0294
Investigating Phase-Cycled bSSFP Imaging for Functional Lung Imaging in 2-Year-Olds After Congenital Diaphragmatic Hernia Repair1Computer Assisted Clinical Medicine, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany, 2Mannheim Institute for Intelligent Systems in Medicine, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany
Synopsis
Keywords: Lung, Lung, Functional, Pulmonary, non-contrast-enhanced
Motivation: bSSFP-based non-contrast-enhanced imaging is a promising alternative for functional lung imaging in pediatric patients. However, bSSFP acquisitions suffer from magnetic field inhomogeneities.
Goal(s): Our goal is to investigate phase-cycled bSSFP acquisitions as a robust alternative in pediatric functional lung imaging.
Approach: We acquired dynamic images using conventional and phase-cycled bSSFP acquisitions at 1.5T, from five 2-year-old patients after congenital diaphragmatic hernia repair. The images were non-rigid registered to a reference frame and functional maps were obtained using dynamic mode decomposition technique.
Results: We have successfully obtained functional maps in all patients and observed a trend toward improved ventilation map homogeneity using phase-cycled acquisitions.
Impact: Pulmonary functional maps obtained via non-contrast-enhanced bSSFP acquisitions may suffer from field inhomogeneity artifacts. Here, we investigate phase-cycled bSSFP imaging in 2-year-old congenital diaphragmatic hernia patients, and show improved robustness, which may be beneficial for lung function assessments.
Introduction
Congenital diaphragmatic hernia (CDH) belongs to rare diseases1, and is characterized by the herniation of abdominal organs into the thoracic cavity, resulting in impaired lung development, followed by irreversible hypoplasia of the pulmonary parenchyma and vasculature2. While advances in treatment have improved survival rates, CDH patients still suffer from morbidities, and periodic structured follow-up programs in specialized centers are strongly recommended to monitor and treat complications2.Previously, MRI based methods have been proposed to measure lung functions in CDH patients without the need for ionizing radiation2. Specifically, DCE MRI studies have shown observable differences between affected ipsilateral and contralateral lungs, which are reflected by lower pulmonary blood flow (PBF) in the ipsilateral lung3,4. However, safety concerns regarding Gadolinium‐based contrast agents limit the usefulness of DCE-based methods5.
Recently a non-contrast-enhanced method displayed that pulmonary ventilation and perfusion information can be obtained in these patients without the need for contrast agents6. This method uses bSSFP acquisitions to capture periodic signal changes present during dynamic acquisition, originating from periodic respiration and cardiac pulsation7. However, conventional bSSFP acquisitions may suffer from field inhomogeneity artifacts8, which results in local signal losses caused by banding artifacts and inhomogeneities in functional maps. Here, we investigate the application of phase-cycled bSSFP acquisitions to improve robustness against magnetic field inhomogeneities. We present results of in vivo measurements obtained from pediatric patients.
Methods
Five patients after CDH repair were measured as a part of our local follow-up study, where an MRI examination is included at the age of two. The study was approved by the local research ethics committee, and the written informed consent was obtained from the parents. The MRI examinations were performed at 1.5T (Magnetom Aera, Siemens Healthineers), and the patients underwent free-breathing MRI scans in supine position after propofol sedation. The bSSFP acquisitions were acquired using conventional and phase-cycled bSSFP pulse sequences as described previuously8. Sequence parameters were adapted for pediatric patients with FOV=280mmx280mm, slice thickness=12mm, TR/TR=0.99ms/2.31ms. For both acquisition schemes, 280 images were acquired with an acquisition rate of 4.87 images/s, and 4 different phase cycles $$$\Delta\phi=0^{\circ},90^{\circ},180^{\circ},270^{\circ}$$$ were utilized in the phase-cycled scheme.Afterwards, dynamic acquisitions were non-rigid registered to a reference frame8 and functional maps were obtained using dynamic mode decomposition technique9. For quantitative comparisons, analyses were performed on manually segmented ROIs containing lung parenchyma. For both acquisitions, ventilation and perfusion ratios between ipsilateral to contralateral lungs (I/C) were calculated to assess functional differences between the lungs, and coefficient of variation (CV) were calculated to assess functional map homogeneity within the lungs.
Results
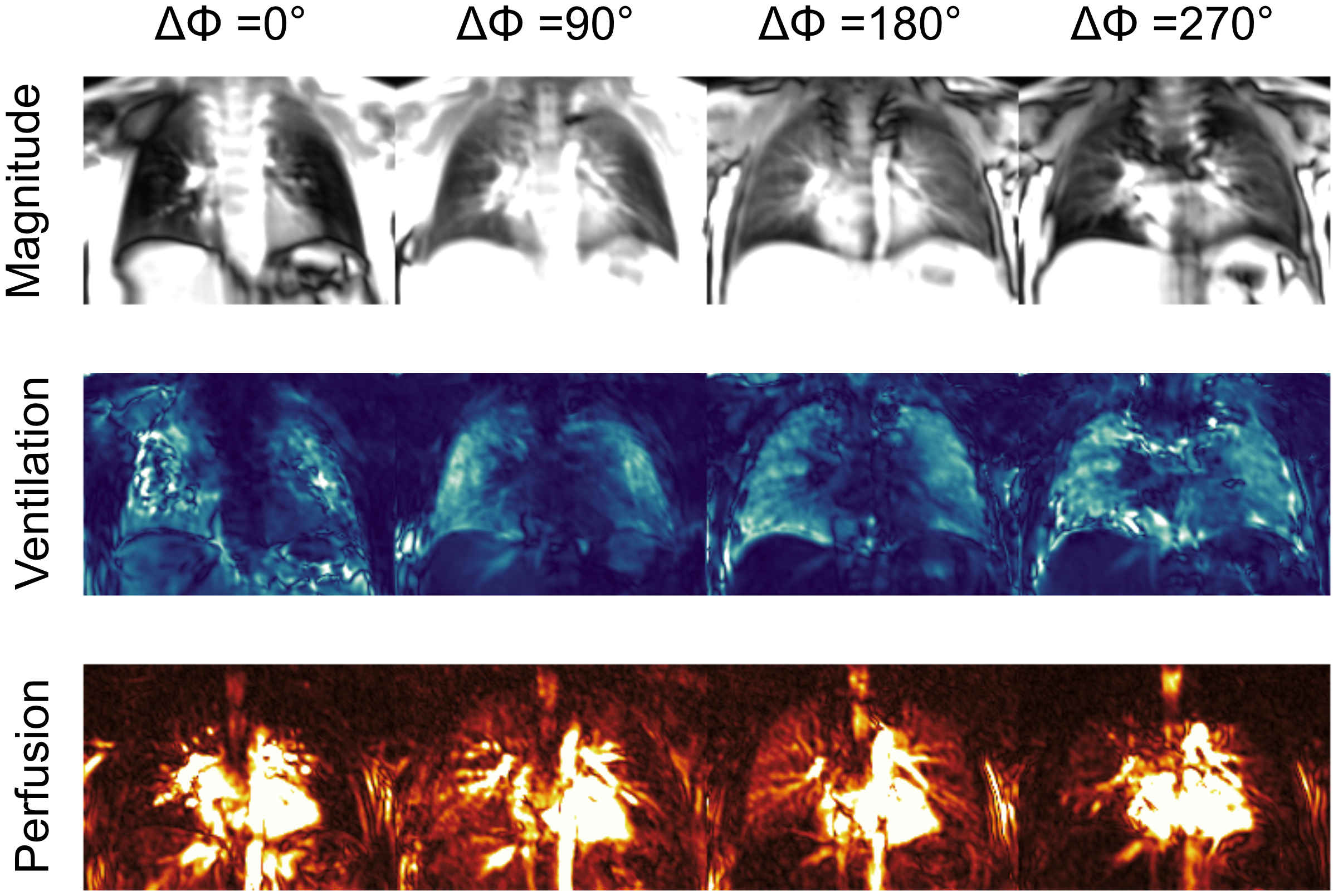
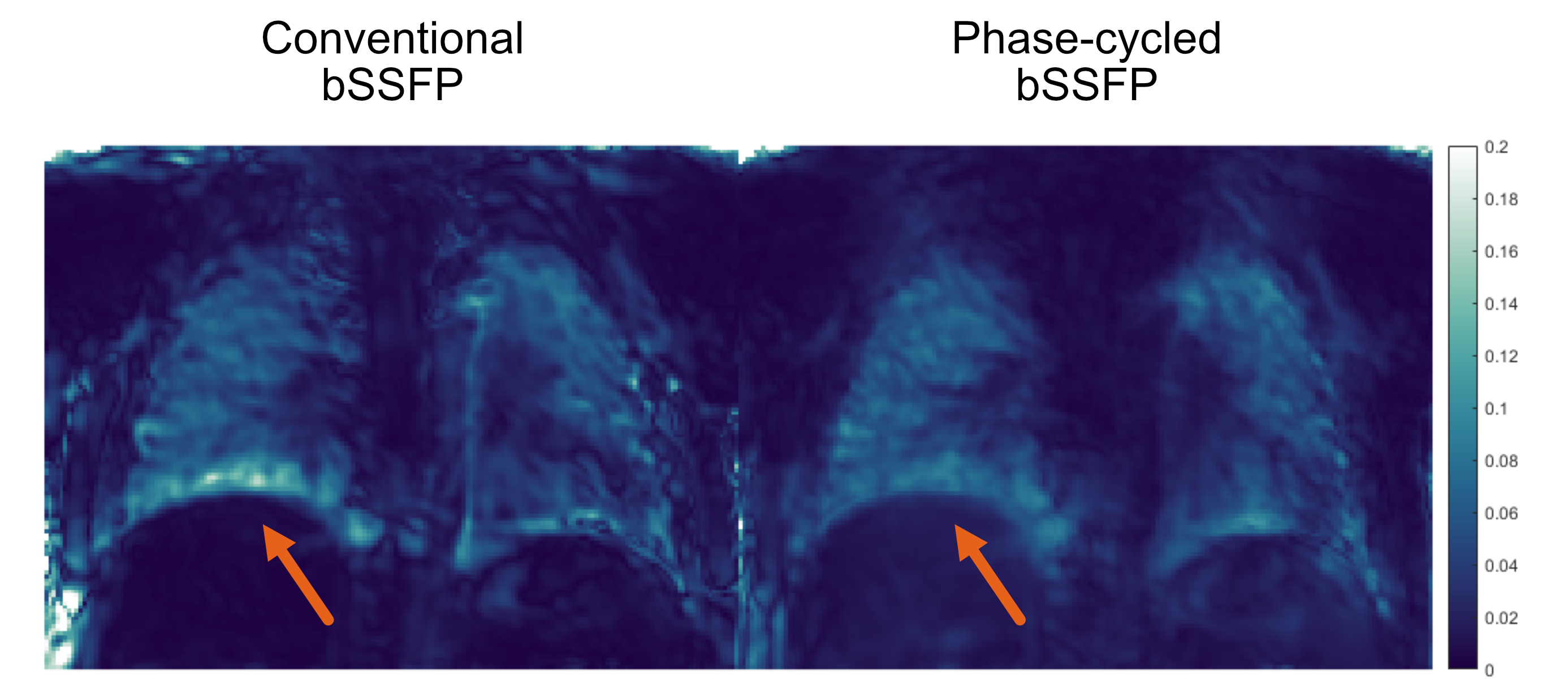
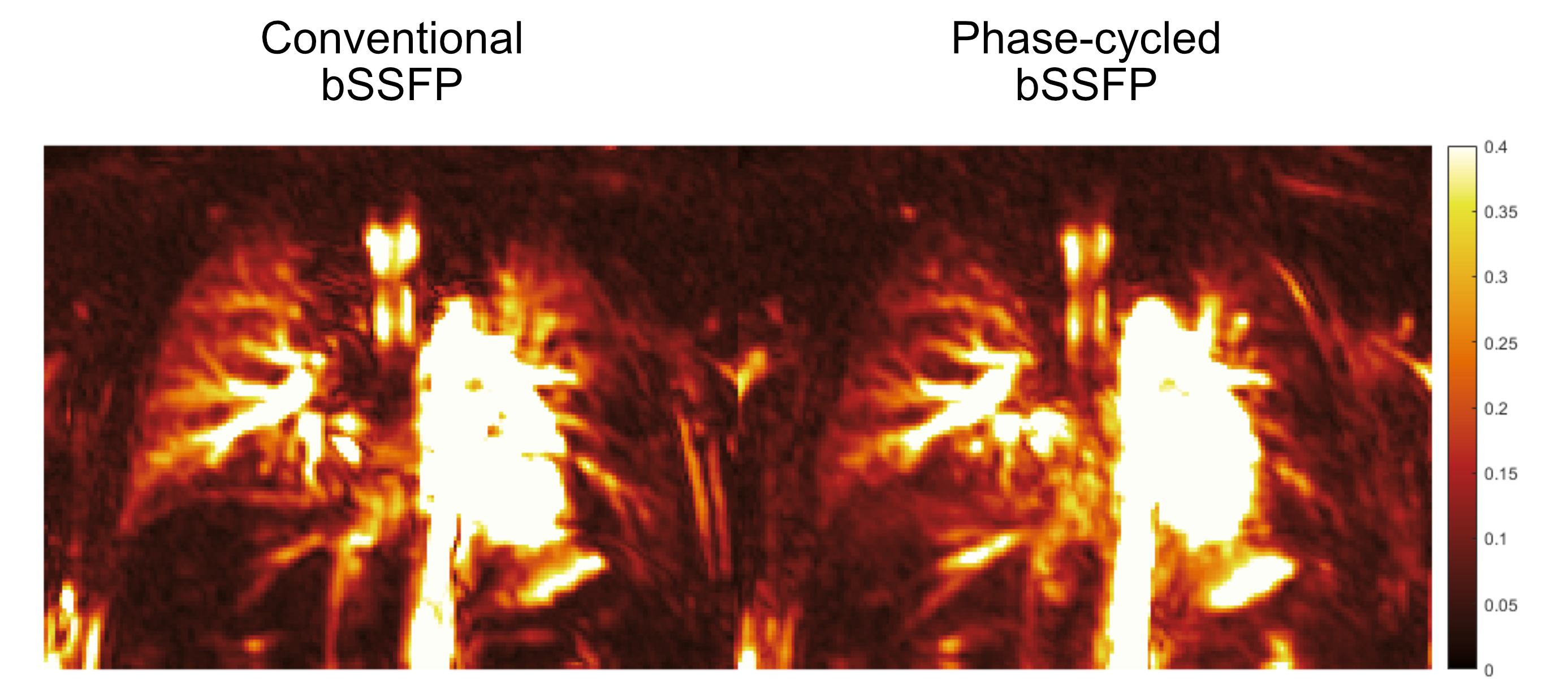
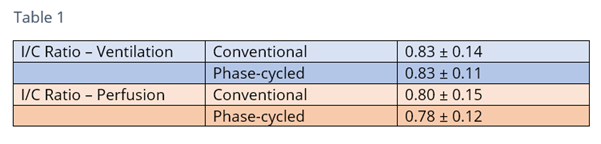
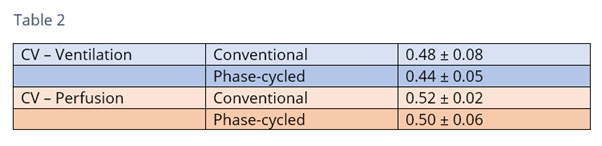
Figure 1 displays magnitude images and functional maps acquired from individual phases of the phase-cycled bSSFP acquisition in a patient with a left-sided hernia. In all patients and individual phase cycle groups, we were able to successfully capture signal variations arising from respiration and cardiac pulsation. Fractional ventilation and normalized perfusion maps obtained from the combination of individual groups are displayed in Figure 2 and Figure 3 for a patient with left-sided hernia. Notice that phase-cycled acquisition displays improved robustness against artificially heightened ventilation results (arrows) owing to its robustness against banding artifacts, and overall shows more homogeneous ventilation results across the parenchyma.Table 1 lists ipsilateral to contralateral lung (I/C) ratios for ventilation and perfusion results obtained using conventional and phase-cycled bSSFP acquisitions, and Table 2 lists the CV results obtained within the ROIs. Notice that both techniques yield similar mean ratio values across the same patients, yet phase-cycled acquisitions yield lower CV indicating improved functional map homogeneity.
Discussion
Although improved image quality was noted in the combined ventilation maps of phase-cycled bSSFP, signal intensities in the combined perfusion maps decreased, possibly due to phases with less favorable perfusion information. However, investigating various phase cycles and their combinations was not within the study's scope. Moreover, it is important to note that phase-cycled acquisitions inherently contain the same information as the conventional bSSFP acquisitions, albeit with fewer number of measurements. Lastly, our study was limited to a small sample size and further studies with larger cohorts are warranted. Nevertheless, these preliminary findings indicate that phase-cycled bSSFP acquisitions may be useful for functional lung imaging in pediatric patients.Conclusion
Here, we have investigated the use of phase-cycled bSSFP acquisitions for functional lung imaging in 2-year-old CDH patients at 1.5T field strength. In all patients, functional maps were successfully obtained. More importantly, with phase-cycled bSSFP we observed improved robustness against banding artifacts compared to the conventional bSSFP, and also a trend towards more homogeneous ventilation maps as reflected by the lower CV values.Acknowledgements
The authors would like to thank Dr. Greta Thater and Dr. Meike Weis for their help with various aspects of this research. This work was supported by Deutsche Forschungsgemeinschaft (grant number: DFG 397806429).References
1. Oluyomi-Obi T, Van Mieghem T, Ryan G (2017) Fetal imaging and therapy for CDH—Current status. Semin Pediatr Surg 26:140–146. https://doi.org/10.1053/j.sempedsurg.2017.04.002
2. Weidner M, Zöllner FG, Hagelstein C, et al (2014) High temporal versus high spatial resolution in MR quantitative pulmonary perfusion imaging of two-year old children after congenital diaphragmatic hernia repair. Eur Radiol 24:2427–2434.
3. Weis M, Sommer V, Zöllner FG, et al (2016) Region of interest-based versus whole-lung segmentation-based approach for MR lung perfusion quantification in 2-year-old children after congenital diaphragmatic hernia repair. Eur Radiol 26:4231–4238. https://doi.org/10.1007/s00330-016-4330-6
4. Groß V, Zahn K, Maurer K, et al (2021) MR lung perfusion measurements in adolescents after congenital diaphragmatic hernia: correlation with spirometric lung function tests. Eur Radiol. https://doi.org/10.1007/s00330-021-08315-9
5. Edelman RR, Koktzoglou I (2019) Noncontrast MR angiography: An update. J Magn Reson Imaging 49:355–373. https://doi.org/10.1002/jmri.26288
6. Ilicak
E, Thater G, Ozdemir S, et al (2023) Functional lung imaging of 2-year-old children aftercongenital diaphragmatic hernia repair using dynamic mode decomposition MRI. Eur Radiol. https://doi.org/10.1007/s00330-023-10335-6.
7. Bauman G, Puderbach M, Deimling M, et al (2009) Non-contrast-enhanced perfusion and ventilation assessment of the human lung by means of fourier decomposition in proton MRI. Magn Reson Med 62:656–664. https://doi.org/10.1002/mrm.22031
8. Ilicak E, Ozdemir S, Schad LR, et al (2022) Phase‐cycled balanced SSFP imaging for non‐contrast‐enhanced functional lung imaging. Magn Reson Med 88:1764–1774. https://doi.org/10.1002/mrm.29302
9. Chefd’Hotel C, Hermosillo G, Faugeras O (2001) A variational approach to multi-modal image matching. In: Proceedings IEEE Workshop on Variational and Level Set Methods in Computer Vision. IEEE Computer Soc, pp 21–28
10. Ilicak E, Ozdemir S, Zapp J, et al (2023) Dynamic mode decomposition of dynamic MRI for assessment of pulmonary ventilation and perfusion. Magn Reson Med 90:761–769. https://doi.org/10.1002/mrm.29656
Figures