0287
Differences in 4D aortic motion derived from 3T bSSFP CMR between Marfan syndrome patients and healthy volunteers1Radiology and Nuclear medicine, Amsterdam University Medical Centers, Amsterdam, Netherlands, 2Amsterdam Cardiovascular Sciences, Amsterdam, Netherlands, 3Cardiology, Amsterdam University Medical Centers, Amsterdam, Netherlands, 4Cardiology, Radboud University Medical Center, Nijmegen, Netherlands, 5University Medical Center Groningen, Groningen, Netherlands
Synopsis
Keywords: Vascular, Blood vessels, Marfan
Motivation: New biomarkers are needed to guide aortic surgery to prevent aortic dissection in Marfan syndrome (MFS).
Goal(s): To investigate differences in aortic motion between healthy volunteers and (subgroups of) MFS patients.
Approach: We apply a recently published novel non-contrast enhanced, free breathing, time-resolved 3D balanced steady free precession CMR scan with a machine learning based algorithm for automatic aortic segmentations to evaluate 4D aortic motion.
Results: We found significant differences in aortic motion between patients with- and without a history of aortic root surgery and healthy volunteers. Thus, aortic motion might be a novel marker for aortic disease severity in MFS.
Impact: The differences in 4D aortic motion measured using 3D CINE balanced steady state free precession CMR between healthy volunteers and (subgroups of) Marfan syndrome patients might provide a new marker for disease severity in Marfan syndrome.
Background
Aortic diameter is currently the only biomarker for elective aortic surgery in Marfan Syndrome (MFS). However, some MFS patients still develop an aortic dissection before reaching this diameter threshold or in an aortic region distal to the operated aortic root. Thus, we need new biomarkers to predict aortic dissections. Abnormal distensibility and motion of the aorta may play a role in aortic growth and dissection. We investigated 4D aortic motion as a potential new biomarker for aortic disease severity in MFS using 4D balanced steady-state free precession (bSSFP) cardiac magnetic resonance imaging (CMR).Methods
57 MFS patients (27 females, aged 35 ± 8.6 years, 31 with a history of aortic root surgery) and 11 healthy volunteers (HV) (7 females, aged 31 ± 8.2 years) underwent imaging of the thoracic aorta using a non-contrast enhanced, free breathing, time-resolved three dimensional (3D) CINE bSSFP sequence with Gaussian shaped RF pulse on an Ingenia 3T MRI scanner (Philips Healthcare, Best, Netherlands)1. PROspective Undersampling in multiple Dimensions (PROUD) with acceleration factor R~10 was used resulting in a scan time of ~4 minutes2. Scan parameters were FOV=256×256-320×70-88mm3 and slice oversampling factor=1.70-2.14, based on aortic geometry; acquired/reconstructed spatiotemporal resolution = 1.6/1.0mm3, ~67ms (15 cardiac phases, [CP]), TR/TE/FA=2.9ms/1.44ms/40°.A previously described nnU-Net was used to automatically segment the thoracic aorta in all CP3. For current analysis, the network was retrained on previously acquired 84 manual segmentations from 14 healthy volunteers and 10 new manual segmentations of randomly selected CP in MFS patient data in the current cohort.
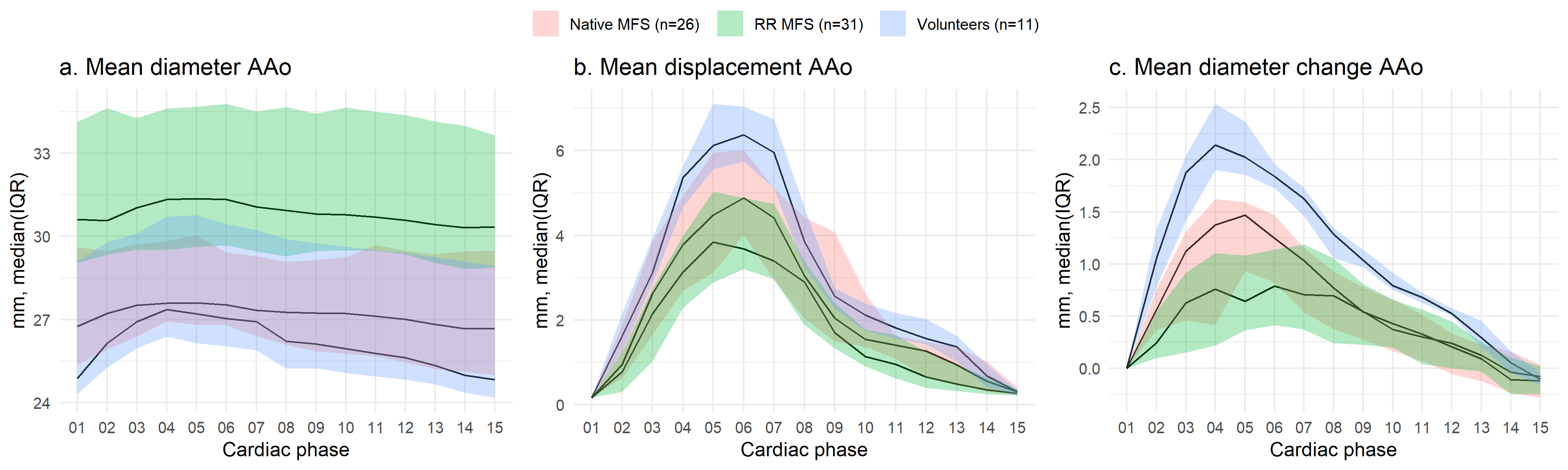
The time-resolved segmentations were used to derive 4D aortic diameter maps4. For analysis, only the ascending aorta (AAo), from the sinotubular junction to the mid-aortic arch, was considered. Mean displacement and diameter change of the AAo were derived using an iterative closest point registration of this single reference end-diastolic phase to all CP4, 5. End-systole was determined by visually assessing the last CP showing left ventricular contraction. Subsequently, CP were grouped for early-systole (1-2), peak-systole (3-4), late-systole (5-6) and diastole (7-15). Figure 1 displays an overview of the entire acquisition and processing pipeline. Additionally, mid-diastolic aortic diameters were manually measured on cross-sections in a clinical 3D mDixon scan (spatial resolution: 1.25x1.25x1.25mm). The Kruskal-Wallis test and Dunn’s test with Bonferroni correction for multiple testing were used to compare differences in median motion parameters per grouped CP for patients with a native aortic root (native MFS), patients with a history of aortic root surgery (RR MFS) and for HV.
Results
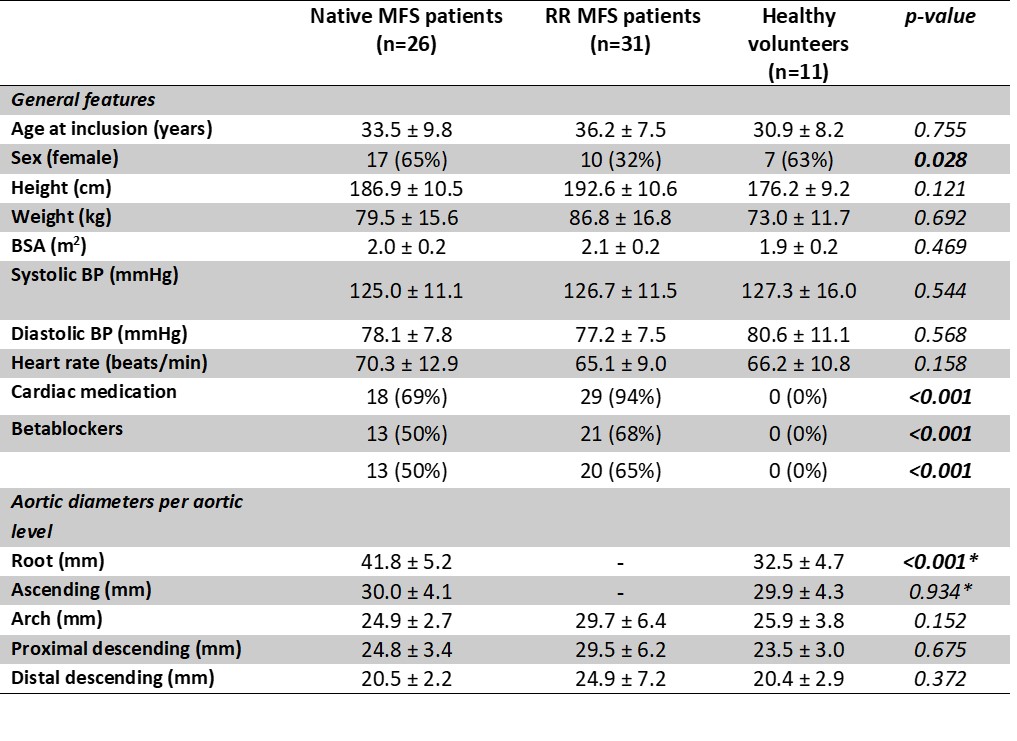
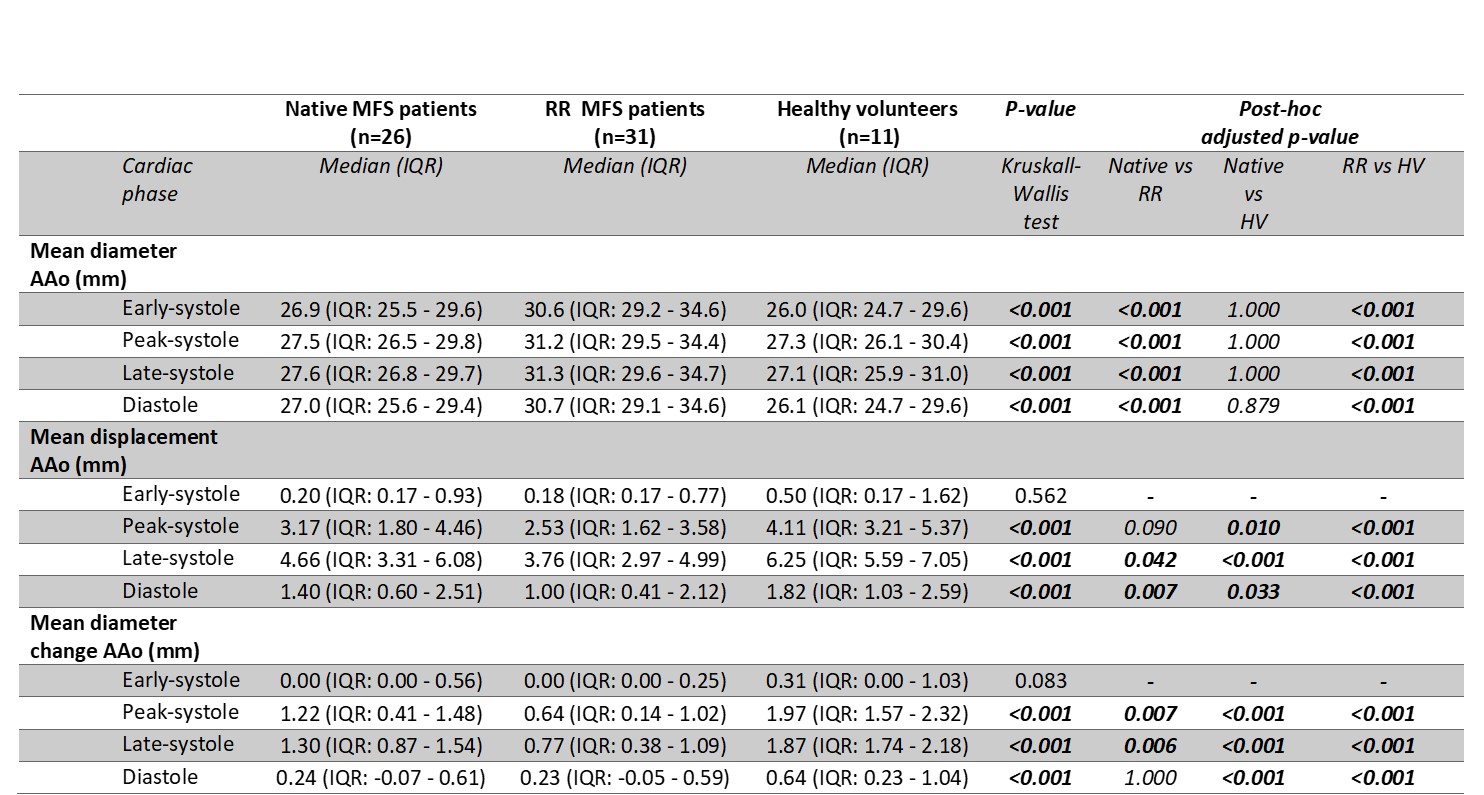
Baseline characteristics are presented in table 1. Typical examples of aortic motion of a HV and a native and a RR MFS patient are displayed in figure 2. Figure 3 shows the mean AAo diameter, diameter change and displacement over the cardiac cycle for MFS patients and HV. All median values +/- IQR are presented in table 2. AAo diameter was significantly larger for RR MFS patients versus native MFS patients and HV. Displacement was significantly larger for HV compared to RR MFS patients and native MFS patients in peak- and late-systole and diastole. Native MFS patients showed higher displacement in peak- and late-systole and diastole compared to RR MFS patients. Mean AAo diameter change was larger for HV versus native and RR MFS patients in peak- and late- systole and in diastole. Furthermore, peak- and late-systole AAo diameter change was larger in native versus RR MFS patients. AAo displacement (mm) was not different for MFS patients on betablockers prescription versus patients without betablockers in any cardiac phase (early-systole: 0.55(IQR: 0.26–0.90) vs 0.54(IQR: 0.36–1.00), p=0.980; peak-systole: 2.82(IQR: 1.87–3.94) vs 3.15(IQR: 2.05–4.10), p=0.41, late-systole: 4.05(IQR: 3.06–5.28) vs 4.42(IQR: 3.54–5.65), p=0.320; and diastole 1.43(IQR: 1.06–1.77) vs 1.78(1.48–2.33), p=0.146. Age was negatively associated with diameter change in late-systole in native MFS patients (rs=-0.508, n=26, p=0.008).Discussion
Pathological changes in the aortic wall in MFS syndrome and presence of a stiff aortic graft seem to result in decreased bulk motion and diameter change in the AAo. Clinical follow-up data is required to assess if this decreased bulk motion can act as an independent marker to identify MFS aortas at high risk of dissection. Furthermore, this work shows potential for future investigation of the stress-strain relationship in the aortic wall by combining aortic movement data, as measurement for strain, with a non-invasive method of measuring arterial pressure, as marker for arterial stress.Conclusion
We showed significant differences in aortic motion during the cardiac cycle between HV, native MFS and RR MFS patients. These findings may be useful for the monitoring of aortic disease in MFS.Acknowledgements
This study is part of the project "Comprehensive assessment of 4D thoracic aorta biomechanics using novel cardiac MRI technology" with project number 18402 of the research programme "Applied and Engineering Sciences", which is partly financed by the Dutch Research Council (NWO).References
1. Merton R, Bosshardt D, Strijkers GJ, Nederveen AJ, Schrauben EM, van Ooij P. Reproducibility of 3D thoracic aortic displacement from 3D cine balanced SSFP at 3 T without contrast enhancement. Magn Reson Med. 2023.
2. Gottwald LM, Peper ES, Zhang Q, Coolen BF, Strijkers GJ, Nederveen AJ, van Ooij P. Pseudo-spiral sampling and compressed sensing reconstruction provides flexibility of temporal resolution in accelerated aortic 4D flow MRI: A comparison with k-t principal component analysis. NMR Biomed. 2020;33(4):e4255.
3. Merton R BD, Strijkers GJ, Nederveen AJ, Schrauben EM, van Ooij P. 4D aortic motion maps from isotropic high-resolution 3D CINE balanced steady state free precession at 3T and automated segmentations. Joint Annual Meeting ISMRM-ESMRMB & ISMRT 32st Annual Meeting; Toronto, Canada2023.
4. van Ooij P, Collins J, Fedak P, Nederveen AJ, Carr JC, Markl M, Barker AJ. 3D Linear Regression Analysis Reveals Relationships of 4D flow MRI-derived Aortic Dimensions with Age, Gender and Wall Shear Stress in Patients with Aortopathy. Honolulu, Hawaii. 2017:288.
5. Audenaert EA, Van Houcke J, Almeida DF, Paelinck L, Peiffer M, Steenackers G, Vandermeulen D. Cascaded statistical shape model based segmentation of the full lower limb in CT. Comput Methods Biomech Biomed Engin. 2019;22(6):644-57.
Figures
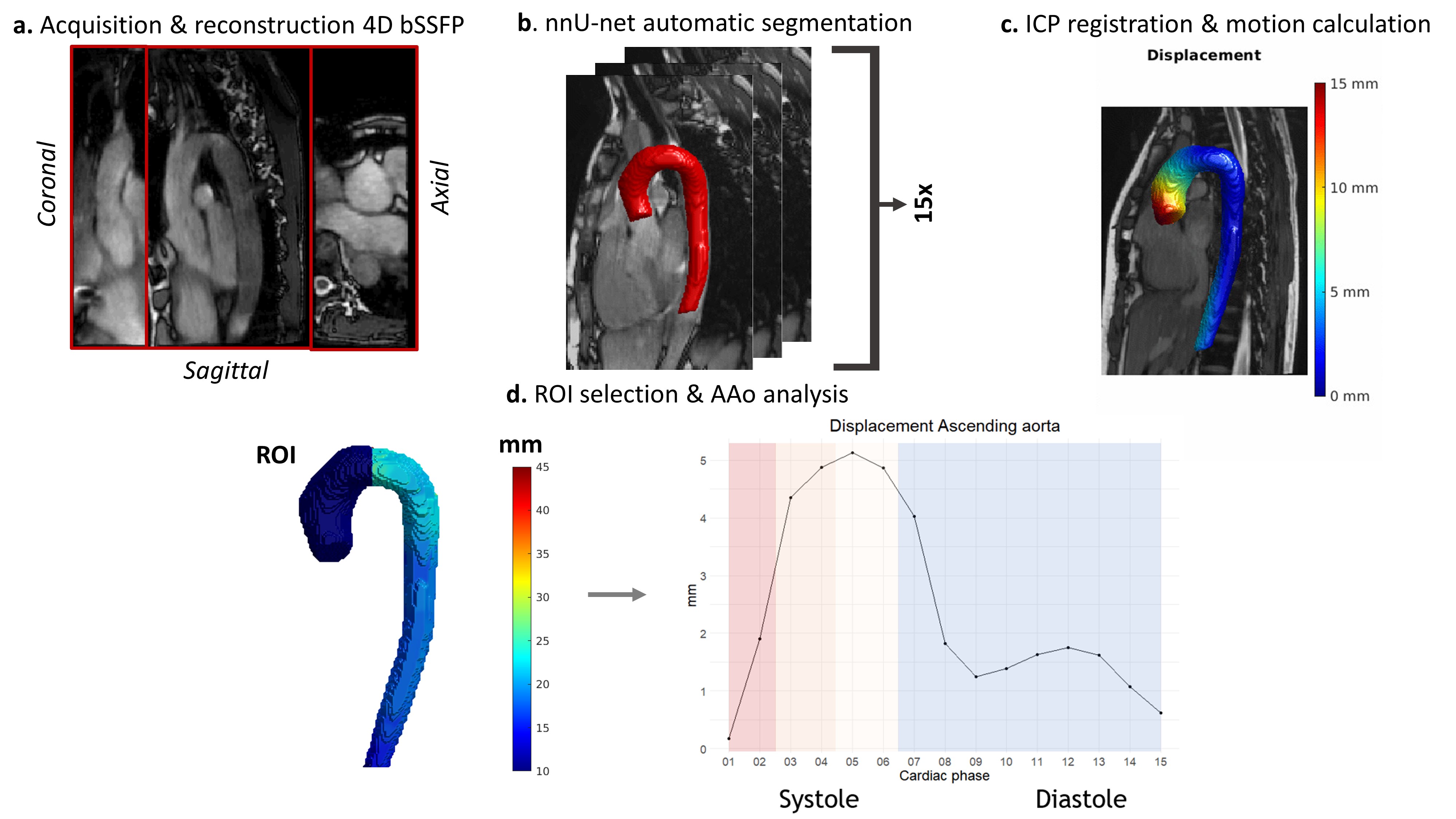
Figure 1. Acquisition and processing pipeline aortic motion measurements:
a. Acquisition of a 4D balanced steady state free precession (bSSFP) scan with compressed sensing reconstruction into a 4D dataset. b. Automatic segmentation of fifteen cardiac phases using a trained nnU-net model. c. Iterative closest point (ICP) registration of a diastolic reference phase to the other 14 phases and calculation of motion versus this reference frame. d. Manual selection of region of interest (ROI) in the ascending aorta (AAo) and motion quantification of systolic and diastolic frames.