model’s accuracy was validated by comparing its mean density for 10mm slice bins along the gravitational (dorso-ventral) direction against the equivalent normalised ZTE lung MRI density bins.
RESULTS AND DISCUSSION
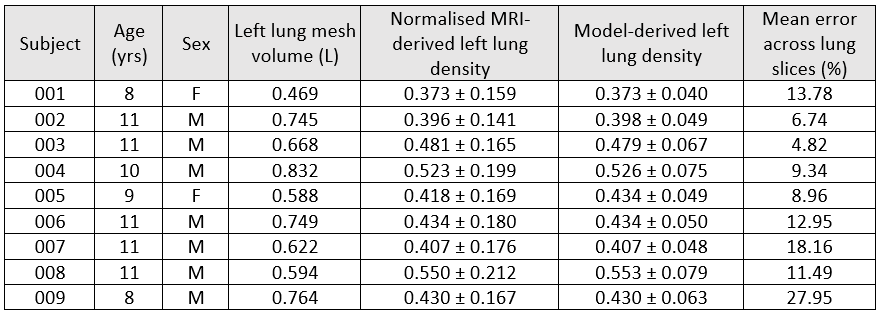
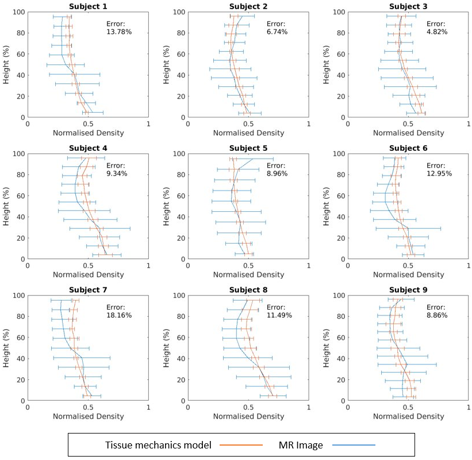
Personalised lung tissue mechanics models were derived from ZTE lung MRI in all nine children (Table 1). The average density error in normalised global left lung density between MRI and model was 0.652 ± 1.22%, suggesting that the density is accurately predicted by the MRI-based tissue mechanics model. Figure 1d illustrates the gravitational gradient distribution of tissue density in the simulated supine posture, showing higher and lower values for tissue density in the dorsal and ventral regions, respectively.Figure 2 shows similar gravitational gradients along the dorso-ventral axis for both MRI- and model-derived densities. Moreover, our MRI-based supine FRC gravitational gradients are comparable to those derived from the established CT-based modelling workflow for adult lungs [3]. The mean absolute error slice bin difference across all subjects was 12.7 ± 6.96%, and further indicates our MRI-based tissue mechanics model can simulate regional changes in tissue density from gravitational loading. The large discrepancy between model and MRI density curves observed in Subjects 007 and 009 may have resulted from poor manual lung segmentation or manual mesh fitting.
Our results demonstrate the feasibility of creating personalised MRI-derived lung tissue mechanics models of the paediatric lung. In future work, the MRI-based mechanics models will be further validated in a cohort of subjects with corresponding CT images, and combined with other computational models that simulate different aspects of paediatric lung structure and function.
CONCLUSION
ZTE lung MRI data from nine healthy children were used to create personalised lung tissue mechanics models of the paediatric lung. Good agreement was observed between FE simulations and MRI-derived supine distribution of lung tissue density. This demonstrates the strong potential for developing computational paediatric lung models from novel lung MRI.Acknowledgements
This work was supported by funding from the Aotearoa Foundation and Kānoa Regional Economic Development & Investment Unit, New Zealand. We would like to acknowledge the technical support from GE Healthcare.References
[1] A. J. Swan, A. R. Clark, and M. H. Tawhai, “A computational model of the topographic distribution of ventilation in healthy human lungs,” Journal of Theoretical Biology, vol. 300, pp. 222–231, 2012. doi:10.1016/j.jtbi.2012.01.042
[2] A. R. Clark, M. H. Tawhai, E. A. Hoffman, and K. S. Burrowes, “The interdependent contributions of gravitational and structural features to perfusion distribution in a multiscale model of the pulmonary circulation,” Journal of Applied Physiology, vol. 110, no. 4, pp. 943–955, 2011. doi:10.1152/japplphysiol.00775.2010
[3] M. H. Tawhai, M. P. Nash, C.-L. Lin, and E. A. Hoffman, “Supine and prone differences in regional lung density and pleural pressure gradients in the human lung with constant shape,” Journal of Applied Physiology, vol. 107, no. 3, pp. 912–920, 2009. doi:10.1152/japplphysiol.00324.2009
[4] J. C. Woods et al., “Current state of the art MRI for the longitudinal assessment of Cystic Fibrosis,” Journal of Magnetic Resonance Imaging, vol. 52, no. 5, pp. 1306–1320, 2019. doi:10.1002/jmri.27030
[5] N. J. Stewart et al., “Lung MRI with hyperpolarised gases: Current & Future Clinical Perspectives,” The British Journal of Radiology, vol. 95, no. 1132, 2022. doi:10.1259/bjr.20210207
[6] F. Gibiino, L. Sacolick, A. Menini, L. Landini, and F. Wiesinger, “Free-breathing, zero-TE MR lung imaging,” Magnetic Resonance Materials in Physics, Biology and Medicine, vol. 28, no. 3, pp. 207–215, 2014. doi:10.1007/s10334-014-0459-y
[7] H. Kumar et al., “Roadmap for an imaging and Modelling Paediatric Study in rural NZ,” Frontiers in Physiology, vol. 14, 2023. doi:10.3389/fphys.2023.1104838
[8] N. S. Higano et al., “Quantification of neonatal lung parenchymal density via ultrashort echo time MRI with comparison to CT,” Journal of Magnetic Resonance Imaging, vol. 46, no. 4, pp. 992–1000, 2017. doi:10.1002/jmri.25643
Figures