0296
Comparison of MR-Signal-based and Deformation-based Ventilation Measurement in Pediatric Patients with non-CF Bronchiectasis1Institute for Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany, 2Biomedical Research in Endstage and Obstructive Lung Disease Hannover (BREATH), Member of the German Center for Lung Research, Hannover, Germany
Synopsis
Keywords: Lung, Lung, Registration, Ventilation, Free-Breathing
Motivation: A previous study showed that MR-signal-based (RVent) and deformation-based approaches (JVent) for ventilation are theoretically equivalent, but result in different defects in a digital lung model. A verification of this finding using real data is pending.
Goal(s): Test if both ventilation parameters result in significant differences on a global and regional level.
Approach: A retrospective analysis of 32 patients with non-CF Bronchiectasis was performed, calculating RVent, JVent and corresponding ventilation defects for three registration variants.
Results: There were significant differences and patterns on a global and regional level, which are consistent with the findings in the lung model study.
Impact: Inferior-superior gradient in deformation-based ventilation measurements might lead to a biased defect detection. Therefore, use of such parameters might require further correction and/or diligent registration optimization. Thus, signal-based ventilation with more stable performance across different registration variants might be benefical.
Introduction
Recently, a digital lung model was introduced as a means for validation of functional lung imaging based on free-breathing MR time-series1. Such methods include Matrix Pencil Decomposition2, Phase-Resolved Functional Lung (PREFUL) MRI3 or 3D MR spirometry4. A common post-processing step for such methods is the motion-compensation via registration. Subsequently, the deformation fields can be analyzed to deduce ventilation from geometry by Jacobian determinant (JVent). Alternatively, the reciprocal relationship of MR-signal and volume is used to derive ventilation from the signal variations (RVent)5.The digital lung model showed different performance in detecting the predefined defect classes for both ventilation methods. JVent values were decreasing towards the superior direction and resulted in no reliable defect detection. Only defect classes with high contrast to the surrounding were detectable with JVent.
An additional test in real data is mandatory to exclude limitations of the model as a possible cause for this finding.
Methods
A subset of data from an observational cohort study of bronchiectasis patients without cystic fibrosis (non-CF bronchiectasis) was used for this study (n=32, female = 15, median age 13, age range 6-19).Scans were performed on a 1.5 T system using a spoiled gradient echo sequence with the following settings (provided as median with range): Field-of-view 395 (340-500) mm2, echo time 0.88 (0.88-0.91) ms, repetition time 3 ms, temporal resolution 192 ms, slice thickness 10 mm, matrix 128 x 128, parallel imaging acceleration factor 2, receive bandwidth 1500 Hz/Pixel for a total of 250 image frames for each slice. For the scope of this study, only the slice at tracheal bifurcation was considered for further analysis.
Images were registered to expiration state with ANTs6, the Forsberg registration (F-REG) method7,8 and a diffeomorphic demons algorithm9 implemented in MATLAB R2020b (M-REG).
The deformation fields created during registration were used to calculate the Jacobi matrix Jf, which consists of all partial derivatives of the total displacement. The determinant of this matrix yields total expansion/inflation of the respective voxel and was used to calculate ventilation:
$$\mathrm{JVent=\ }\frac{\mathrm{v}_{\mathrm{Insp}}\mathrm{-}\ \mathrm{v}_{\mathrm{Exp}}}{\mathrm{v}_{\mathrm{Exp}}}\mathrm{=}{\mathrm{det(J}}_\mathrm{f}\mathrm{\mathrm{)-1,}}$$
with the volumes v in expiration (Exp) and inspiration (Insp). Alternatively, the signal-to-volume relation (s~1/v) was used to derive the signal-based ventilation:
$$\mathrm{RVent=\ }\frac{\mathrm{v}_{\mathrm{Insp}}\mathrm{-}\ \mathrm{v}_{\mathrm{Exp}}}{\mathrm{v}_{\mathrm{Reg}}}\mathrm{=}\frac{\mathrm{s}_{\mathrm{Exp}}\mathrm{-}\ \mathrm{s}_{\mathrm{Insp}}}{\mathrm{s}_{\mathrm{Insp}}}.$$Prior to this calculation, the registered images were filtered with image guided filtering to account for low SNR10. Lung parenchyma region of interest (ROI) was automatically segmented and refined by vessel exclusion with convolutional networks. Ventilation defects (VD) were determined similarly to previous studies by an adaptive threshold (THR) for each RVent and JVent map:
$$\mathrm{THR=\ }{90}^{th}\mathrm{-Percentile(Map(ROI))\ *\ 0.4}.$$For statistical analysis, median values in the ROI were calculated. Additionally, the defect percentage was calculated for quadrants of the ROI: up right (UR), up left (UL), down right (DR) and down left (DL). Differences between registration and ventilation measurement methods were tested with Friedman’s test as omnibus test. For post-hoc, Wilcoxon signed rank test was performed at the 5% significance level.
Results
Figure 1, Figure 2 and Figure 3 show representative examples with mixed, strong and weak concordance for VD derived by JVent and RVent. All cases exhibited a decreasing quality of JVent: ANTs > F-REG > M-REG.Median values of JVent in comparison to RVent were elevated (e.g. ANTs: RVent = 0.09 vs. JVent = 0.19, P≤0.0001, see Table 1). Quadrant analysis demonstrated that defects were mainly found in upper quadrants for JVent with a reversed pattern for RVent, e.g. ANTs: UR/DRJVent= 33/18% vs. UR/DRRVent = 13/35%, P≤0.0001, see Table 2).
Discussion
Distinct patterns of VD derived by RVent and JVent were found in patients with non-CF bronchiectasis. If JVent is showing artificially high VD in the upper lung regions as found in the lung model study, cannot be inferred for sure due to missing gold standard. Nevertheless, the similarity of the pattern and the fact that certain regions showed decreased parenchymal signal (e.g. see Figure 3) associated with VDRVent, but no corresponding VDJVent suggests this interpretation. The strong regularization of deformation fields, preserving large movements but underestimating/removing smaller ones, might be an explanation for this finding. Therefore, other registration settings/algorithms might result in a different performance. Additionally, as suggested previously, an additional air-volume estimation could be used to account for bias in Jacobian-based estimations, but might be more challenging in MR setting compared to CT.11Conclusion
In the investigated setting, signal-based RVent seems to produce more reliable VD results in line with simulated data in comparison to deformation-based JVent measurements.Acknowledgements
This work was supported by the German Center for Lung Research (DZL). The authors would like to thank Frank Schröder and Sven Thiele from Diagnostic and Interventional Radiology (Hanover Medical School) for outstanding technical assistance in performing the MRI examinations.References
1. Voskrebenzev A, Gutberlet M, Klimeš F, Wacker F, Vogel-Claussen J. Introduction of a Digital Lung Model for Validation and Refinement of Functional Lung Imaging Methods. In: Proc. Intl. Soc. Mag. Reson. Med. 31. ; 2023:4820.
2. Bauman G, Bieri O. Matrix pencil decomposition of time-resolved proton MRI for robust and improved assessment of pulmonary ventilation and perfusion. Magn Reson Med. 2017;77(1):336-342. doi:10.1002/mrm.26096
3. Voskrebenzev A, Gutberlet M, Klimeš F, Kaireit TF, Schönfeld C, Rotärmel A, Wacker F, Vogel-Claussen J. Feasibility of quantitative regional ventilation and perfusion mapping with phase-resolved functional lung (PREFUL) MRI in healthy volunteers and COPD, CTEPH, and CF patients. Magn Reson Med. 2018;79(4):2306-2314. doi:10.1002/mrm.26893
4. Boucneau T, Fernandez B, Larson P, Darrasse L, Maître X. 3D Magnetic Resonance Spirometry. Sci Rep. 2020;10(1):9649. doi:10.1038/s41598-020-66202-7
5. Zapke M, Topf HG, Zenker M, Kuth R, Deimling M, Kreisler P, Rauh M, Chefd’hotel C, Geiger B, Rupprecht T. Magnetic resonance lung function – a breakthrough for lung imaging and functional assessment? A phantom study and clinical trial. Respir Res. 2006;7(1). doi:10.1186/1465-9921-7-106
6. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A Reproducible Evaluation of ANTs Similarity Metric Performance in Brain Image Registration. NeuroImage. 2011;54(3):2033-2044. doi:10.1016/j.neuroimage.2010.09.025
7. Forsberg D, Andersson M, Knutsson H. Extending Image Registration Using Polynomial Expansion To Diffeomorphic Deformations. In: SSBA Symposium on Image Analysis. ; 2012:4.
8. Forsberg D. fordanic/image-registration. Published online 2022. Accessed April 12, 2022. https://github.com/fordanic/image-registration
9. Vercauteren T, Pennec X, Perchant A, Ayache N. Diffeomorphic demons: Efficient non-parametric image registration. NeuroImage. 2009;45(1, Supplement 1):S61-S72. doi:10.1016/j.neuroimage.2008.10.040
10. He K, Sun J, Tang X. Guided Image Filtering. IEEE Trans Pattern Anal Mach Intell. 2013;35(6):1397-1409. doi:10.1109/TPAMI.2012.213
11. Castillo R, Castillo E, Martinez J, Guerrero T. Ventilation from four-dimensional computed tomography: density versus Jacobian methods. Phys Med Biol. 2010;55(16):4661. doi:10.1088/0031-9155/55/16/004
Figures
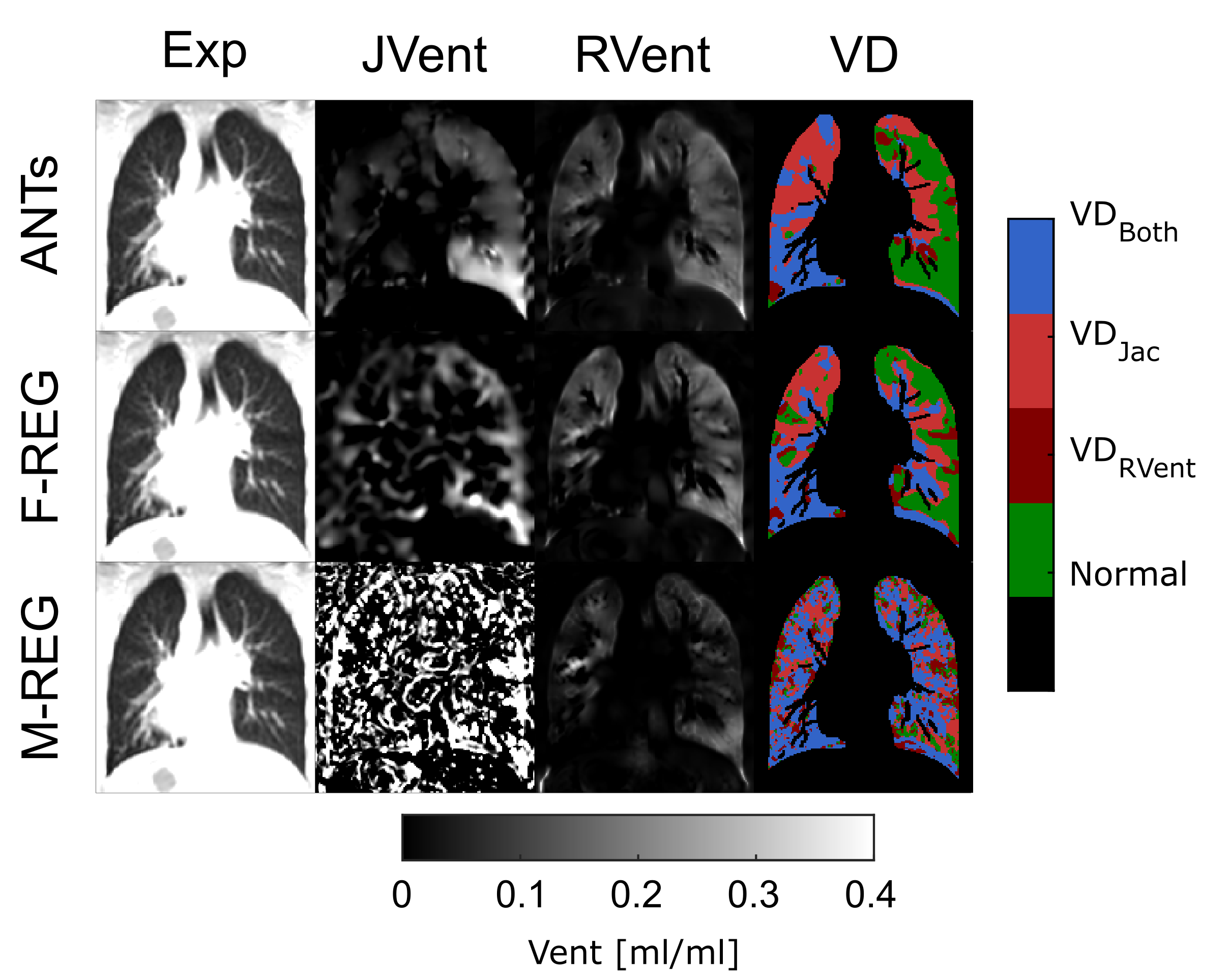
Figure 1 Mixed ventilation defect (VD) concordance of signal-based regional ventilation (RVent) and deformation-based ventilation (JVent) for a male non-CF bronchiectasis patient (age = 16). JVent showed VD in the whole right lung, whereas RVent only showed VD in the lower right region. A quality gradient of JVent is noticeable: ANTs > F-REG > M-REG. Differences for RVent are less pronounced, especially for ANTs and F-REG.
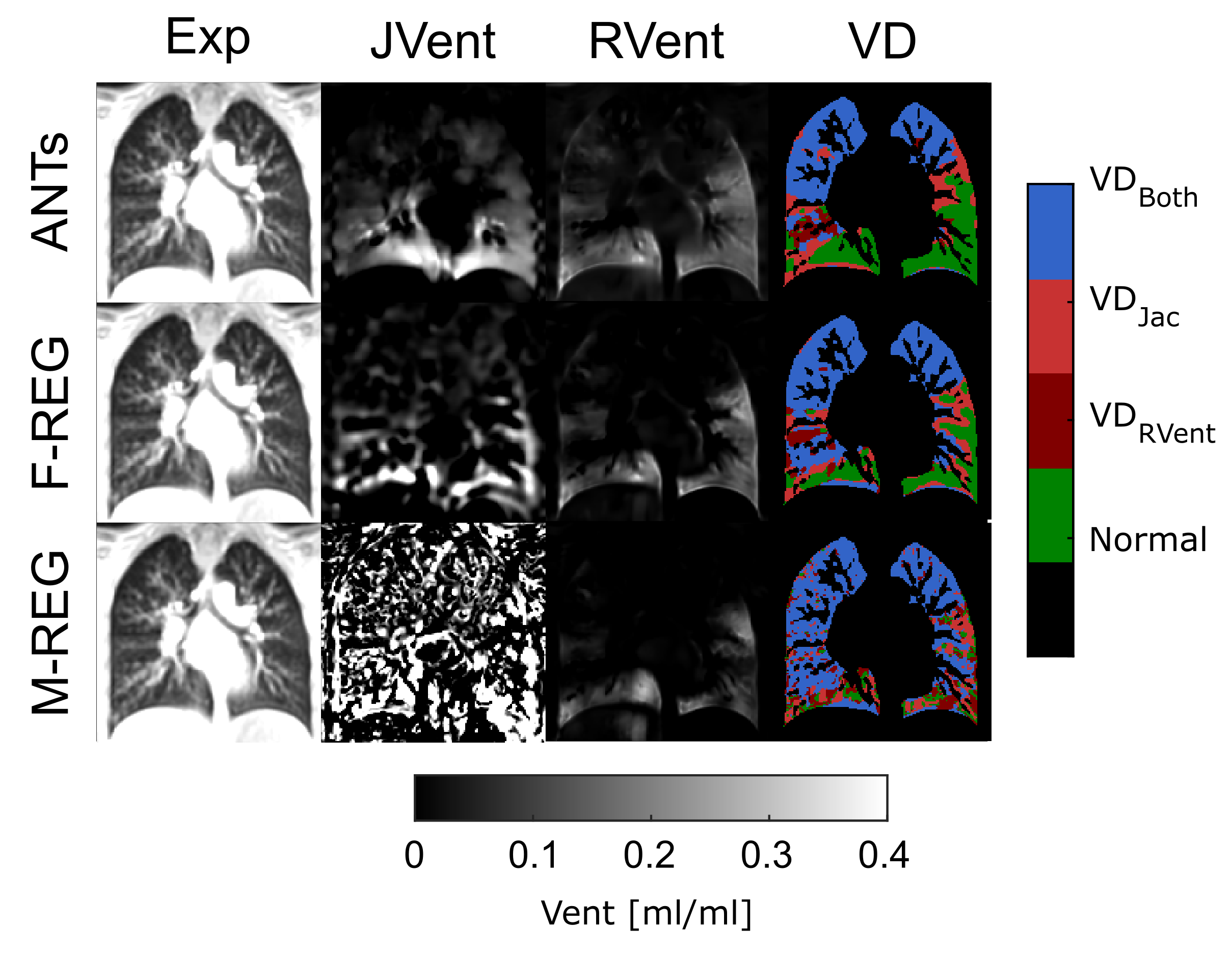
Figure 2 Strong ventilation defect (VD) concordance of signal-based regional ventilation (RVent) and deformation-based ventilation (JVent) for a female non-CF bronchiectasis patient (age = 15). JVent and RVent show similar VD patterns mainly located in the upper regions of the lung in this case. A quality gradient of JVent is noticeable: ANTs > F-REG > M-REG. Differences for RVent are less pronounced, especially for ANTs and F-REG.
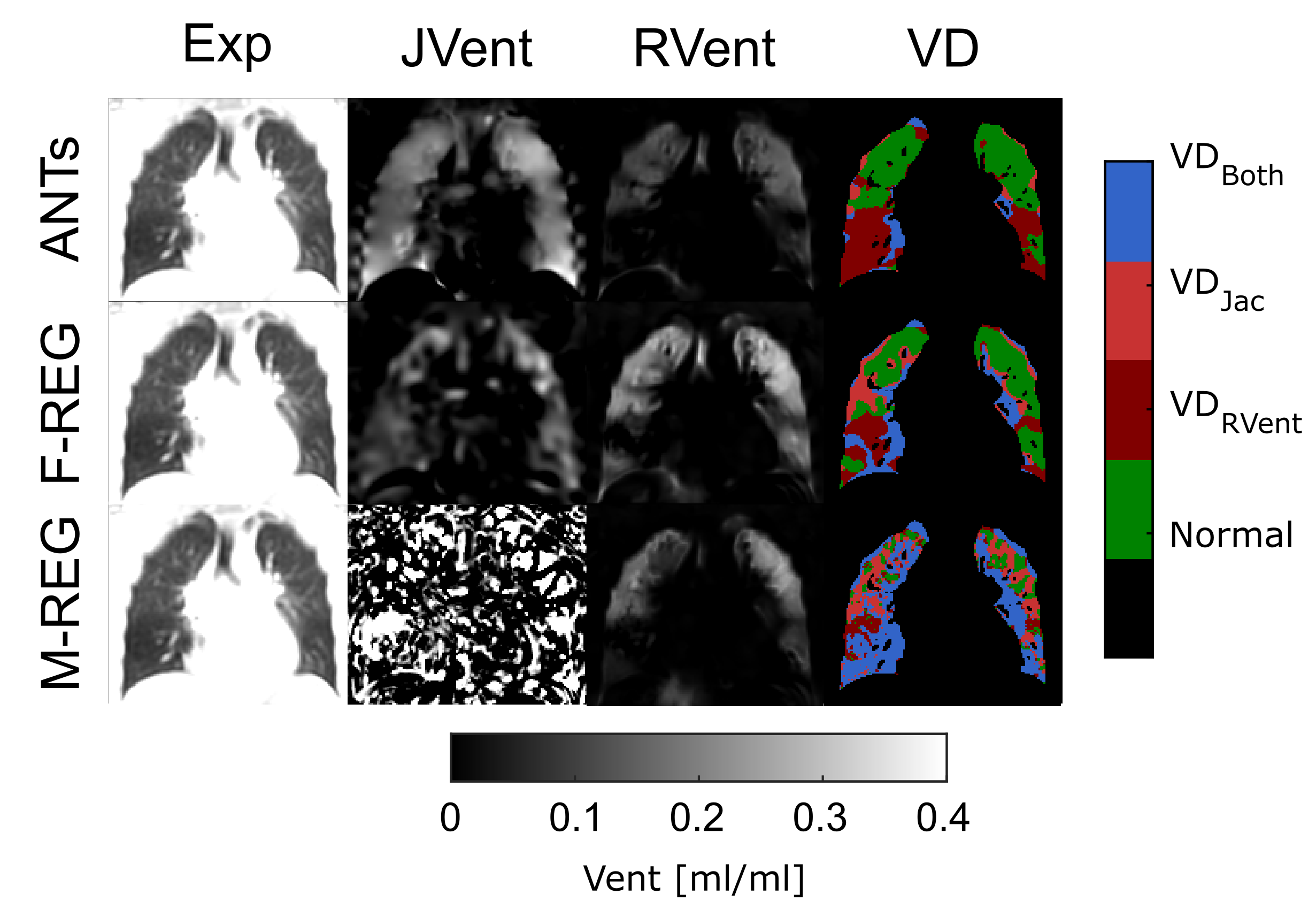
Figure 3 Weak ventilation defect (VD) concordance of signal-based regional ventilation (RVent) and deformation-based ventilation (JVent) for a male non-CF bronchiectasis patient (age = 17). Nearly no defects for JVent and large defects for RVent in lower lung regions were detected. A quality gradient of JVent is noticeable: ANTs > F-REG > M-REG. Differences for RVent are less pronounced for ANTs and F-REG.
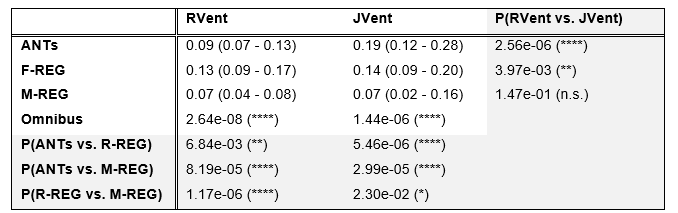
Table 1 RVent and JVent median (interquartile) values. Except for M-REG all values were significantly different comparing methods and registration variants. In general, JVent was increased in comparison to RVent. P≤0.05 (*), P≤0.01 (**), P≤0.001 (***), P≤0.0001 (****).
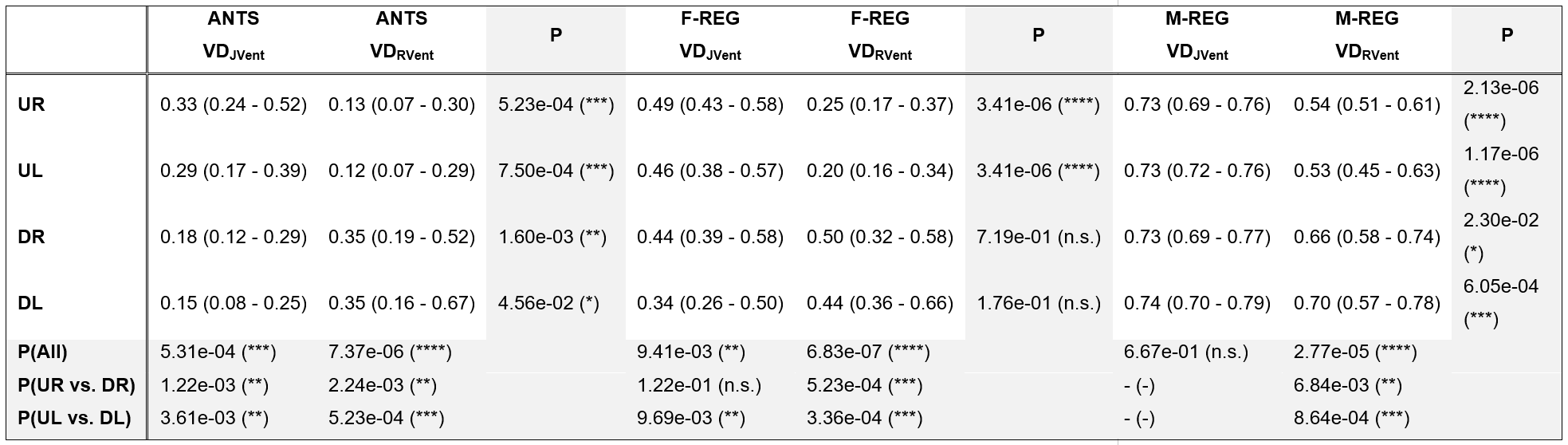
Table 2 Overview of ventilation defects (VD) for different quadrants (up right (UR), up left (UL), down right (DR) and down left (DL)). Significantly higher VDJVent were present in the upper lung regions in comparison to the lower regions for ANTs, and less pronounced for F-REG. RVent showed a reversed relationship for all registration variants. P≤0.05 (*), P≤0.01 (**), P≤0.001 (***), P≤0.0001 (****).