0286
Cardiovascular MRI study of the relationship between right ventricular function and biventricular shape in repaired tetralogy of Fallot1Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX, United States, 2German Competence Network for Congenital Heart Defects, Berlin, Germany, 3Department for Paediatric Cardiology and Paediatric Intensive Care Medicine, Hannover Medical School, Hannover, Germany, 4Department of Cardiothoracic, Transplantation and Vascular Surgery, Hannover Medical School, Hannover, Germany, 5Department of Paediatric Cardiology and Congenital Heart Defects, German Heart Centre Munich, Munich, Germany, 6Inria, Palaiseau, France, 7Ecole Polytechnique, CNRS, Palaiseau, France, 8School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom
Synopsis
Keywords: Myocardium, Cardiovascular, Statistical shape modeling, biomechanical modeling, myocardial contractility, biventricular interaction, biomarkers
Motivation: In patients with repaired tetralogy of Fallot prolonged exposure to the right ventricular (RV) pressure and/or volume overload can affect the function of both RV and left ventricle (LV).
Goal(s): We aimed to investigate the link between RV function and RV and LV shape variation.
Approach: We combined biomechanical modeling (i.e., provides RV contractility) with statistical shape modeling to quantify function and shape interaction.
Results: Higher values of RV contractility were associated with a compressed LV cavity with associated septal flattening. No meaningful relationship was identified between RV function and RV endocardial shape.
Impact: The link between anatomy and function can be studied with unprecedented detail in rTOF by combining biomechanical and statistical modeling frameworks from MRI. Such an approach facilitates the discovery of new disease mechanisms.
Introduction
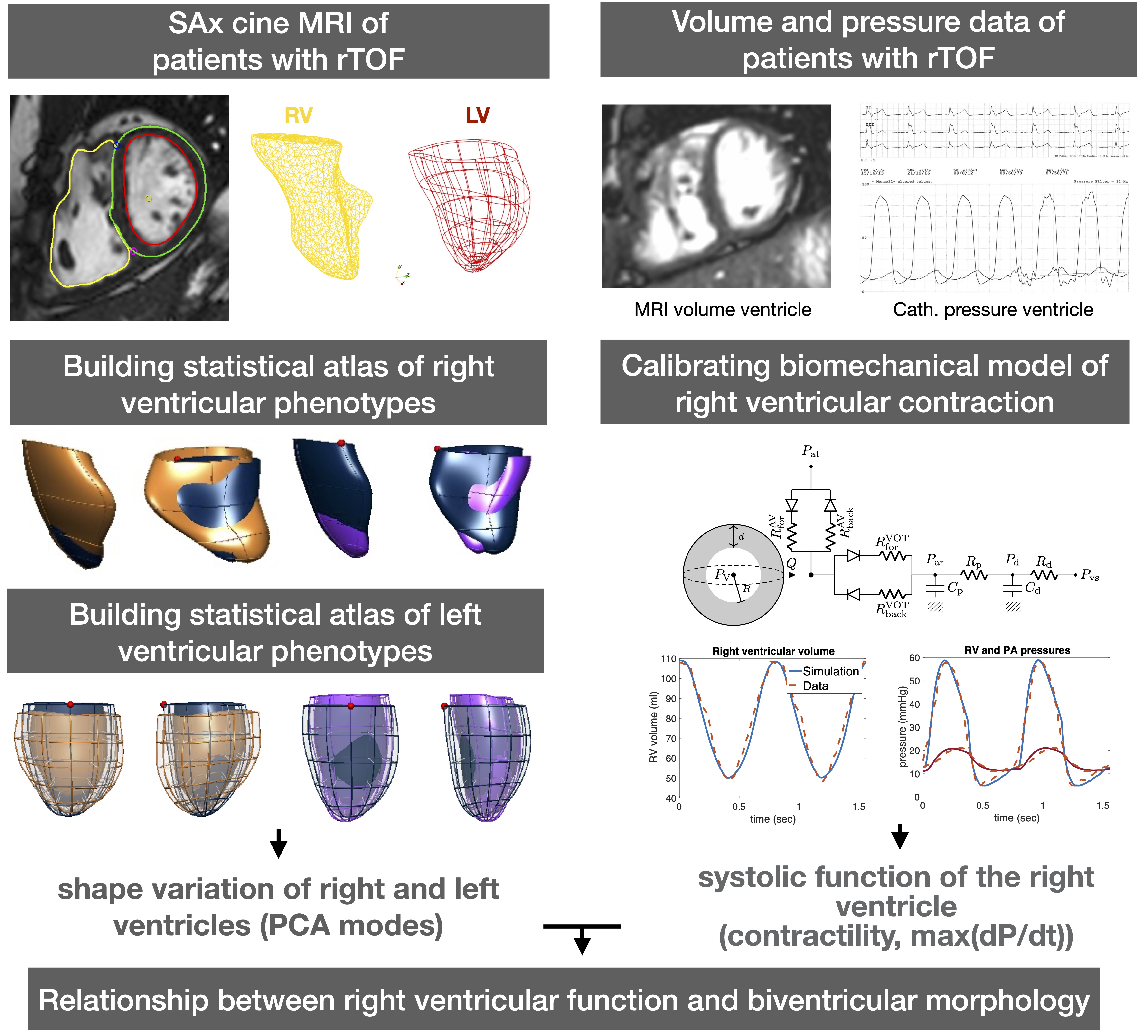
Patients with repaired tetralogy of Fallot (rTOF) experience chronic right ventricular (RV) pressure and/or volume overload leading to a compromised RV performance. In addition, the left ventricular (LV) cavity can experience deconditioning secondary to RV remodeling via direct ventricular interaction1.Exploring the link between ventricular morphology and function could provide novel insights of disease pathophysiology. In this work, we approached this link by a comprehensive analysis of cardiovascular magnetic resonance imaging (MRI) datasets and invasive hemodynamics. We combined biomechanical model of the heart to obtain contractility metrics with a statistical shape model to quantify variation in ventricular shape. We hypothesize that the level of RV inotropy is linked to specific patterns of RV or LV shape in patients with rTOF.
Methods
Shape descriptors: statistical shape models57 cardiovascular MRI datasets (retrospectively ECG-gated cine bSSFP sequence, SENSE=2, spatial resolution 2x2x10 mm) of patients with rTOF prior to pulmonary valve replacement (PVR) were used to construct a statistical shape atlases of RV and LV2,3. The RV endocardium and LV myocardium templates were fitted into the RV endocardial, and LV epicardial and endocardial contours in end-diastole, respectively, using a non-rigid registration method4. Principal component analysis (PCA) was used to build the model and compute shape scores (PCA scores) of RV endocardium and LV models.
Inotropic descriptors: biomechanical models
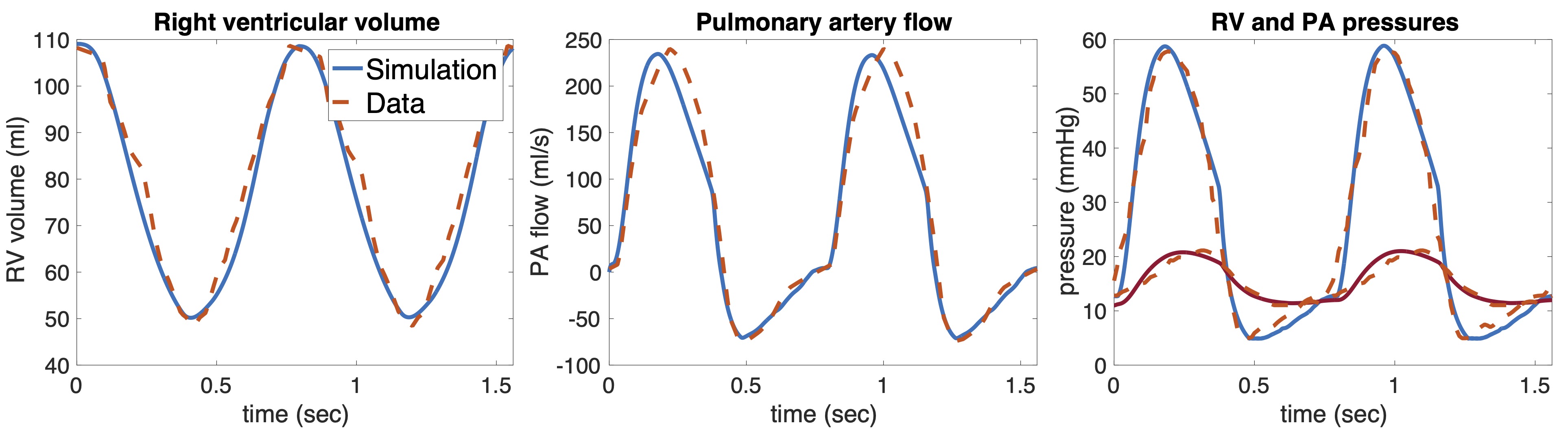
In 19 patients RV cardiovascular MRI was used along with catheterization data to construct patient-specific biomechanical models of the RV. Catheterization was performed during percutaneous PVR therapy. The biomechanical model represented the mechanical (contractile and viscoelastic) behavior of a RV cavity5,6. Cavity mass and radius were prescribed from patient’s MRI data. Mechanical laws were calibrated such that simulated pressure and volume (P-V) waveforms corresponded to the measured maximum and minimum P-V traces providing a patient-specific model of one cardiac beat (Fig. 2). Calibration of the model provided quantitative metrics of ventricular inotropic state – i.e. myocardial contractility and the maximum time derivative of RV pressure (max(dP/dt) – as in our previous clinical work7. Contractility was indexed by the ratio of ventricular chamber thickness/radius (i.e. the ratio derived from patients MRI data).
Link between anatomy and inotropy: Linear regression analysis
Linear regression analysis was used to identify the PCA components (from either the RV or the LV) that explained RV function. The adjusted R2 is used to quantify the amount of variance in RV function explained by PCA linear combination.
Results
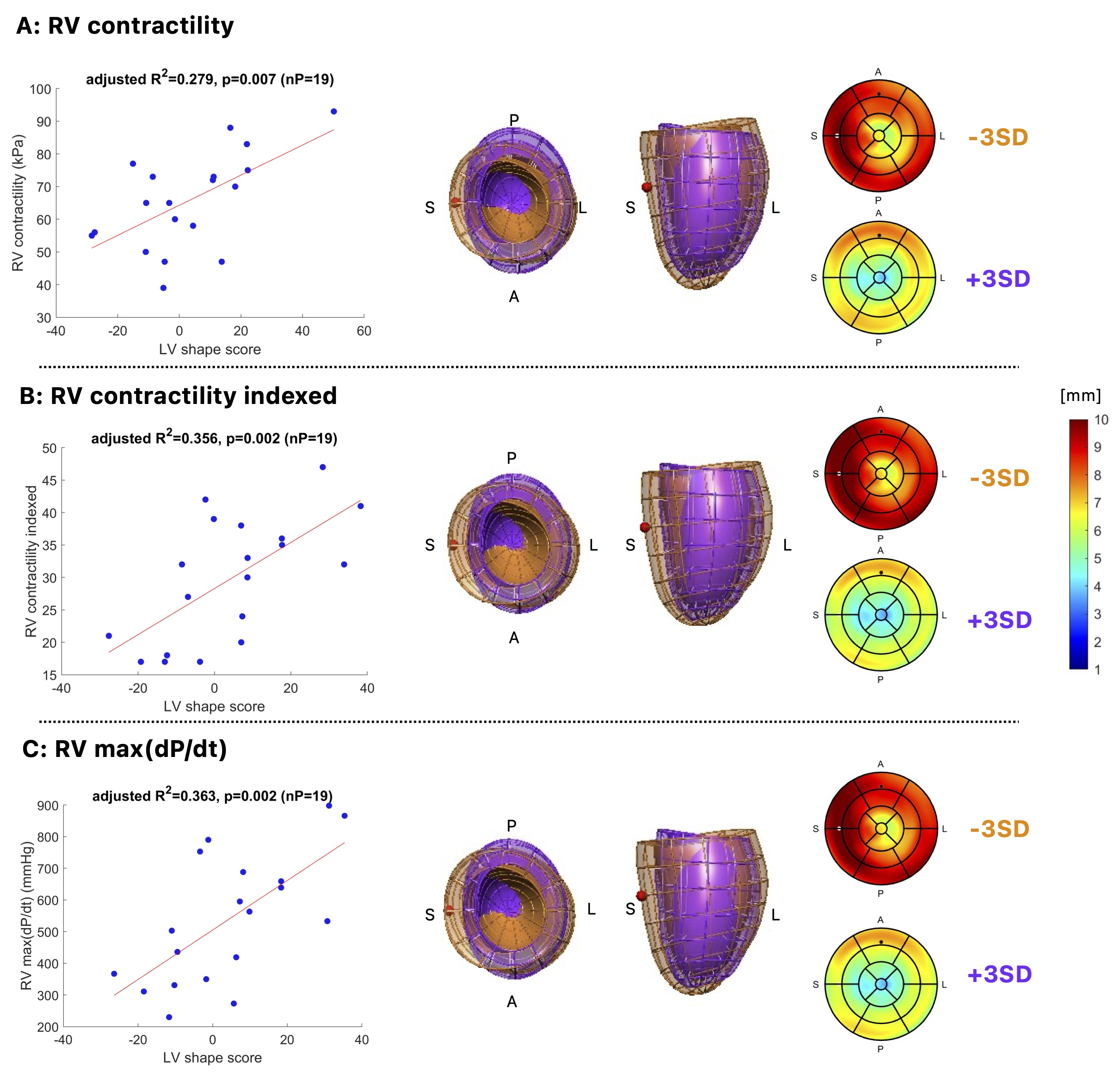
Average (±SD) EDVi was 127 (±31) ml/m2 for all patients. Pulmonary artery to RV pressure gradient was 27 (±15) mmHg for 19 patients.3rd and 6th PCA modes from the LV shape provided significant relationships with RV inotropy. Using these modes, RV contractility, contractility indexed, and max(dP/dt), was explained in 28%, 36%, and 36%, respectively (p<0.05), Fig 3.
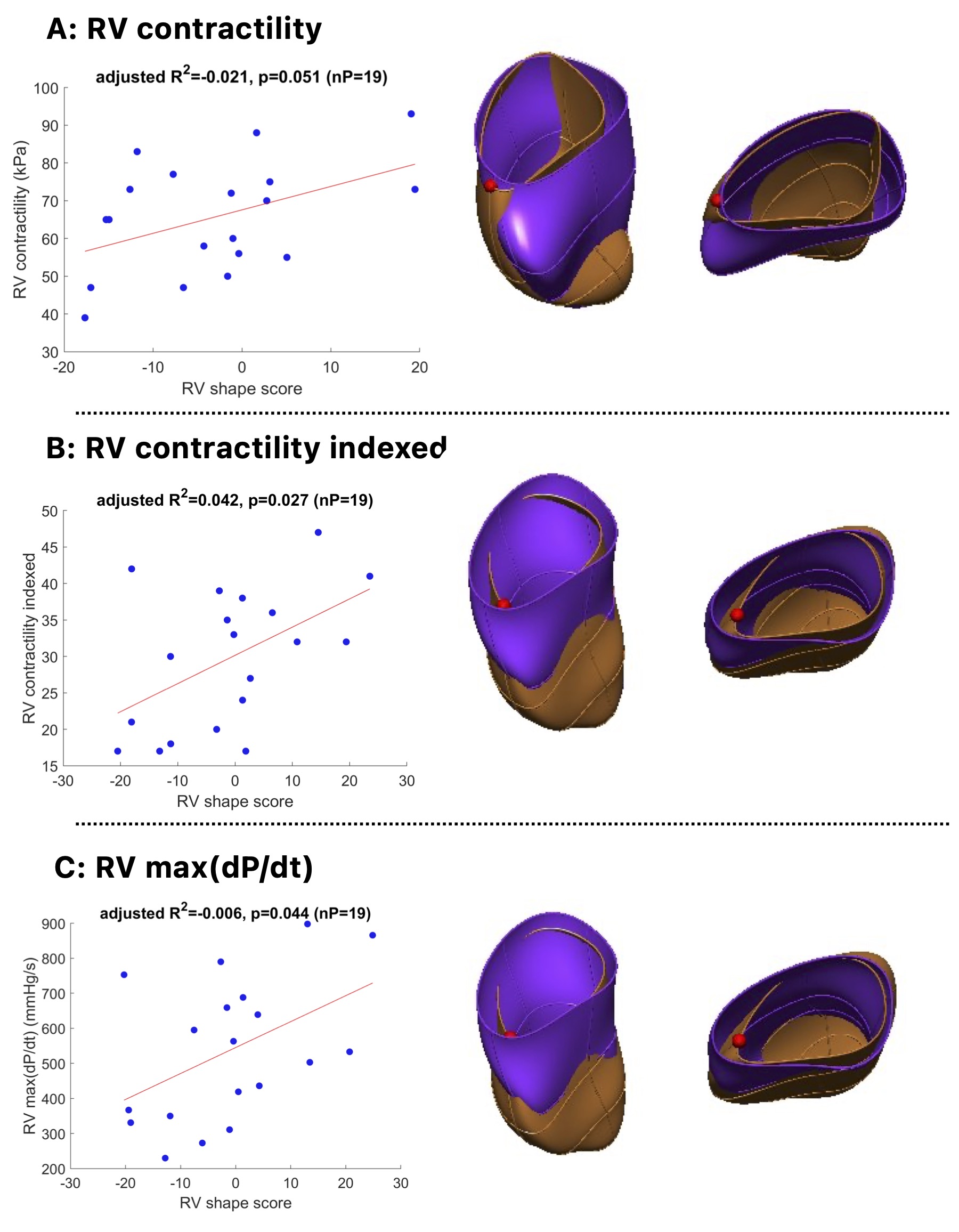
The relationship between RV shape linked to RV inotropy was identified by a combination of 4 PCA modes (5th, 6th, 7th, 8th) as linear, but not meaningful: adjusted R2 were -0.021, 0.042, -0.006 for RV contractility, contractility indexed, and max(dP/dt), respectively (p<0.05), Fig 4.
Discussion
In LV, higher values of all RV inotropy metrics produced a reduction of short axis eccentricity, a reduction of LV cavity size, and a thinning of a myocardial wall. RVs working at high wall stresses are thus linked with flattened septal wall at end-diastole. Patients with rTOF are known to experience high contractile RV demand, and this demand is interpreted to cause a compression of the LV, both in mass and volume, and with a shift towards the lateral wall.In RV, no meaningful relationship is identified between RV inotropy and RV shape. A small patient cohort with inotropy metrics might hamper to explain the features of highly irregular RV anatomy.
We present a computational framework to quantify and interpret the link between anatomy and function. The same PCA modes explained all RV inotropy metrics in the LV shape model, suggesting the robustness of the findings. RV inotropic level appeared to be more predictive of LV shape than RV shape. LV cavity shape might be an overlooked biomarker of myocardial health in rTOFs.
This study predominantly captured the effect of RV volume overload on end-diastolic shape deformation. In the future, the influence of RV pressure overload shall be investigated on end-systolic shape deformation. Nevertheless, results should be regarded as preliminary, and further studies are needed to refine the findings and interpretations.
Conclusion
In rTOF, the larger RV inotropy is associated with a smaller LV and a flattened septal wall. The link between anatomy and function can be quantified and interpreted by combining biomechanical and statistical modeling.Acknowledgements
The authors would like to acknowledge Dr Philippe Moireau, Inria research team MΞDISIM, for the development of the cardiac simulation software CardiacLab used in this work.References
1. Fernandes, F. P., Manlhiot, C., Roche, S. L., Grosse-Wortmann, L., Slorach, C., McCrindle, B. W., et al. (2012). Impaired left ventricular myocardial mechanics and their relation to pulmonary regurgitation, right ventricular enlargement and exercise capacity in asymptomatic children after repair of tetralogy of Fallot. Journal of the American Society of Echocardiography, 25(5), 494-503.
2. Rodero, C., Strocchi, M., Marciniak, M., Longobardi, S., Whitaker, J., O’Neill, M. D., et al. (2021). Linking statistical shape models and simulated function in the healthy adult human heart. PLoS Computational Biology, 17(4), e1008851.
3. Mîra, A., Lamata, P., Pushparajah, K., Abraham, G., Mauger, C. A., McCulloch, A. D., ... & Hussain, T. (2022). Le Cœur en Sabot: shape associations with adverse events in repaired tetralogy of Fallot. Journal of Cardiovascular Magnetic Resonance, 24(1), 46.
4. Mauger, C., Gilbert, K., Lee, A. M., Sanghvi, M. M., Aung, N., Fung, K., et al. (2019). Right ventricular shape and function: cardiovascular magnetic resonance reference morphology and biventricular risk factor morphometrics in UK Biobank. Journal of Cardiovascular Magnetic Resonance, 21, 1-13.
5. Caruel, M., Chabiniok, R., Moireau, P., Lecarpentier, Y., & Chapelle, D. (2014). Dimensional reductions of a cardiac model for effective validation and calibration. Biomechanics and modeling in mechanobiology, 13, 897-914.
6. Chapelle, D., Le Tallec, P., Moireau, P., & Sorine, M. (2012). Energy-preserving muscle tissue model: formulation and compatible discretizations. International Journal for Multiscale Computational Engineering, 10(2).
7. Gusseva, M., Hussain, T., Friesen, C. H., Moireau, P., Tandon, A., Patte, C., et al. (2021). Biomechanical modeling to inform pulmonary valve replacement in tetralogy of Fallot patients after complete repair. Canadian Journal of Cardiology, 37(11), 1798-1807.
Figures