0284
Initial demonstration of free-running whole-heart radial 4D flow using ultra-short echo times (UTE)1Department of Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Service of Cardiology, Heart and Vessel Department, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 3Division of Pediatric Cardiology, Woman-Mother-Child Department, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 4Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 5Department of Biomedical Engineering, Northwestern University, Chicago, IL, United States, 6Center for Biomedical Imaging (CIBM), Lausanne, Switzerland
Synopsis
Keywords: Flow, Heart, Whole-heart, UTE, Congenital Heart Disease
Motivation: Free-running phase-contrast whole-heart MRI, despite its ease of use and efficiency may suffer from artifacts and inaccuracy in the presence of non-laminar flow and high velocities due to prolonged echo times.
Goal(s): Our goal was to reduce the echo time in free-running radial 4D flow (radial 4D flow).
Approach: We incorporated ultra-short echo time (UTE) imaging techniques into our radial 4D flow framework.
Results: Net flow and peak flow measurements that correlate well with reference values were obtained in a cohort of healthy volunteers with the modified sequence and enabled qualitative evaluation of turbulent flow in patients with congenital heart disease.
Impact: The combination of UTE and radial 4D flow MRI marks a step towards a more precise and robust quantification of hemodynamics under complex conditions, in an effort to improve both diagnosis and patient outcomes.
INTRODUCTION
Recent advances in free-running radial whole-heart phase-contrast MRI [1,2] have enabled the comprehensive assessment of cardiovascular hemodynamics in a fixed scan time without the need for ECG-gating or respiratory navigation. The free-running properties offer simplified scan planning along with robust compensation of respiratory motion through either respiratory-resolved 5D flow [1] or respiratory-corrected 4D flow [2] reconstructions. Still, when faced with non-laminar blood flow and high velocities, as in the case of patients with high grade stenoses or malformations, signal dephasing coupled with long echo times can impact both the accuracy of blood-flow measurements and image quality [3]. Conversely, ultra-short echo-time (UTE) sequences are successful in reducing flow dephasing artifacts including applications to free-running anatomical imaging [4] and 4D flow [3]. In this work, we therefore integrate UTE [4,5] into the previously described free-running radial flow sequence [1] to reduce the echo time and build towards a robust method for free-running radial flow in the presence of non-laminar flow and high velocities. We test the hypothesis that our proposed radial UTE flow sequence provides net and peak flow measurements that are comparable to previously described radial [2] and Cartesian techniques [6] in healthy volunteers and demonstrate its initial feasibility in patients with congenital heart disease (CHD).METHODS
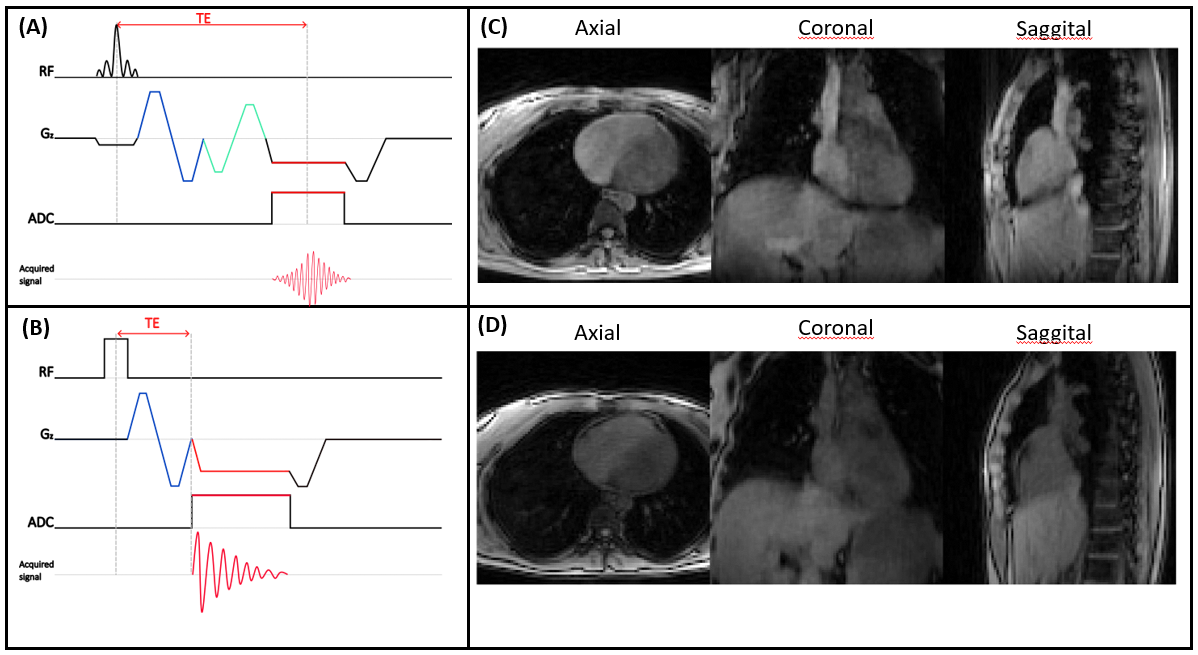
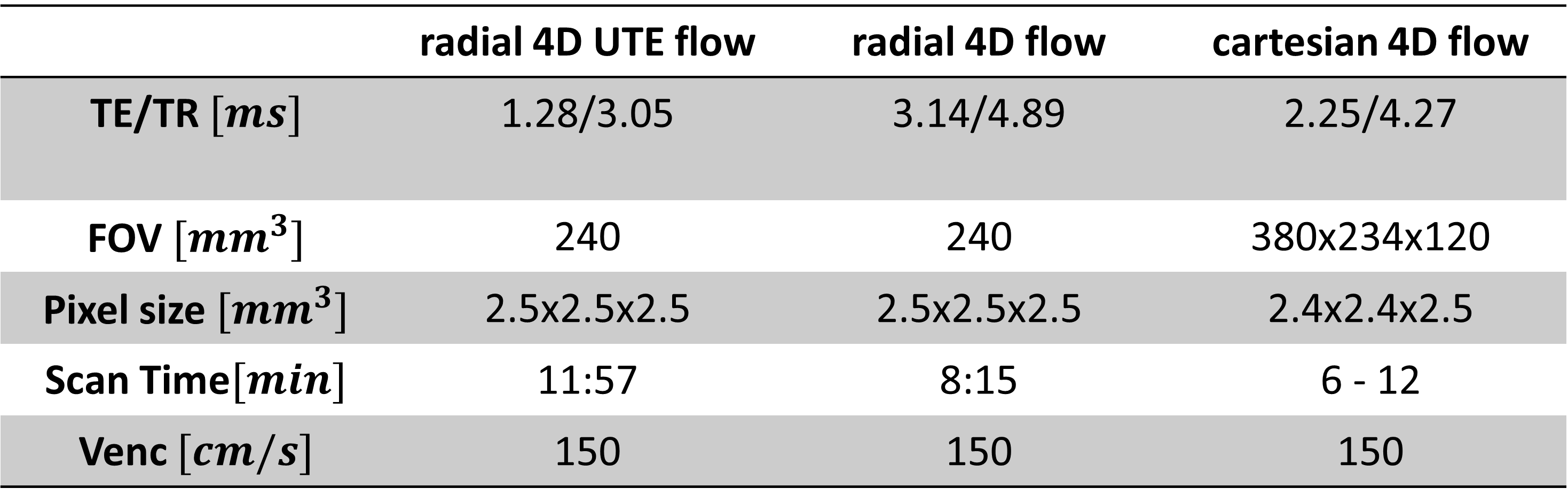
A free-running 3D radial phase-contrast MRI sequence was modified to reduce the echo-time [Figure 1]. The RF excitation was made non-selective, center-out readouts with ramp sampling were acquired, and the flow-compensation gradient, that is no longer needed due to ramp sampling, was removed. Seven healthy volunteers (ages: 25-35; 3 females, 4 males) were scanned on a 3T research scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). For each volunteer, three sequences were acquired: free-running radial flow method (radial 4D flow) [1,2], the proposed free-running radial UTE flow variant (radial 4D UTE flow), and respiratory navigator-gated Cartesian 4D flow (Cartesian 4D flow) for reference . The acquisition was performed in a random order to avoid fatigue bias. Scan parameters are provided in Table 1. A pulse oximeter signal recorded throughout the scan was used for retrospective cardiac binning. Both radial sequences were reconstructed offline into 4D flow datasets using focused navigation for respiratory motion correction and compressed sensing [2]. The Cartesian 4D flow sequence was reconstructed inline . All three sequences were analyzed using Circle CVI42(Calgary, Canada), wherein 2D planes in the ascending aorta (AAo), descending aorta (DAo), and main pulmonary artery (MPA) were manually chosen for estimation and comparison of net volume and peak flow. The agreement between the 3 sequences was assessed by Pearson correlation coefficients and Bland-Altman analysis. Finally, the initial feasibility of the proposed UTE flow sequence was assessed in three patients on 1.5 T clinical scanner (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany) with CHD and streamline analysis was performed in Circle CVI42. All volunteers and patients provided written informed consent compliant with our institutional guidelines and approved by the local research ethics committee.RESULTS
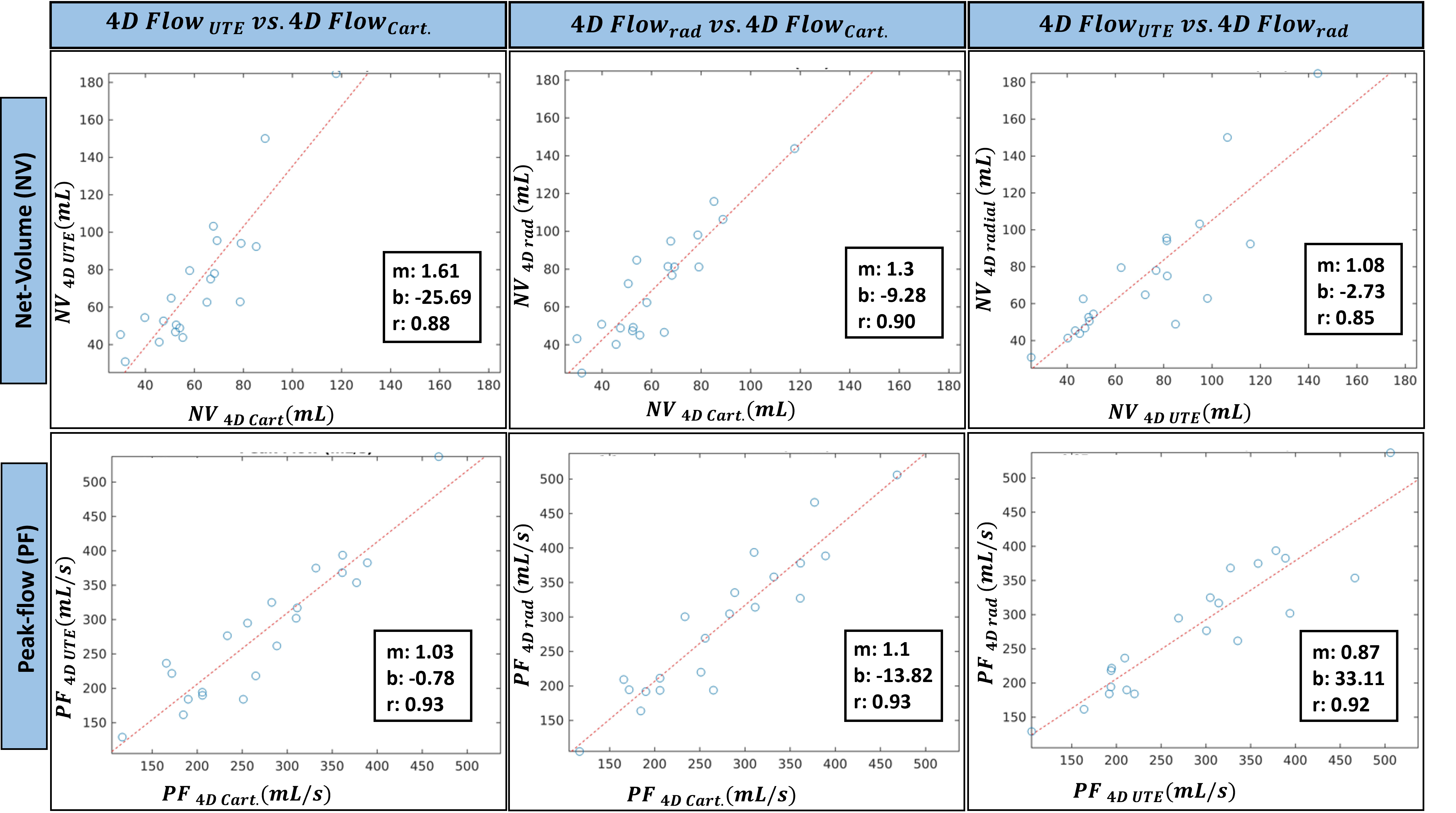
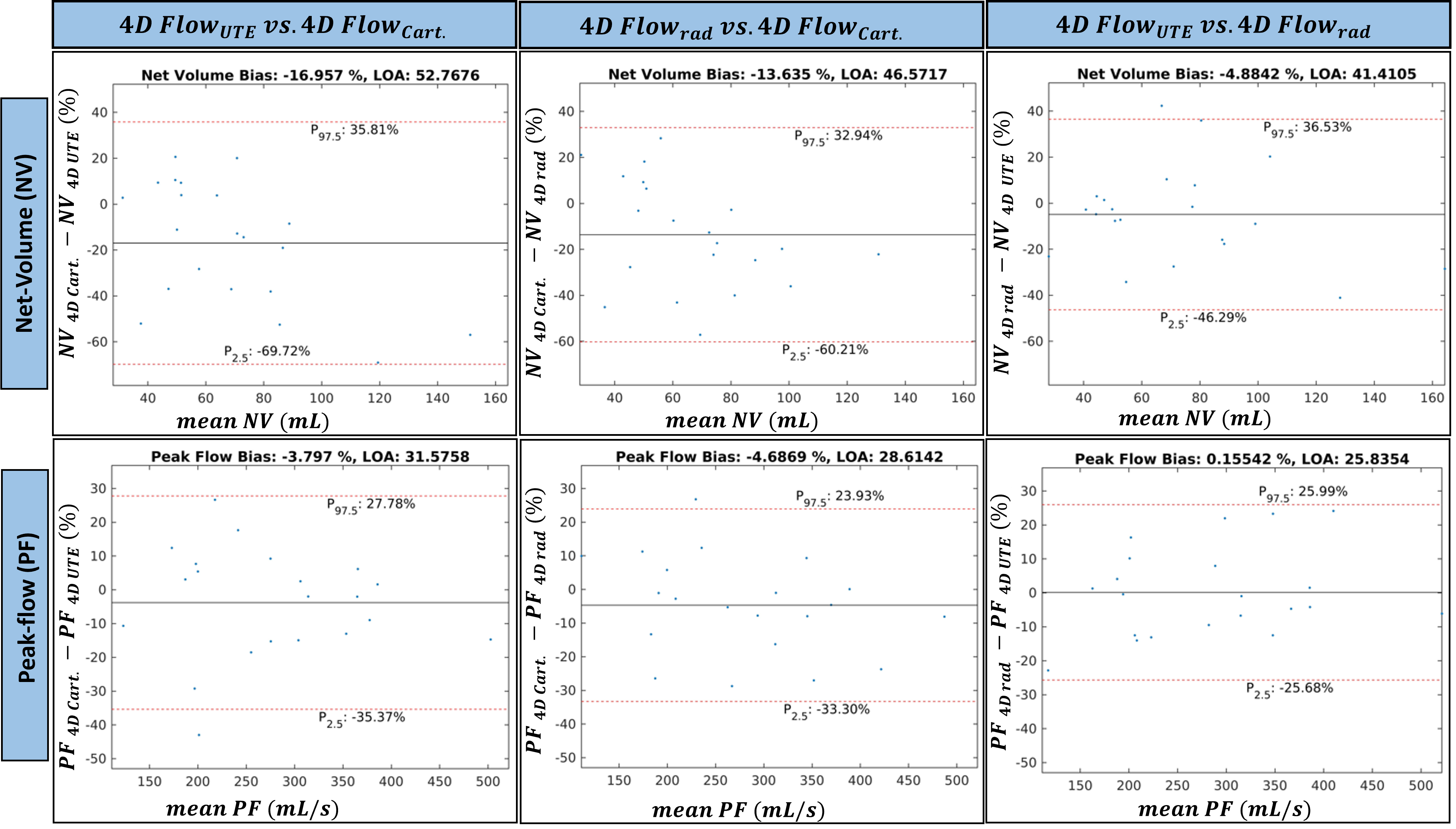
The quality of the 4D radial UTE flow magnitude images is comparable to the contrast of the 4D radial flow magnitude images [Figure 1]. Overall, there was a strong correlation between net volume and peak flow measurements when comparing the proposed radial 4D UTE flow to the previously established radial 4D flow (r2net-volume=0.85, r2peak-flow=0.94) [Figure 2]. Similarly, there were also strong correlation between net volume and peak flow measurements when comparing the reference cartesian 4D flow to radial 4D UTE flow (r2net-volume=0.88, r2peak-flow=0.93) and radial 4D flow (r2net-volume=0.90, r2peak-flow=0.93) respectively, with radial 4D flow having the strongest overall correlation [Figure 2]. Bland-Altman analysis [Figure 3], however showed larger bias in net volume but a lower bias in peak flow measurements between cartesian 4D flow and radial UTE flow (bnet-volume= -16.96, bpeak-flow= -3.98), with similar results between cartesian 4D flow and radial 4D flow (bnet-volume= -13.64, bpeak-flow= -4.69). The smallest overall bias obtained (bnet-volume= -4.88, bpeak-flow= 0.16) was between radial 4D flow and radial 4D UTE flow measurements. In the patients, streamline analysis enables visualization of flow through stenoses demonstrating the initial feasibility of our approach [Figure 4].DISCUSSION AND CONCLUSION
This work introduces free-running radial 4D UTE flow, a step towards robust quantitative whole-heart assessment of hemodynamics in the presence of non-laminar flow. These promising initial results in healthy volunteers motivate more thorough testing in a flow phantom and a larger cohort of volunteers and patients in working towards the goal of providing time-efficient whole-heart 4D flow with simplified scan planning to improve patient management in diseases that affect the cardiovascular system.Acknowledgements
Matthias Stuber is the PI on the Swiss National Science Foundation Grants 320030_173129 and 201292 that funded part of this research. Christopher Roy is the PI on Swiss National Science Foundation Grant PZ00P3_202140 that funded part of this research.References
1. Ma LE, Yerly J, Piccini D, Di Sopra L, Roy CW, Carr JC, Rigsby CK, Kim D, Stuber M, Markl M. 5D Flow MRI: A Fully Self-gated, Free-running Framework for Cardiac and Respiratory Motion-resolved 3D Hemodynamics. Radiol Cardiothorac Imaging. 2020 Nov 12;2(6):e200219. Doi: 10.1148/ryct.2020200219.
2. Mariana B. L. Falcão, Giulia M. C. Rossi, Tobias Rutz, Milan Prša, Estelle Tenisch, Liliana Ma, Elizabeth K. Weiss, Justin J. Baraboo, Jérôme Yerly, Michael Markl, Matthias Stuber, Christopher W. Roy. Focused navigation for respiratory–motion-corrected free-running radial 4D flow MRI
3. Kadbi M, Negahdar M, Cha JW, Traughber M, Martin P, Stoddard MF, Amini AA. 4D UTE flow: a phase-contrast MRI technique for assessment and visualization of stenotic flows. Magn Reson Med. 2015 Mar;73(3):939-50. Doi: 10.1002/mrm.25188. Epub 2014 Mar 6. PMID: 24604617.
4. Giulia M.C. Rossi, Ludovica Romanin, Mariana B.L. Falcão, Bastien Milani, Davide Piccini, Jérôme Yerly, Jürg Schwitter, Milan Prša, Tobias Rutz, Estelle Tenisch, Matthias Stuber and Christopher W. Roy (2022). Free-running contrast-enhanced ultra-short TE (UTE) for cardiac and respiratory motion-resolved flow artifact-free 5D whole-heart MRI.
5. Delacoste J, Chaptinel J, Beigelman-Aubry C, Piccini D, Sauty A, Stuber M. A double echo ultra short echo time (UTE) acquisition for respiratory motion-suppressed high resolution imaging of the lung. Magn Reson Med. 2018 Apr;79(4):2297-2305. Doi: 10.1002/mrm.26891. Epub 2017 Aug 30. PMID: 28856720.
6. Di Sopra, L., Piccini, D., Coppo, S., Stuber, M., & Yerly, J. (2019). An automated approach to fully self‐gated free‐running cardiac and respiratory motion‐resolved 5D whole‐heart MRI. Magnetic resonance in medicine, 82(6), 2118-2132.
Figures