0285
Free-running 5D whole-heart MRI using a Gadolinium enhanced Fast-Interrupted Steady-State sequence to evaluate congenital heart disease1Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Service of Cardiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 3Division of Pediatric Cardiology, Mother-Woman-Child Department, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 4Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 5Center for Bio-medical Imaging (CIBM), Lausanne, Switzerland, 6Cardiac MR Center, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 7Diagnostic, Interventional and Pediatric Radiology (DIPR), Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland, 8Translational Imaging Center (TIC), Swiss Institute for Translational and Entrepreneurial Medicine, Bern, Switzerland
Synopsis
Keywords: Myocardium, Cardiovascular, Congenital heart disease, Free-running, whole-heart
Motivation: There is a need for simplified and time-efficient dynamic whole-heart imaging in the evaluation of congenital heart disease patients.
Goal(s): To demonstrate the feasibility of Gadolinium enhanced 5D FISS CMR and compare it to established 2D and 3D CMR methods in a cohort of congenital heart disease patients.
Approach: Ejection fraction and vessel sharpness measurements derived from established 2D and 3D CMR are quantitatively compared to those obtained from the proposed 5D sequence.
Results: 5D FISS CMR is feasible for the evaluation of cardiac function and anatomy building towards an easy-to-use and time-efficient method for evaluating congenital heart disease.
Impact: Free-running 5D whole-heart MRI using a Gadolinium enhanced FISS sequence enables both measurements of cardiac function and evaluation of morphology in patients with congenital heart disease with a fixed six-minute scan time.
Background
In a typical clinical cardiac MRI exam, 2D CINE imaging, and electrocardiogram (ECG) triggered respiratory navigated 3D whole heart imaging are essential for assessing the ventricular function and cardiac morphology [1,2]. Recently, free-running 5D whole-heart imaging has been proposed to simplify exams by capturing the entire dynamic 3D cardiac anatomy without the need for ECG gating or breath-holding [3]. In CHD patients, free-running 5D imaging has been shown to provide excellent delineation of the cardiac anatomy [4] and assessment of cardiac function [5] within a single time-efficient sequence using ferumoxytol. In this work, we extend the use of 5D imaging, and evaluate its initial feasibility for Gadolinium enhanced (Gd) imaging of patients with CHD. Using a Fast-Interrupted Steady-State (FISS) sequence [6,7] we compare the proposed Gd 5D FISS sequence to gold standard 2D CINE imaging and to a well-established ECG-triggered self-navigated 3D whole heart sequence [8] in a cohort of CHD patients.Methods
Ten patients (47±16 years of age, 7 female) were included, with approval by the local research ethics committee. All patients underwent 2D CINE imaging prior to a clinically indicated injection of 0.2 mmol/kg body weight of Gadobutrol (Gadovist™, Bayer Schweiz AG, Switzerland). Self-navigated ECG-triggered 3D radial whole-heart imaging and a free-running 5D FISS research sequence (7) were performed after contrast injection. For simplicity we refer to these sequences as 2D, 3D, and 5D hereafter. Scans were performed on a 1.5T clinical MR scanner (MAGNETOM Sola, Siemens Healthineers AG, Erlangen, Germany) with an 18-channel coil, acquired spatial resolution (2D: 1.17-1.40 x 1.17-1.40 x 8 mm3, 3D: 1.15-1.25 mm3, 5D: 1.25 mm3, field-of-view (2D: 300-360 mm2, 3D: 220-240 mm3, 5D: 220 mm3), and number of cardiac phases (2D: 25, 5D: 25). The acquisition time for each sequence was recorded for subsequent comparison.Segmentation and calculation of left ventricular ejection fraction for both the acquired 2D images and 5D reformats was performed using open-source software (Medviso Segment [9]). A contrast ratio was calculated from 2D, 3D, and 5D images by manually selecting ROIs in the left ventricular blood pool and myocardium. Sharpness for each sequence was measured as the slope of sigmoid functions fitted to lines perpendicular to the blood-myocardium interface as defined by the manually selected ROIs [10]. Multi-planar reformats of the coronary arteries from the acquired 3D and manually selected rest-phase of the 5D images were performed in Soap-bubble for qualitative comparison [11]. Comparison of 2D versus 5D ejection fraction was measured by the Pearson correlation coefficient and Bland-Altman analysis. Contrast and sharpness between 2D, 3D and 5D images was compared with a paired t-test with p<0.05 considered statistically significant after Bonferroni correction for multiple comparisons.
Results
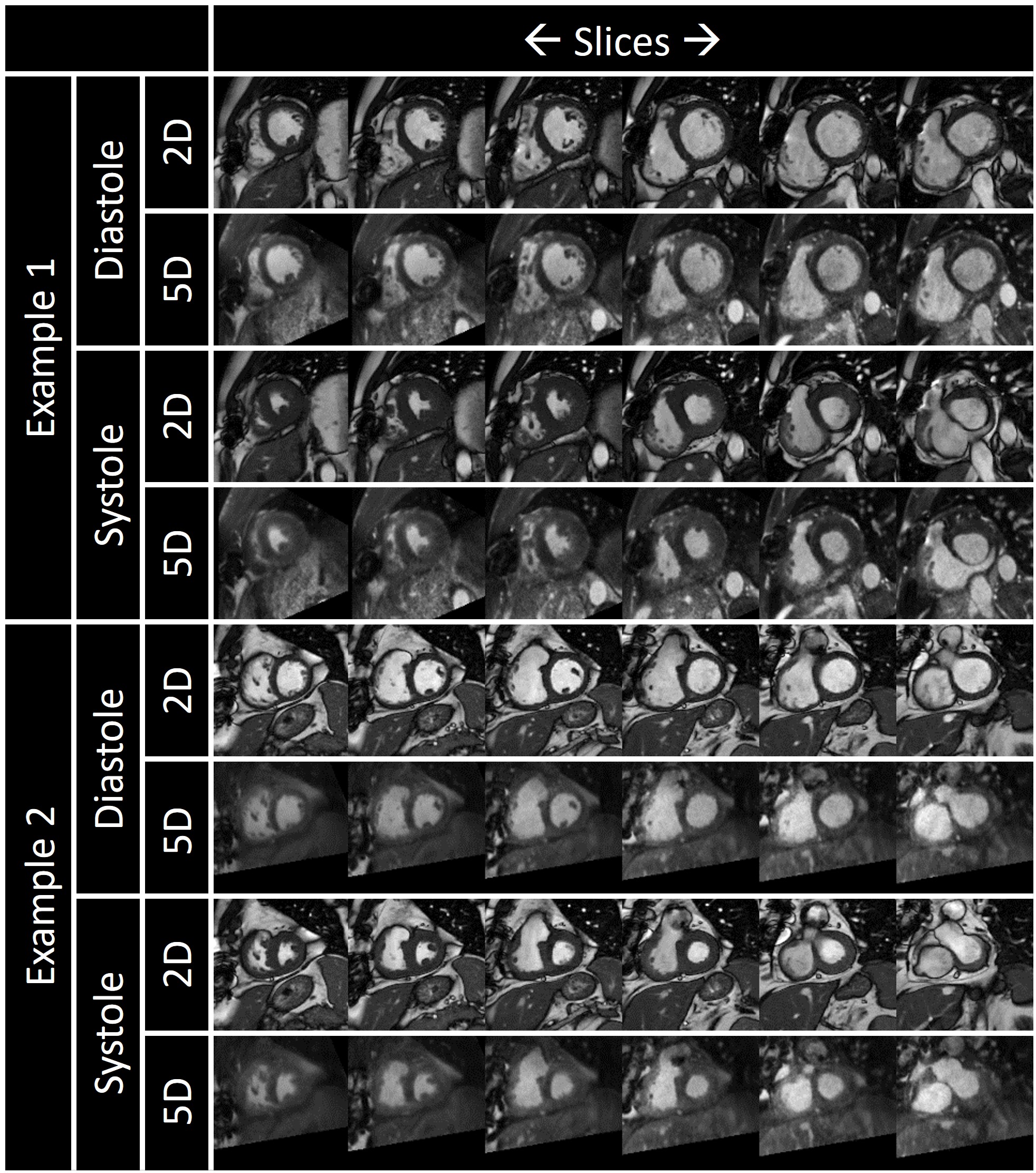
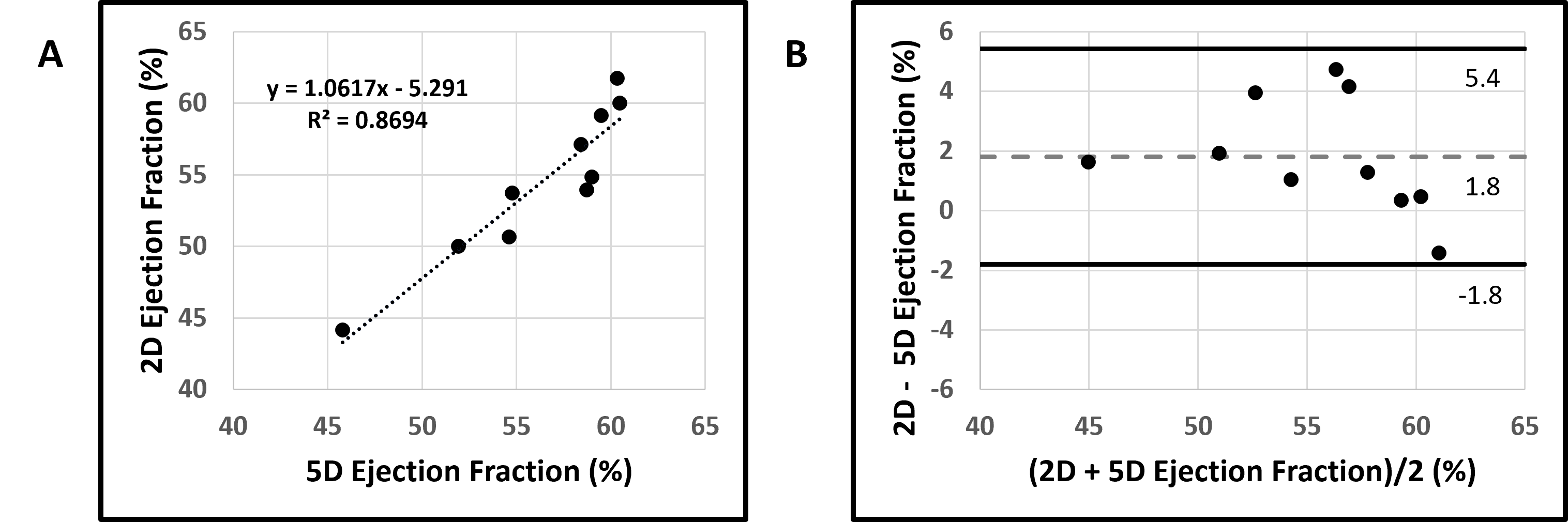
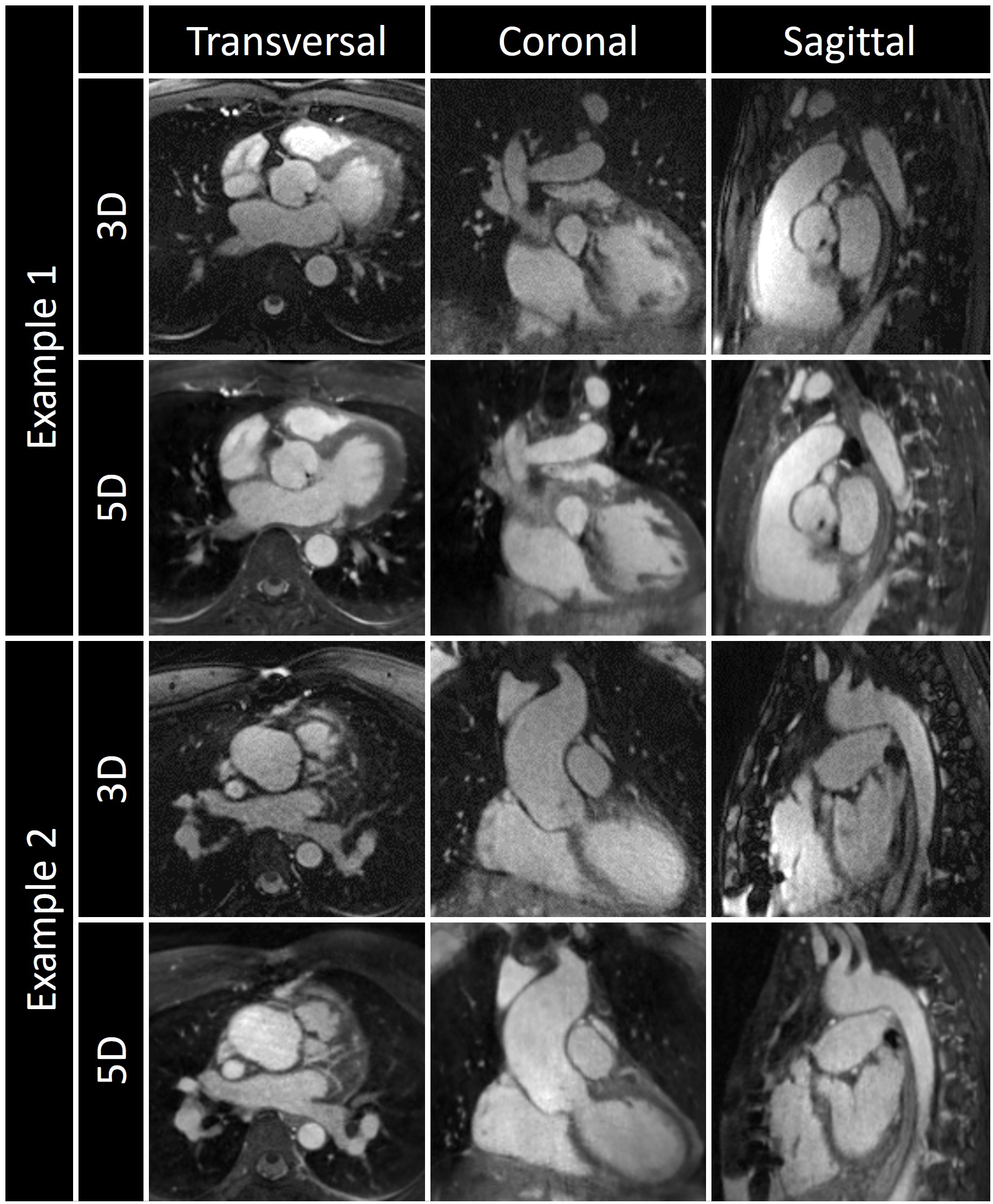
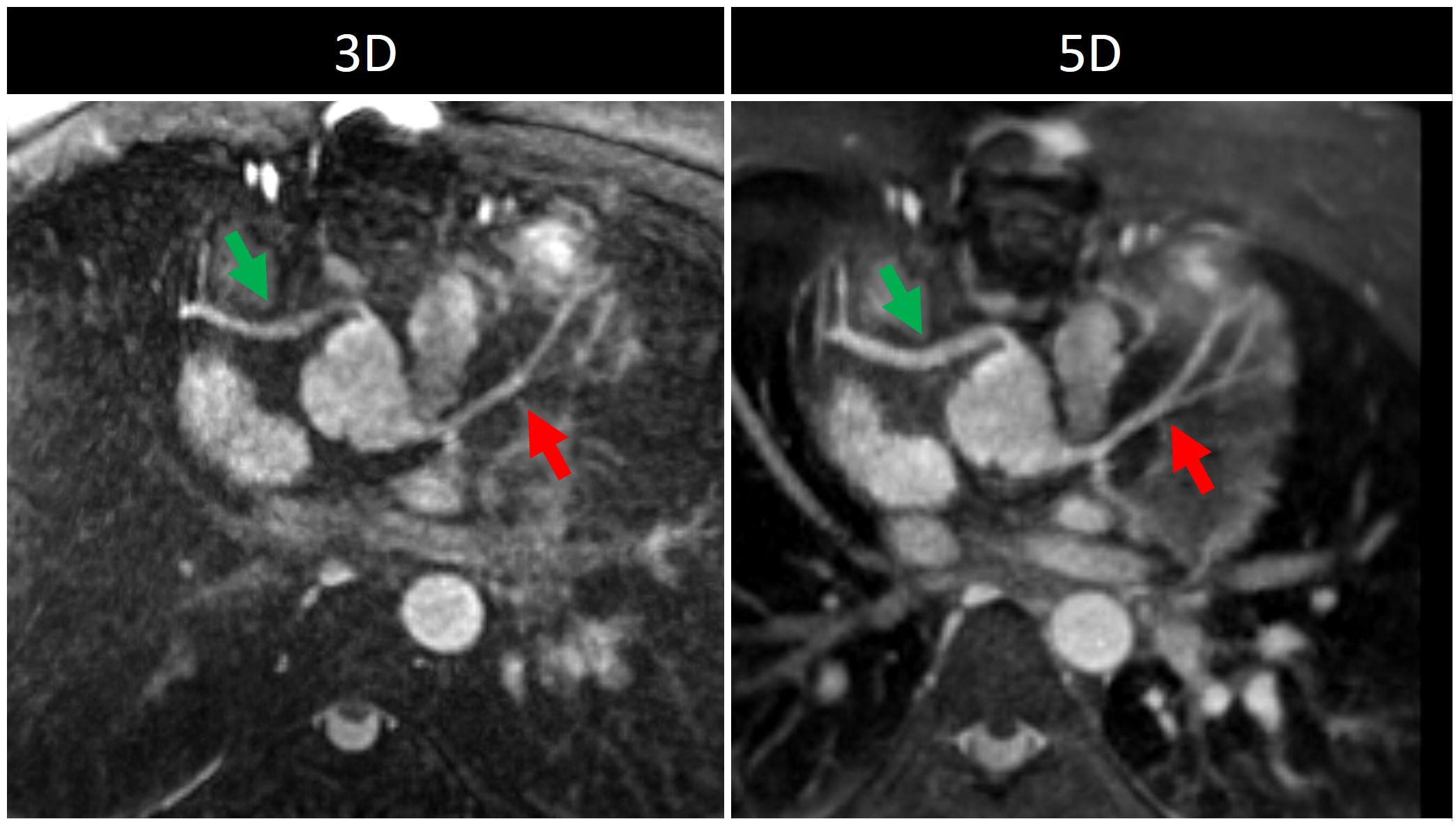
Free-running 5D had a fixed scan time of 6 minutes compared to 2D (3-8 minutes) and 3D (6-10 minutes). 5D images were similar to reference 2D with clear delineation of the cardiac chambers in short-axis views throughout the cardiac cycle (Fig. 1). This enabled evaluation of left ventricular function (Fig. 2) with very strong correlation (R = 0.87) between measurements derived from 2D and 5D images. Similarly, 5D images compare favorably to the reference 3D images providing a comprehensive assessment of cardiac morphology (Fig. 3). Overall, 2D images, provided significantly higher blood-myocardium contrast (mean ± standard deviation across all patients: 3.75±0.66) when compared to 3D (1.78±0.15, p<10-6) and 5D (1.91±0.13, p<10-5) images. However, there was no significant difference between the contrast of 3D and 5D images (p = 0.1). Similarly, the blood-myocardium interface sharpness was higher for 2D images (0.58±0.09) when compared to 3D (0.48±0.10, p = 0.002) and 5D images (0.48±0.13 p<10-2), but there was no significant difference between 3D and 5D (p = 0.19). Both 3D and 5D images could be reformatted to visualize the origins of coronary arteries with good vessel conspicuity (Fig. 4) and dynamic motion of the right coronary artery could be visualized using 5D (Fig. 5).Discussion and Conclusion
Gd enhanced free-running 5D FISS whole-heart images were acquired in a cohort of CHD patients and both qualitatively and quantitatively compared with reference standard 2D and 3D. While 3D and 5D sequences cannot match the contrast and sharpness of 2D imaging, 5D imaging provided measurements of left ventricular ejection fraction while simultaneously enabling assessment of cardiac morphology in arbitrary scan planes. 5D imaging underestimated left ventricular ejection fraction up to 5%. These initial results are therefore promising for anatomical assessment of the heart and motivate future evaluation of this sequence to further improve the functional assessment of the left ventricular function by 5D imaging.Acknowledgements
Christopher Roy is the PI on Swiss National Science Foundation Grant PZ00P3_202140 that funded part of this research. Matthias Stuber is the PI on the Swiss National Science Foundation Grants 320030_173129 and 201292 that funded part of this research.References
1. Dorfman AL, Geva T, Samyn MM, Greil G, Krishnamurthy R, Messroghli D, et al. SCMR expert consensus statement for cardiovascular magnetic resonance of acquired and non-structural pediatric heart disease. J Cardiovasc Magn Reson. 2022;24:44.
2. Fratz S, Chung T, Greil GF, Samyn MM, Taylor AM, Valsangiacomo Buechel ER, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15:51.
3. Di Sopra L, Piccini D, Coppo S, Stuber M, Yerly J. An automated approach to fully self-gated free-running cardiac and respiratory motion-resolved 5D whole-heart MRI. Magn Reson Med. 2019;82:2118–32.
4. Roy CW, Di Sopra L, Whitehead KK, Piccini D, Yerly J, Heerfordt J, et al. Free-running cardiac and respiratory motion-resolved 5D whole-heart coronary cardiovascular magnetic resonance angiography in pediatric cardiac patients using ferumoxytol. J Cardiovasc Magn Reson. 2022;24:39.
5. Salim Aymeric Si-Mohamed, Ludovica Romanin, Mariana Falcao, Jerome Yerly, Estelle Tenisch, Tobias Rutz, Charles De Bourguignon, Jurg Schwitter, Matthias Stuber, Christopher Roy and MP. Free-running 5D whole-heart MRI with ferumoxytol enhancement to evaluate cardiac function in congenital heart disease. Int Soc Magn Reson Med. 2023. p. 0556.
6. Koktzoglou I, Edelman RR. Radial fast interrupted steady-state (FISS) magnetic resonance imaging. Magn Reson Med. 2018;79:2077–86.
7. Bastiaansen JAM, Piccini D, Di Sopra L, Roy CW, Heerfordt J, Edelman RR, et al. Natively fat‐suppressed 5D whole‐heart MRI with a radial free‐running fast‐interrupted steady‐state (FISS) sequence at 1.5T and 3T. Magn Reson Med. 2019;mrm.27942.
8. Piccini D, Littmann A, Nielles-Vallespin S, Zenge MO. Respiratory self-navigation for whole-heart bright-blood coronary MRI: Methods for robust isolation and automatic segmentation of the blood pool. Magn Reson Med. 2012;68:571–9.
9. Heiberg E, Sjögren J, Ugander M, Carlsson M, Engblom H, Arheden H. Design and validation of Segment--freely available software for cardiovascular image analysis. BMC Med Imaging. 2010;10:1.
10. Ahmad R, Ding Y, Simonetti OP. Edge sharpness assessment by parametric modeling: Application to magnetic resonance imaging. Concepts Magn Reson Part A. 2015;44:138–49.
11. Etienne A, Botnar RM, van Muiswinkel AMC, Boesiger P, Manning WJ, Stuber M. Soap-Bubble visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002;48:658–66.
Figures