0291
Multiorgan quantitative abdominal MRI in paediatric patients with Cystic Fibrosis1Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom, 2NIHR Nottingham Biomedical Research Centre, Nottingham, United Kingdom, 3Population and Lifespan Sciences, University of Nottingham, Nottingham, United Kingdom, 4Translational Medical Sciences, University of Nottingham, Nottingham, United Kingdom
Synopsis
Keywords: Body, Pediatric, liver, pancreas, spleen
Motivation: Cystic fibrosis (CF) is a multi-system, life-limiting genetic disorder. There is a need for multiorgan assessment in children with CF and the response to modulator therapies.
Goal(s): To perform multiorgan MRI in children to quantify lung, liver, pancreas, spleen, and gut function.
Approach: 8 children with CF and 3 healthy volunteers (HV) performed the protocol including quantitative assessment (T1, T2, T2*, fat fraction (FF), stiffness) of liver, pancreas and spleen.
Results: Increased pancreas FF, T1 and T2, spleen T1 and hepatic arterial velocity in CF compared to HVs. Increased liver T1, T2 and stiffness in a CF child independently diagnosed with liver disease.
Impact: This protocol will be used to study the effect of the Cystic Fibrosis Transmembrane Regulator Modulator therapy in children on liver toxicity, pancreas and gut function, and lung health, by performing MRI before and 12 months after commencement of Kaftrio.
Introduction
Cystic fibrosis (CF) is a multi-system, life-limiting autosomal recessive genetic disorder which causes mucus to build-up in certain organs, such as the lungs, liver, pancreas, and intestines. Cystic Fibrosis Transmembrane Regulator (CFTR) Modulator therapies target multiple organ systems, and modulators have maximal benefit when commenced in early childhood. There is a need for multisystem assessment of beneficial as well as potential adverse effects of modulators in children. Here, we develop a multi-organ MRI protocol (the GIFT protocol) designed to be tolerable for children aged 6 to 11 years to quantify measures of lung, liver, spleen, pancreas and gut function for future use to study the effects of CFTR therapies. This abstract presents results on the abdominal (liver, pancreas and spleen) component.Methods
Study protocol8 children with CF (aged 9±2 years) and 3 healthy volunteers (HV) (aged 9±3 years) were recruited (https://clinicaltrials.gov/study/NCT05699148). The study day consisted of a fasted gut MRI (small bowel water content and gut motility) [1] followed by abdominal (liver, pancreas and spleen) MRI acquired in 20-minutes. Subjects then had a set breakfast, with a gut and lung scan (lung UTE and PREFUL) collected at 240-minutes after breakfast, followed by a second set meal and a gut scan 300-minutes post breakfast. All scans were acquired on a Philips 3T Ingenia scanner using a 16-channel anterior coil with paediatric coil holder. Children undertook the scanning protocol without sedation.
Abdominal MRI measures collected included a breath hold mDIXON-Quant sequence to assess organ volume and fat fraction (FF). A fat suppressed respiratory triggered spin-echo echo-planar-imaging (SE-EPI) inversion recovery technique with 15 inversion times (100-1500ms, ascend/descend acquisition) to assess organ tissue T1 in ~3 minutes (3x3x8mm3 voxel size, 9 axial slices). A breath hold multi-echo (mFFE) sequence was used to collect T2* data (10s,12 echoes, TE1=2.35ms,ΔTE=2.35ms,3x3x8mm3,9 axial slices). T2 data were collected using a respiratory triggered GraSE sequence with 30 echoes (TE1=5.6ms,ΔTE=5.6ms,3x3x8mm3, 9 axial slices). Phase contrast MRI (PC-MRI) assessed blood flow through the superior mesenteric artery (SMA), hepatic artery (HA) and portal vein (PV) (velocity encoding: 140, 100 and 50cm/s respectively,1x1x6mm3) to monitor for CF related liver disease and portal hypertension [2]. Liver MR elastography (MRE) was collected using a QIBA recommended SE-EPI sequence with 4 axial slices, 4 phase offsets and 60Hz vibration frequency [3].
Data Analysis
mDIXON FF, T2, T2*, and MRE stiffness maps were scanner computed. T1 data were fit voxel-wise to compute T1 maps (MATLAB). A manual ROI was drawn of the liver, spleen and pancreas from the mDIXON images and used to compute organ volume. This ROI was then used to interrogate the quantitative maps with histogram analysis performed to compute the mode of a fitted gaussian. PC-MRI data was analyzed in Philips Q-flow software to compute flow, mean velocity and mean cross sectional area.
Statistical Analysis
Data were Shapiro-Wilk normality tested, and an unpaired t-test or Mann-Whitney test used to compare the two groups. Data is reported as mean±standard deviation or median (interquartile range).
Results
Figure 1 shows the MRI scan protocol, and an example abdominal T1, T2, T2*, stiffness, and FF maps from a child with CF compared to an age-matched healthy child are shown in Figure 2. Liver tissue T1, T2, T2*, stiffness, FF and volume were comparable between children with CF and HVs, Figure 3, but note outlier values in 1 CF child who was independently being reviewed for CF-related liver disease. For the pancreas, there was a trend for higher FF in CF (CF=6.3(78)%, HV=0.9(2)%, p=0.09), with 3 CF children having partial or complete replacement by fat tissue, Figure 4A. There was also a significant increase in pancreas T1 (CF=1166(494)ms, HV=736(228)ms, p<0.004) and T2 (CF=111±32ms HV=59.9±5.9ms, p<0.002). There was a trend for an increase in spleen tissue T1 in CF (CF=1418±40ms, HV=1381±24ms, p=0.05), Figure 4B. No difference was observed in SMA or PV flow but there was a significant increase in hepatic artery velocity in CF (CF=13.1±6.4cm/s, HV=8.2±1.5cm/s, p<0.04).Discussion
We have demonstrated the feasibility of acquiring a multiorgan multiparametric quantitative MRI protocol in children. Differences in liver, pancreas and spleen MRI measures in CF compared to HVs were seen in the spleen and pancreas, alongside liver changes in a CF child who was independently diagnosed with liver disease. HV T1 measures agree with literature paediatric values [4], and we plan to collect more HV data.Conclusion
Following this baseline feasibility, we are now studying the effect of CFTR therapy on lung, gut, liver, pancreas and spleen function by scanning these children with CF 12-months after commencement of Kaftrio.Acknowledgements
Study funded by grants from Vertex Ltd, Nottingham University Hospitals Charity, the MRC Confidence in Concept Programme, and the Nottingham NIHR Biomedical Research Centre
References
1. Dellschaft NS, Ng C, Hoad C, et al (2022) Magnetic resonance imaging of the gastrointestinal tract shows reduced small bowel motility and altered chyme in cystic fibrosis compared to controls. Journal of Cystic Fibrosis 21:502–505. https://doi.org/10.1016/J.JCF.2021.12.007
2. Palaniyappan N, Cox E, Bradley C, et al (2016) Non-invasive assessment of portal hypertension using quantitative magnetic resonance imaging. J Hepatol 65:. https://doi.org/10.1016/j.jhep.2016.07.021
3. Quantitative Imaging Biomarkers Alliance (2017) QIBA Profile: Magnetic Resonance Elastography of the Liver. 1–65
4. Gilligan LA, Dillman JR, Tkach JA, et al (2019) Magnetic resonance imaging T1 relaxation times for the liver, pancreas and spleen in healthy children at 1.5 and 3 tesla. Pediatr Radiol 49:1018–1024. https://doi.org/10.1007/S00247-019-04411-7
Figures
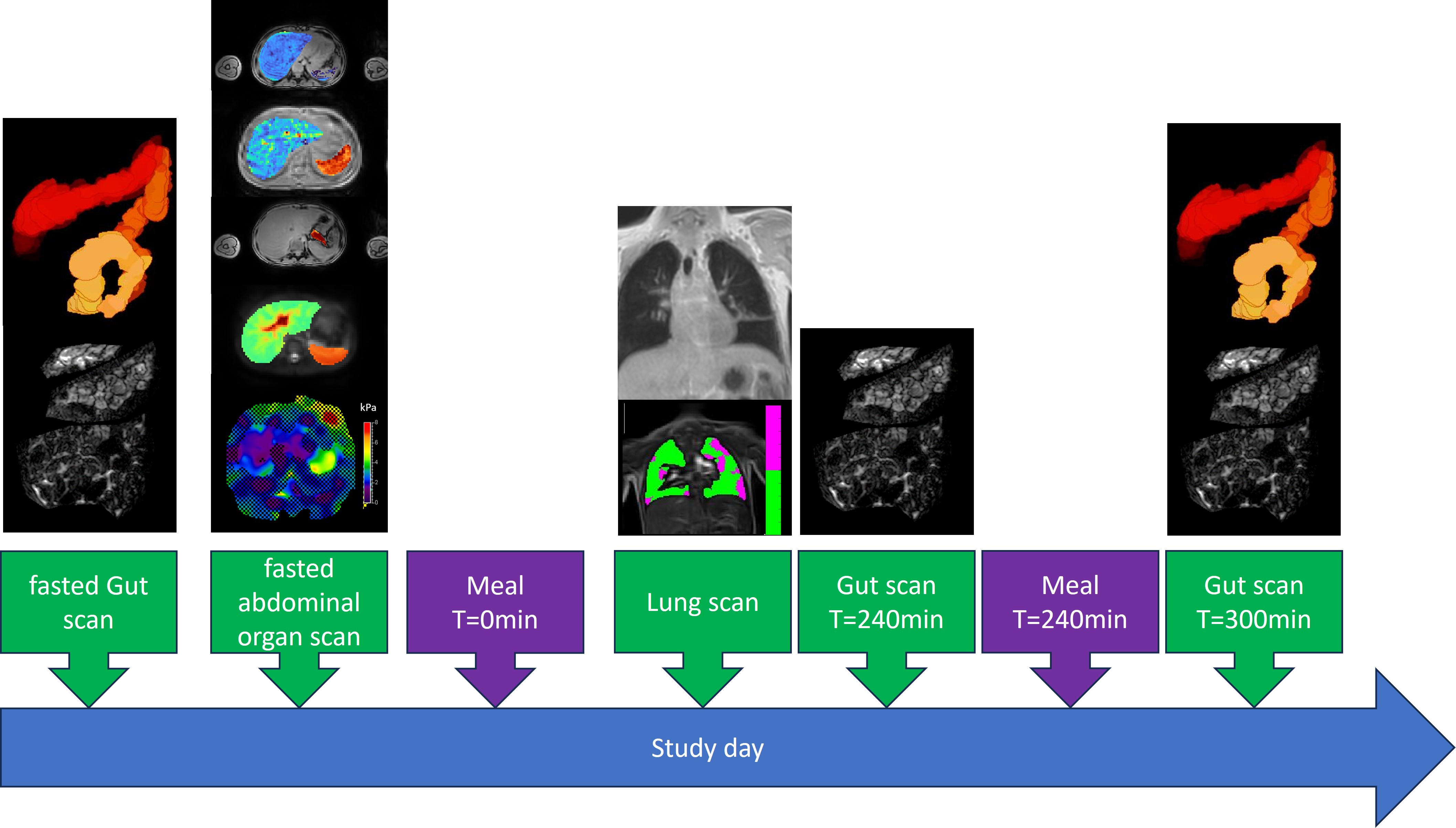
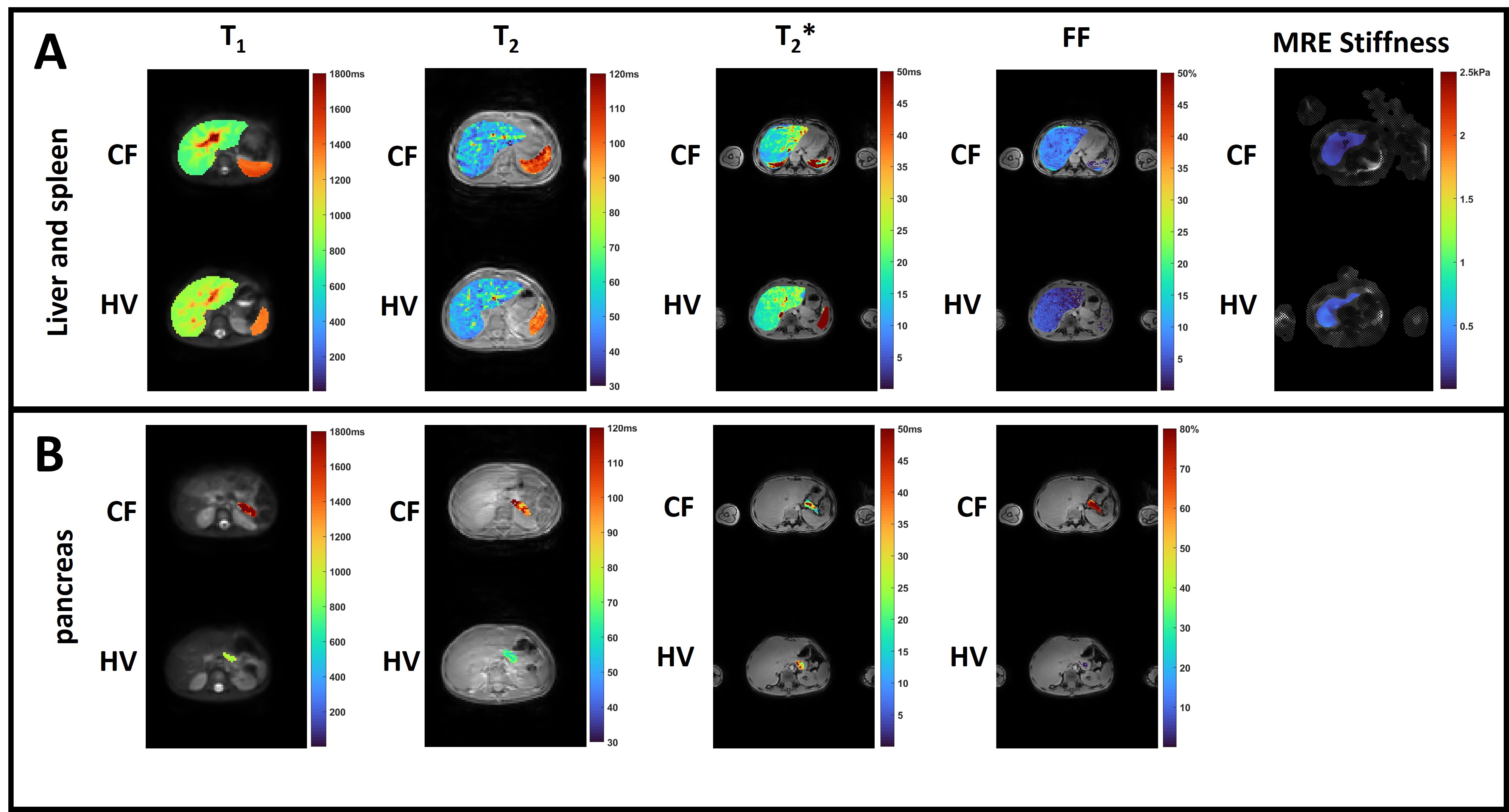
Figure 2: Example abdominal T1, T2, T2*, FF and MRE stiffness maps for A) liver and spleen and B) pancreas in a child with cystic fibrosis (CF) and age-matched healthy child (HV).
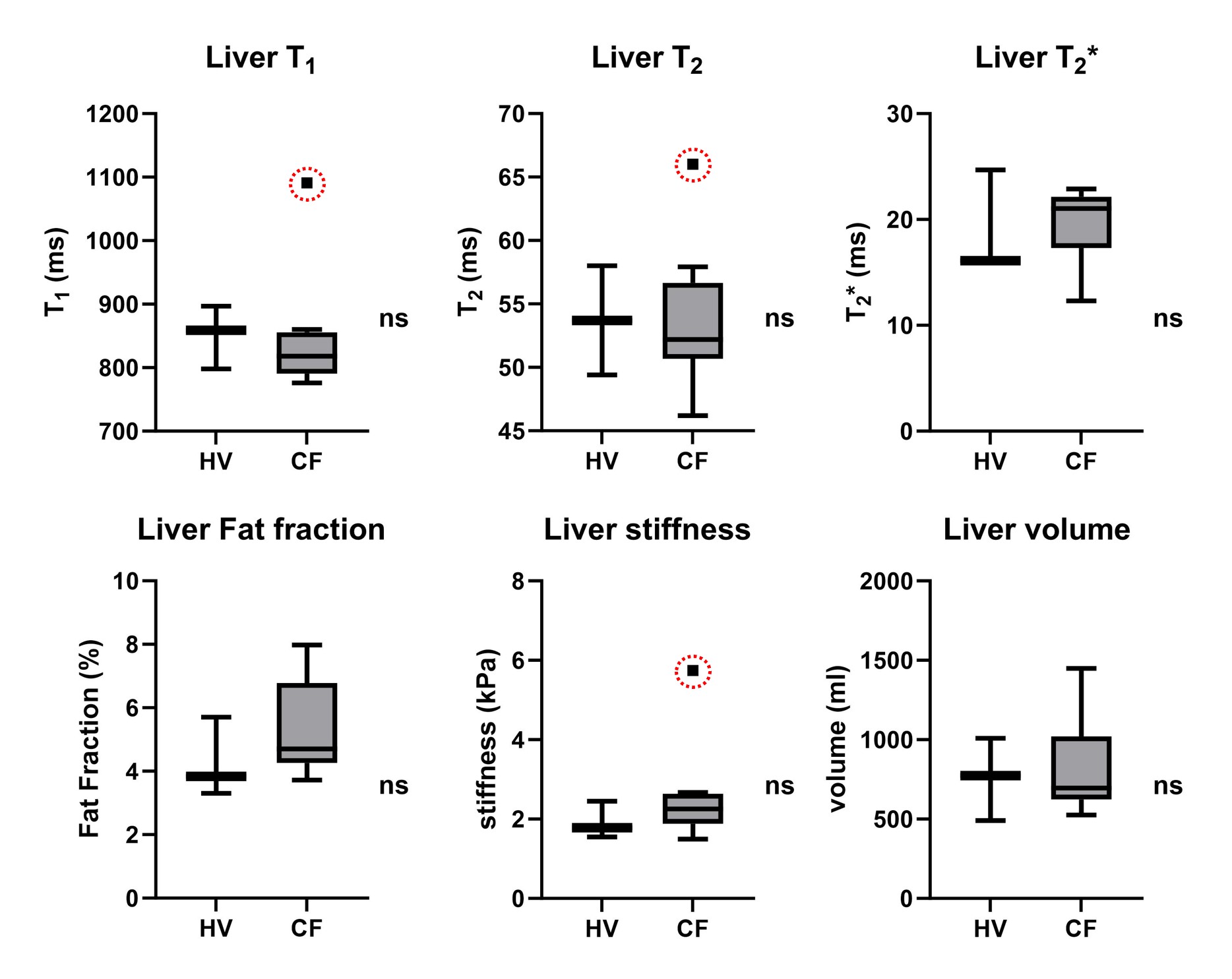
Figure 3: Liver tissue T1, T2, T2*, FF, MRE stiffness, and volume in HV and CF. Note an outlier in the CF group with high T1, T2, and MRE stiffness values, with this child found to have CF-related liver disease.
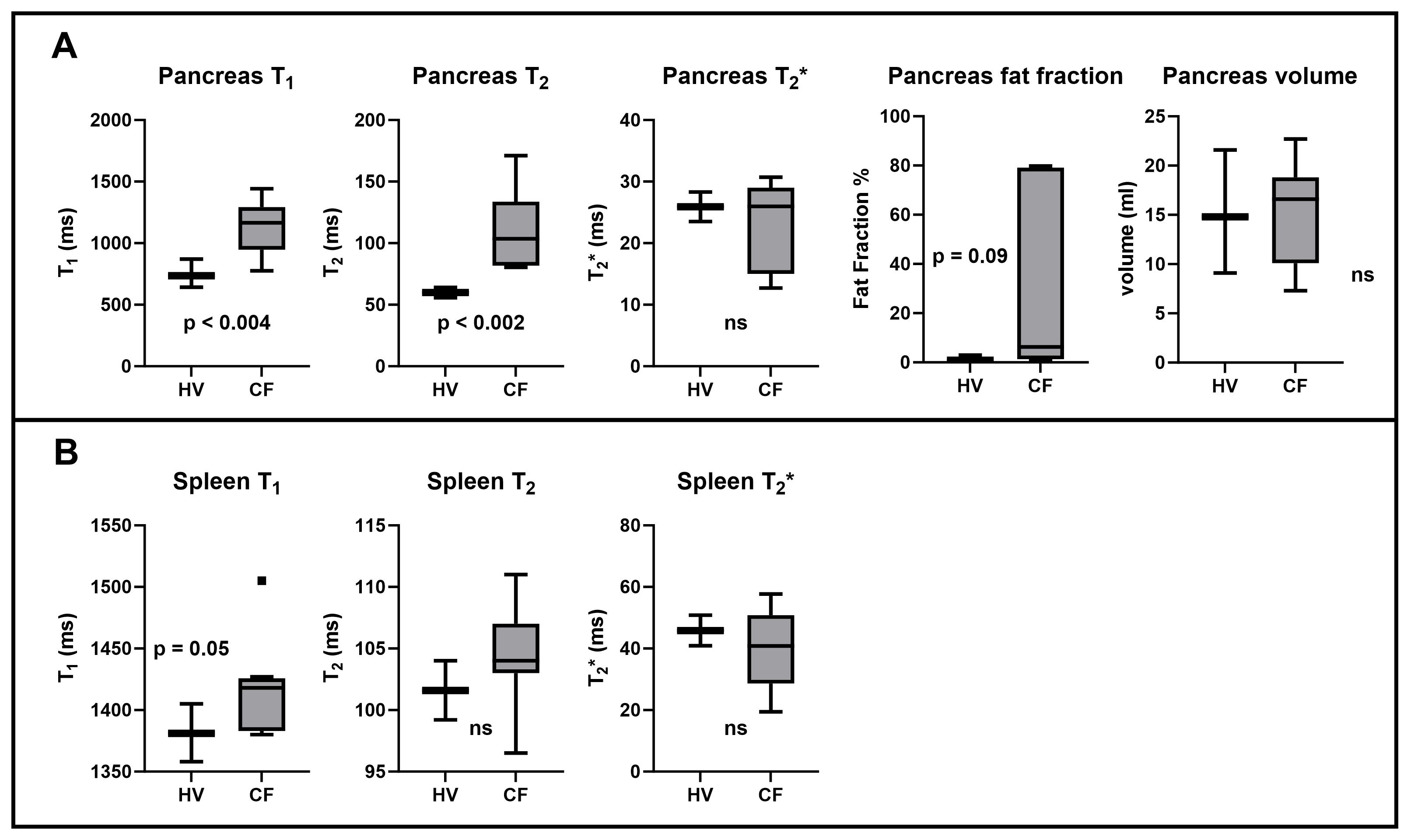
Figure 4: A) Pancreas measures which shows in CF compared to HV a significant increase in T1 (CF 1166(494)ms, HV 736(228)ms, p<0.004) and T2 (CF 111±32ms HV 59.9±5.9ms, p<0.002), and a trend for an increase in fat fraction (CF = 6.3(78)%, HV = 0.9(2)%, p = 0.09). B) Spleen measures shows a trend for an increase in spleen tissue T1 in CF (CF 1418±40ms, HV 1381±24ms, p=0.05).
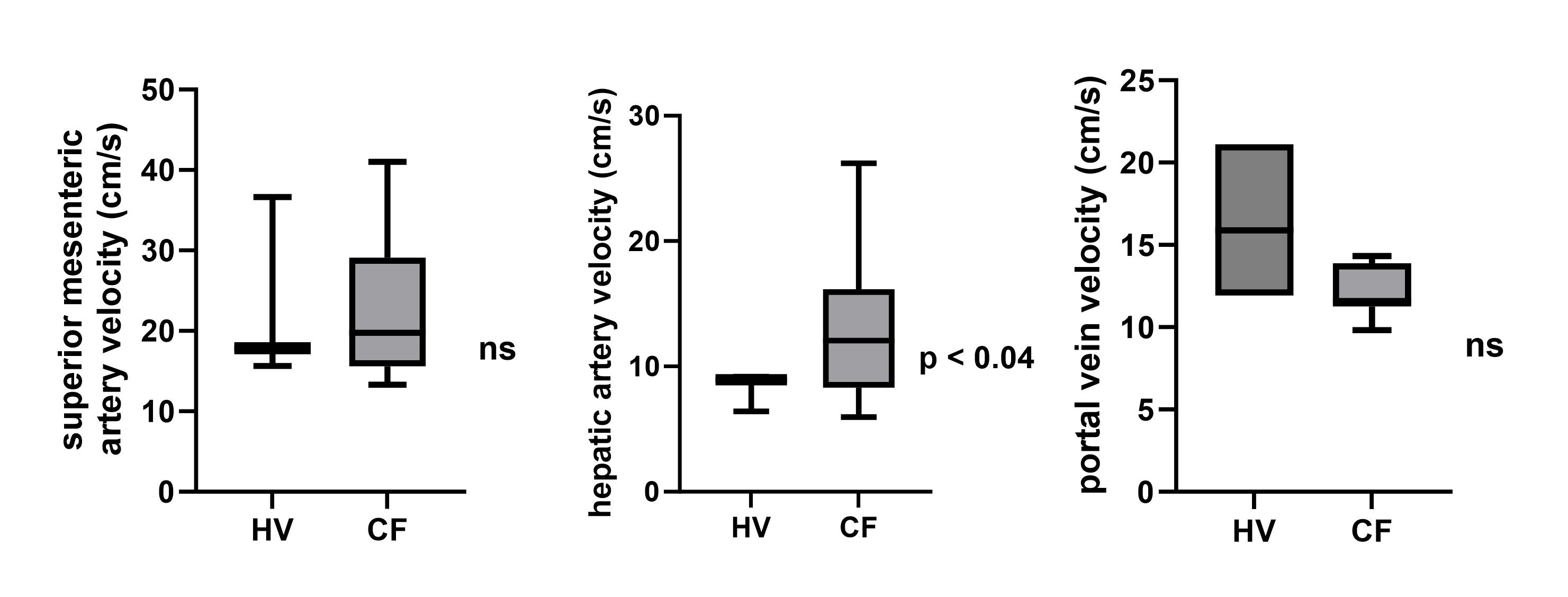
Figure 5: PC-MRI mean velocity measures which shows a significant increase in the hepatic artery in CF (CF 13.1±6.4cm/s, HV 8.2±1.5cm/s, p<0.04), but no difference in the SMA or portal vein.