0289
Trajectories of abdominal subcutaneous and visceral adipose tissue accumulation and cardiometabolic health in children: The GUSTO study1Singapore Institute for Clinical Sciences, A*STAR, Singapore, Singapore, 2Bioinformatics Institute, A*STAR, Singapore, Singapore, 3Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 4Department of Pediatric Endocrinology, KK Women’s and Children’s Hospital, Singapore, Singapore, 5Duke-National University of Singapore Graduate Medical School, Singapore, Singapore, 6Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore, 7Department of Maternal Fetal Medicine, KK Women's and Children's Hospital, Singapore, Singapore, 8MRC Lifecourse Epidemiology Centre & NIHR Southampton Biomedical Research Centre, University of Southampton & University Hospital Southampton NHS Foundation Trust, Southampton, United Kingdom, 9Centre for Human Evolution, Adaptation and Disease, Liggins Institute, University of Auckland, Auckland, New Zealand, 10Department of Obstetrics and Gynaecology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 11Sheffield Institute for Translational Neuroscience, University of Sheffield, Sheffield, United Kingdom, 12Department of Computer Science, University of Sheffield, Sheffield, United Kingdom, 13National Heart and Lung Institute, Imperial College London, London, United Kingdom, 14Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, Singapore, 15Department of Paediatrics, Khoo Teck Puat-National University Children’s Medical Institute, National University Health System, Singapore, Singapore, 16Department of Diagnostic and Interventional Imaging, KK Women’s and Children’s Hospital, Singapore, Singapore, 17Human Potential Translational Research Programme, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore, 18Department of General Practice and Primary Health Care, University of Helsinki and Helsinki University Hospital, Helsinki, Finland, 19Folkhälsan Research Center, Helsinki, Finland, 20Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
Synopsis
Keywords: Body, Body, Pediatrics, abdominal adipose tissue, subcutaneous and visceral fat, insulin resistance
Motivation: Unravel the links between childhood abdominal fat distribution patterns and subsequent cardiometabolic risks aiming to provide effective strategies for preventing childhood obesity.
Goal(s): To investigate the presence of distinct abdominal fat accumulation patterns during infancy and childhood in a multi-ethnic cohort, and their associations with cardiometabolic risk.
Approach: Latent class growth mixture modeling was used to identify three trajectories (stable, slow acceleration, rapid acceleration) for deep subcutaneous (DSAT), superficial subcutaneous (SSAT), and visceral adipose tissues (VAT).
Results: Compared to Chinese children, Indian children had higher odds of being in the rapid acceleration trajectory. All accelerated trajectories were associated with inflammatory marker, hsCRP.
Impact: This research has the potential to impact public health by providing evidence-based insights into the relationships between abdominal fat distribution patterns and cardiometabolic health. Our findings may aid development of targeted interventions and strategies to mitigate long-term adverse cardiometabolic consequences.
Introduction
Accelerated growth patterns in infancy and early childhood have been associated with an increased susceptibility to obesity and cardiometabolic risks in adulthood1,2. The assessment of childhood growth patterns, often evaluated through trajectories of gross adiposity measures such as body mass index (BMI) has been an invaluable tool in understanding developmental trends and the complexities of childhood obesity3. However, BMI provides a crude measure of whole-body adiposity and does not discern fat distribution among different adipose tissue depots. Within the abdominal region, the distribution of adipose tissue is not homogenous, and distinct depots, including deep subcutaneous (DSAT), superficial subcutaneous (SSAT), and visceral adipose tissue (VAT), exhibit different functional characteristics and distinct associations with metabolic risks4,5. In a multi-ethnic cohort of children in Singapore, we aimed to investigate if differential abdominal fat accumulation patterns exist in infancy and childhood and if they have different associations with cardiometabolic risk factors during adolescence.Methods
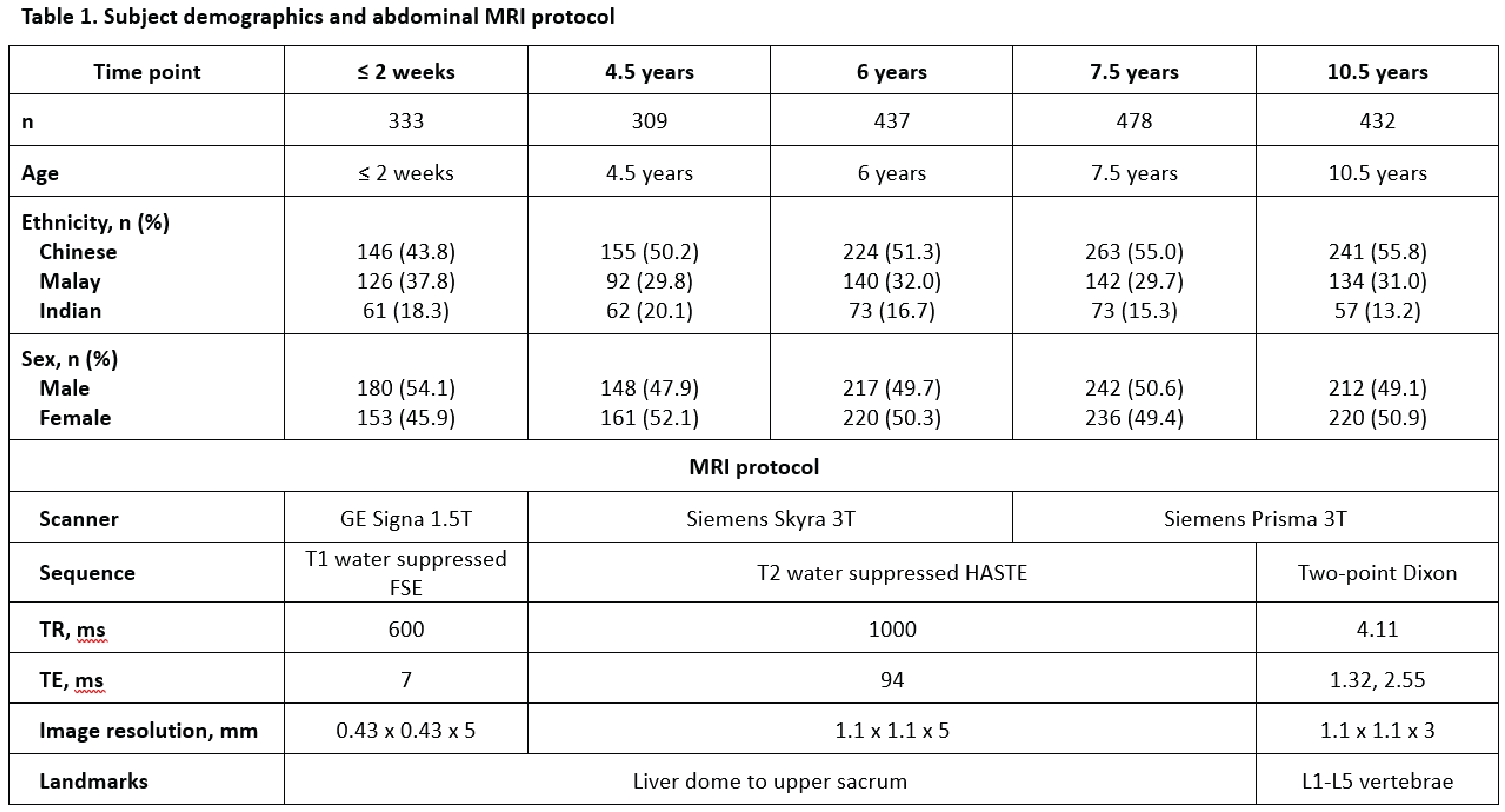
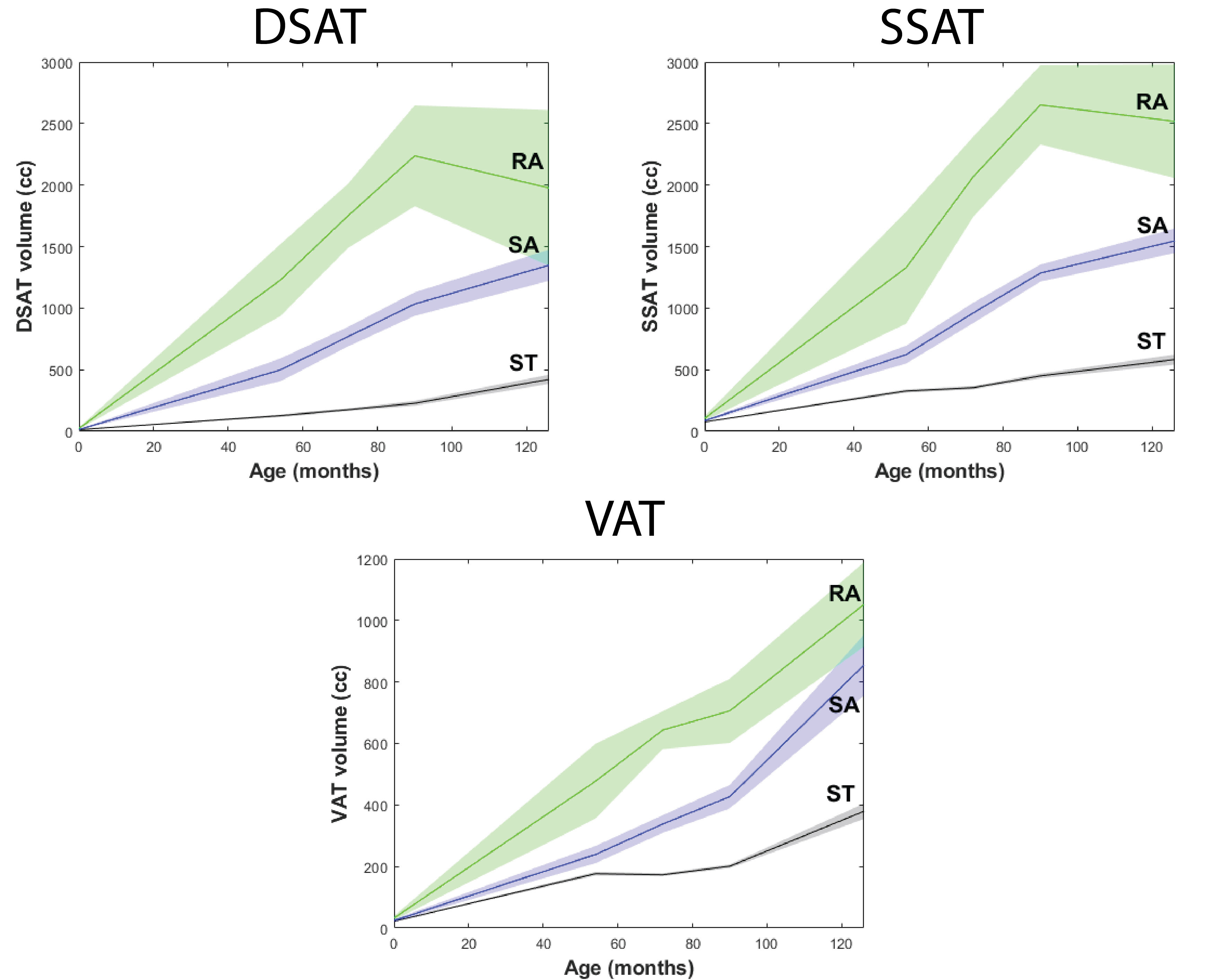
Data from children were analysed from the Growing Up in Singapore Towards healthy Outcomes (GUSTO) cohort6. Serial measures of MRI-based abdominal fat depot volumes from the children at ≤ 2 weeks after birth (n=333), 4.5 years (n=309), 6 years (n=437), 7.5 years (n=478), and 10.5 years (n=432) were used (Table 1). A deep learning-based segmentation technique was used to segment and quantify abdominal MRI into deep subcutaneous (DSAT), superficial subcutaneous (SSAT), and visceral adipose tissue (VAT) depots7. Latent class growth mixture modeling (LCGMM) was used to identify the trajectory patterns of DSAT, SSAT, and VAT from all subjects (n=397) who had MRI data from at least 3 time points (Fig. 1)8. To account for underlying quadratic shapes of trajectories intercepts, slopes, and curvatures were considered, and full information maximum likelihood was used to address missing values. The criteria for classification were based on entropy, Bayesian information criterion, posterior probability, replication of log likelihood ratio corresponding to best solutions, and non-overlapping 95% confidence intervals of mean trajectory patterns. At age 10 years, glucose, insulin, triglycerides, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, and high sensitivity C-reactive protein (hsCRP) were measured from fasting plasma. Homeostasis model assessment of insulin resistance (HOMA2-IR) was determined using the HOMA2 calculator9. We examined the associations of the trajectory patterns with metabolic markers using multiple linear regression models with adjustment for ethnicity, maternal educational attainment, sex, maternal age at recruitment, parity, prepregnancy BMI, fasting plasma glucose at gestational week 26, gestational weight gain, and birth weight.Results
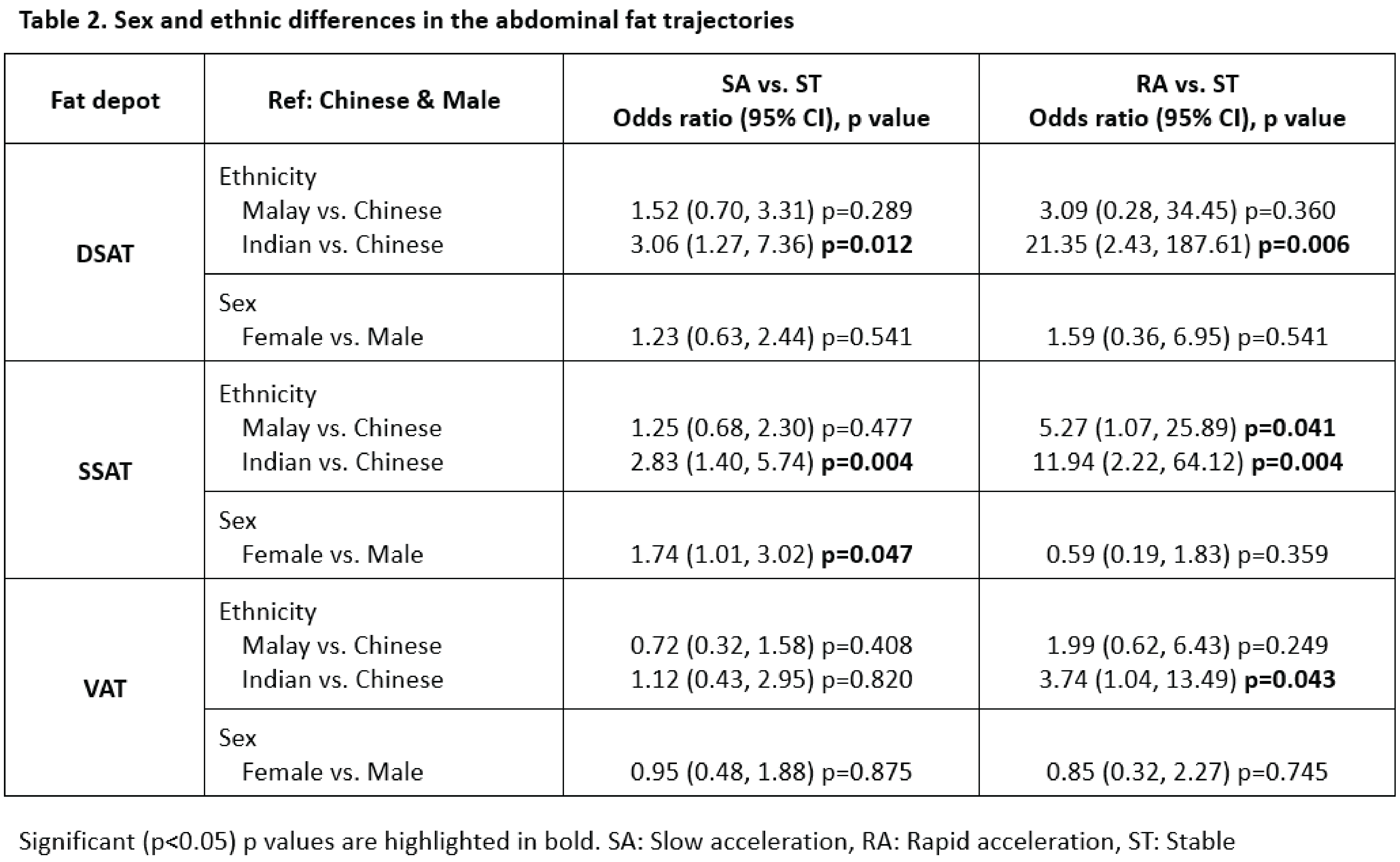
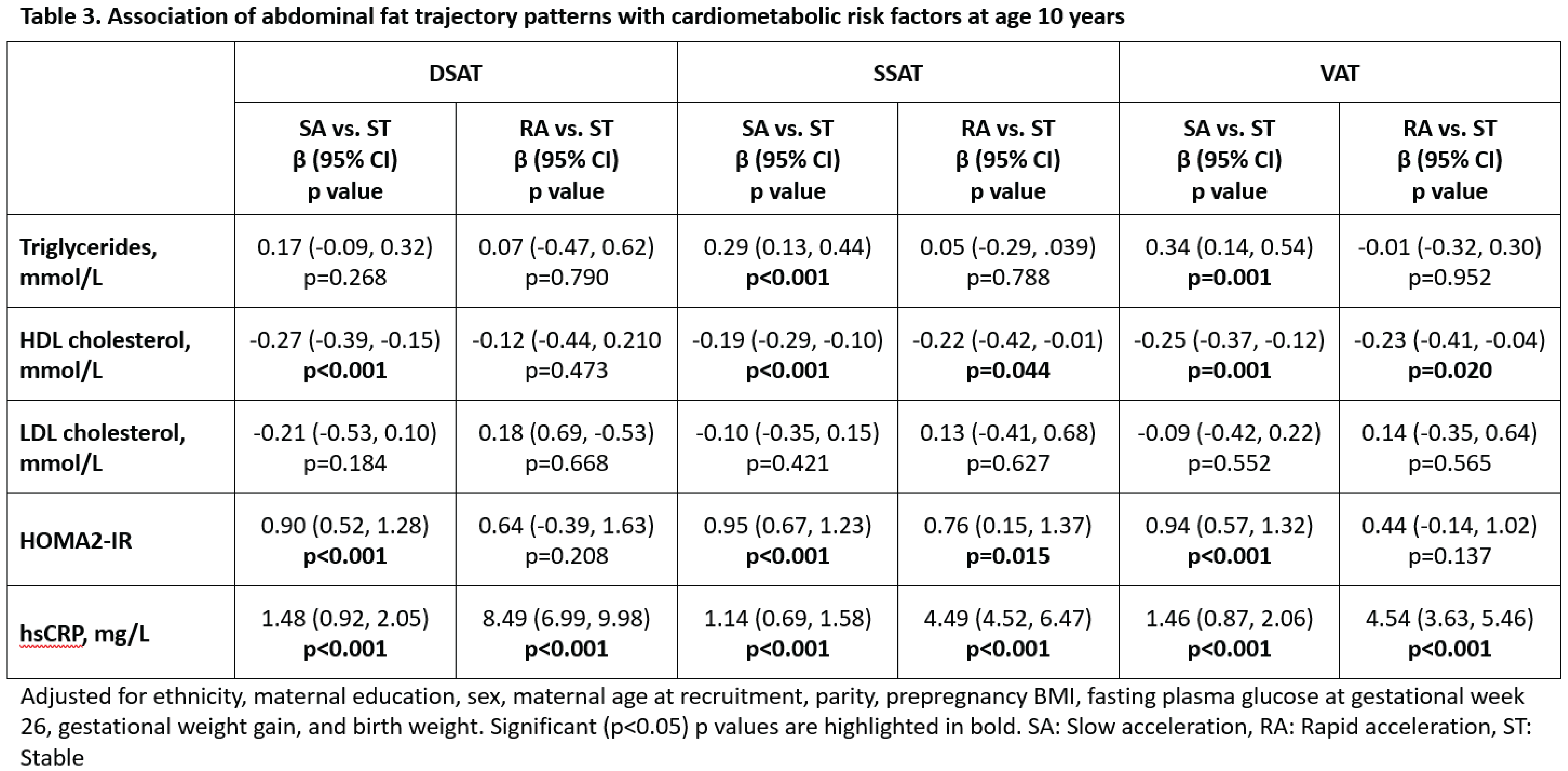
We identified three trajectory patterns for DSAT, SSAT, and VAT and classified them as Stable (ST), Slow Acceleration (SA), and Rapid Acceleration (RA) (Fig 1). Compared to Chinese children, Indian children had higher odds of being in the RA trajectory for DSAT, SSAT, and VAT. For the subcutaneous depots (DSAT and SSAT), Indian ethnicity was also associated with the SA trajectory (Table 2). For SSAT, Malay ethnicity was associated with the RA trajectory. Girls had about 75% higher odds of belonging to the SA trajectory of SSAT. No sex differences were identified among the other trajectory classes. SA trajectories of SSAT and VAT were linked to elevated levels of triglycerides (Table 3). SA trajectories of all depots and RA trajectory of SSAT were associated with increased HOMA2-IR and reduced HDL-cholesterol. SA and RA trajectories of all fat depots were associated with the inflammatory marker, hsCRP.Conclusions
Analysis of dynamic fat accumulation patterns during early childhood revealed unique trajectories of abdominal fat deposition, each demonstrating specific links to cardiometabolic health outcomes during adolescence. Our findings highlight the association between Indian ethnicity and accelerated trajectories of fat gain in all three abdominal depots. Understanding the early-life dynamics of these fat depots and their implications for long-term health may aid development of targeted interventions and strategies to mitigate the long-term adverse cardiometabolic consequences associated with childhood fat partitioning.Acknowledgements
This research is supported by the Singapore National Research Foundation under its Translational and Clinical Research (TCR) Flagship Programme and administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC), Singapore (NMRC/TCR/004-NUS/2008; NMRC/TCR/012-NUHS/2014). Additional funding is provided by the Singapore Institute for Clinical Sciences, Agency for Science Technology and Research (A*STAR), Singapore, and Nestec.References
- Eriksson JG, Forsen T, Tuomilehto J, Osmond C, Barker DJ. Early growth and coronary heart disease in later life: longitudinal study. BMJ 2001;322:949-53.
- Geserick M, Vogel M, Gausche R, et al. Acceleration of BMI in early childhood and risk of sustained obesity. New Engl J Med 2018;379:1303-12.
- Michael N, Gupta V, Fogel A, et al. Longitudinal characterization of determinants associated with obesogenic growth patterns in early childhood. Int J Epidemiol 2023;52:426-39.
- Kelley DE, Thaete FL, Troost F, Huwe T, Goodpaster BH. Subdivisions of subcutaneous abdominal adipose tissue and insulin resistance. American Journal of Physiology-Endocrinology And Metabolism 2000;278:E941-E8.
- Lee M-J, Wu Y, Fried SK. Adipose tissue heterogeneity: implication of depot differences in adipose tissue for obesity complications. Mol Aspects Med 2013;34:1-11.
- Soh S-E, Tint MT, Gluckman PD, et al. Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int J Epidemiol 2013;43:1401-9.
- Kway YM, Thirumurugan K, Tint MT, et al. Automated Segmentation of Visceral, Deep Subcutaneous, and Superficial Subcutaneous Adipose Tissue Volumes in MRI of Neonates and Young Children. Radiology: Artificial Intelligence 2021;3:e200304.
- Jung T, Wickrama KA. An introduction to latent class growth analysis and growth mixture modeling. Soc Personal Psychol Compass 2008;2:302-17.
- Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care 2004;27:1487-95.
Figures