0282
Ex-vivo 4D Flow MRI for Evaluation of Aortic Valve Pathologies in a Mock Circulatory System1Surgery, University of Wisconsin-Madison, Madison, WI, United States, 2Mechanical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 3Radiology, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Keywords: Valves, Velocity & Flow
Motivation: The Ross Procedure is a complex cardiac surgery that utilizes the pulmonary valve to replace a diseased aortic valve. More work is needed to improve preoperative candidacy.
Goal(s): To develop and validate an ex-vivo model of the aortic valve in combination with a mock circulatory system.
Approach: The left ventricle was mounted on a circulatory loop with preservation of aortic valve anatomy and application of hemodynamic flow to assess valve characteristics.
Results: A successful system was built and 4D Flow MRI performed with resultant functional quantification and representative curves mimicking ventricular inflow and aortic outflow.
Impact: 4D Flow MRI, in combination with an ex-vivo left ventricular mock circulatory system, provides a method to study aortic flow and assess valvular abnormalities or preoperative candidacy in cardiac surgery.
Introduction
The Ross procedure, wherein the diseased aortic valve is replaced with a pulmonary autograft, is rare in its complexity, however beneficial to the patient. Patients who undergo the Ross have improved age-specific survival rates, superior hemodynamics, reduced incidence of endocarditis and no need for anticoagulation.1-3 This superiority is compounded by the elevated risk of operative mortality and the inherent risk of operating on two valves.4,5 Unfortunately, up to 15% of Ross patients require reintervention, which is integrally difficult due to the complexity of the initial operation.5,6 In order to maximize the benefit to those suffering with aortic valve disease, it is important to test the effects of autograft or homograft implantation, for improvement on valve design and surgical optimization. In this study, we use 4D Flow MRI to better understand the hemodynamic changes experienced by the aortic valve in an ex-vivo model and mock circulatory loop. We ultimately aim to apply the same left-sided ex-vivo experimental set up to the right heart to fully emulate an ex-vivo Ross procedure.Methods
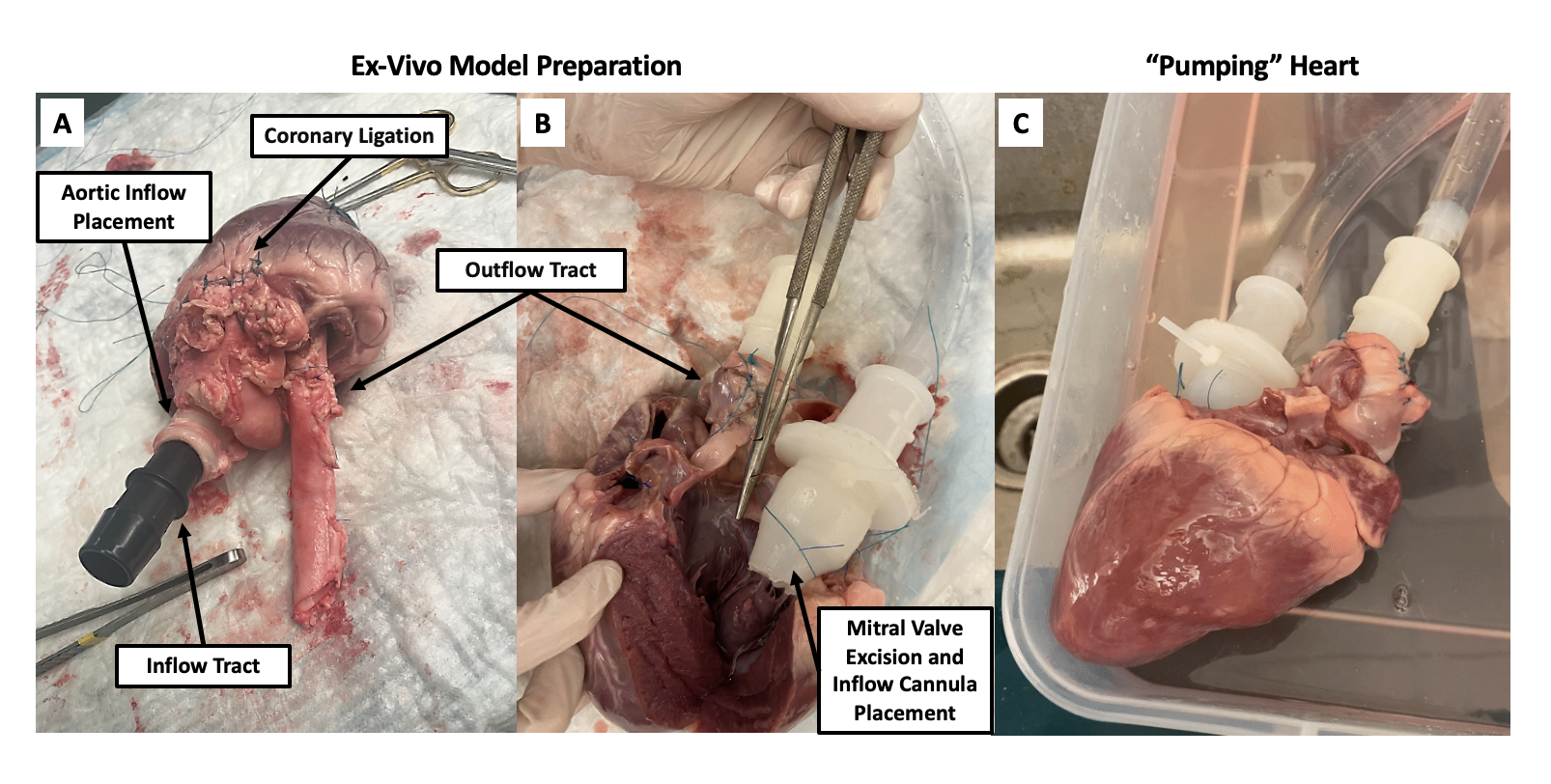
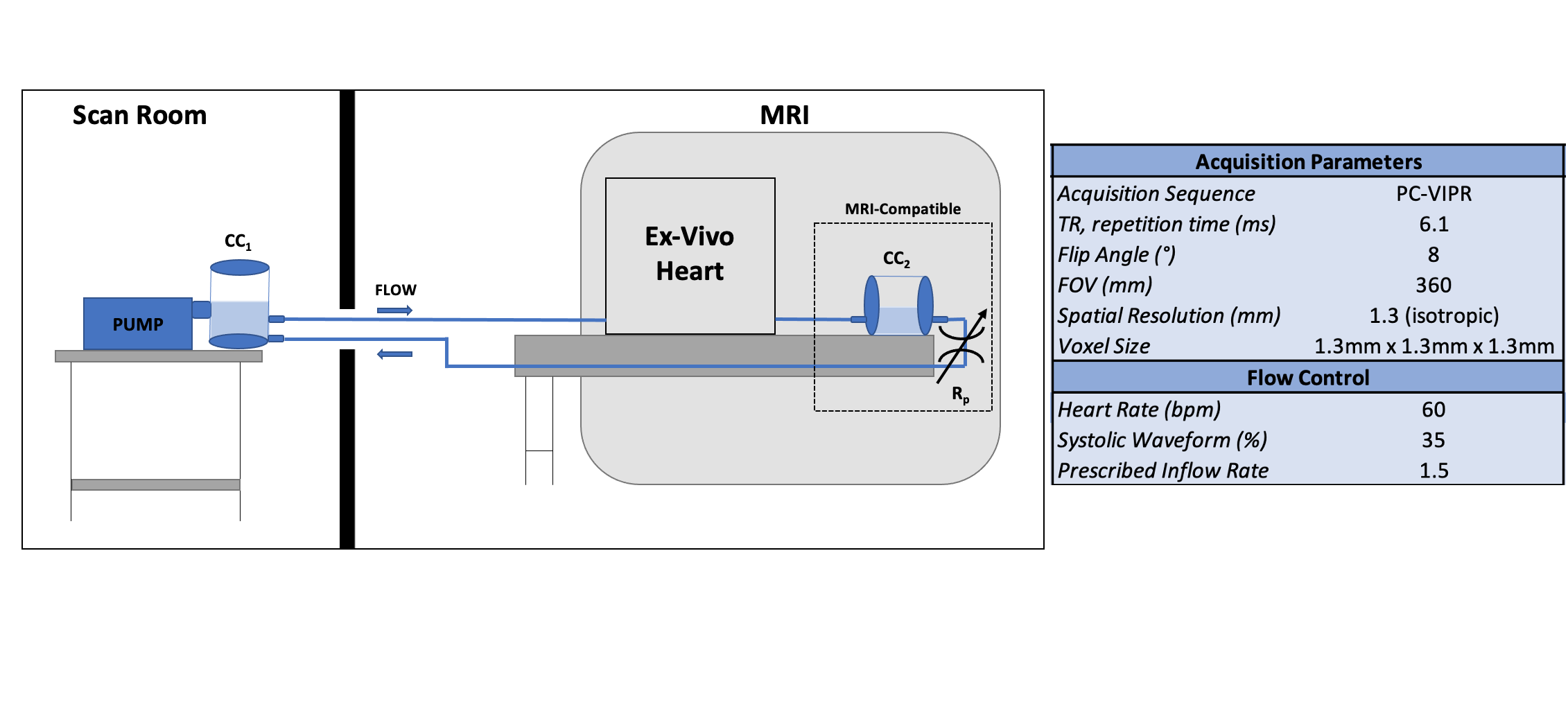
Ex-vivo Valve Preparation: All research was performed in compliance with institutional guidelines for the care of animals. Porcine cardiac specimens with a 10-15cm length of aorta were obtained from the Department of Animal and Dairy Sciences. A 5cm section of aorta was removed from the distal specimen for use as inflow. The mitral valve leaflets were partially excised and a running prolene suture via the parachute technique was used to sew the inflow to the mitral annulus. All coronaries and aortic branches were ligated. A 3D printed fixture was used to cannulate the inflow and secured with zip ties. The aortic cannula was advanced to the distal extent of the aortic valve, used to visualize the valve and then secured in place with zip ties (Figure 1).Mock Circulatory System: Physiological flow was generated using a positive displacement pulsatile pump (PD-1100, BDC Laboratories, CO). A closed flow loop was created by attaching ¾" ID flexible tubing to the inflow and outflow cannulae attached to the heart. Inflow rate, waveform (35% systolic) and heart rate (60 bpm) were controlled by the pump. In series with the pump, 3D-printed, MRI-compatible flow conditioning components including resistance valves and compliance chambers were connected. These adjustable elements were used to augment the inflow waveform to facilitate typical aortic valve dynamics by simulating arterial resistance and peripheral compliance, thus achieving physiologic flow. The working fluid used was normal saline (𝜌 = 1004 kg/m3, m = 1.01 cP, 20°C), which was circulated in our model at an inflow rate of 1.5LPM.
MRI Acquisition: The ex-vivo model was scanned on a 3.0T clinical MRI system (Signa Premier, GE Healthcare) using a high-density flexible surface coil array (AIR Coil, GE Healthcare). 3D flow dynamics were acquired using the radially undersampled 4D Flow MRI sequence PC-VIPR7. ECG gaiting necessary for time-resolved acquisition was achieved using a transistor-transistor logic (TTL) ECG signal from the pump. Data analysis was performed in Ensight (Ansys, Inc). A detailed summary of the experimental setup and MRI acquisition parameters are shown in Figure 2.
Results
4D Flow MRI data analysis included flow rate and volume quantification as well as representative curves for inflow and outflow. Left ventricular inflow and aortic outflow curves were successfully replicated. Ultrasound images (Figure 3), confirmed valvular closure, which correlated with the lack of retrograde flow seen in the 4D Flow MRI pathlines (Figure 4).Discussion
The ex-vivo method presented here provides a robust benchtop platform for dynamic AV testing in a “semi-in-vivo” environment for evaluation of valve performance. By mounting the left heart, and secondarily the aortic valve, on a mock circulatory system, we are able to apply systemic flow conditions such as cardiac output, blood pressure and heart rate to mimic in-vivo conditions. While other systems are in development that mount the AV and LVOT on a pulse duplicator system, the set up presented here requires minimal manipulation of the aortic valve, annulus and LVOT, preserves the right heart for potential pulmonary valve evaluation and is uniquely MRI compatible.8 Ongoing work is focused on surgically correcting leakage around the inflow cannula and therefore volume loss, as reflected in our outflow wave.Conclusion
4D Flow MRI offers a non-invasive method to evaluate the aortic valve, when properly mounted on a left-ventricle driven mock circulatory system. The resulting data is valuable for hemodynamic-driven valvular analyses and eventually, for exposing the pulmonary valve to systemic flow conditions to determine Ross Procedure viability.Acknowledgements
GE Healthcare provides support to the University of Wisconsin.References
1 Torii, R. et al. Integrated morphologic and functional assessment of the aortic root after different tissue valve root replacement procedures. J Thorac Cardiovasc Surg 143, 1422-1428, doi:10.1016/j.jtcvs.2011.12.034 (2012).
2 Bissell, M. M. et al. Differential flow improvements after valve replacements in bicuspid aortic valve disease: a cardiovascular magnetic resonance assessment. J Cardiovasc Magn Reson 20, 10, doi:10.1186/s12968-018-0431-5 (2018).
3 Notzold, A. et al. Quality of life in aortic valve replacement: pulmonary autografts versus mechanical prostheses. J Am Coll Cardiol 37, 1963-1966, doi:10.1016/s0735-1097(01)01267-0 (2001).
4 Reece, T. B. et al. Rethinking the ross procedure in adults. Ann Thorac Surg 97, 175-181, doi:10.1016/j.athoracsur.2013.07.036 (2014).
5 Stulak, J. M. et al. Spectrum and outcome of reoperations after the Ross procedure. Circulation 122, 1153-1158, doi:10.1161/CIRCULATIONAHA.109.897538 (2010).
6 Charitos, E. I. et al. Reoperations on the pulmonary autograft and pulmonary homograft after the Ross procedure: An update on the German Dutch Ross Registry. J Thorac Cardiovasc Surg 144, 813-821; discussion 821-813, doi:10.1016/j.jtcvs.2012.07.005 (2012).
7 Johnson, K. M. et al. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med 60, 1329-1336, doi:10.1002/mrm.21763 (2008).
8 LaSala, V. R. et al. An Ex Vivo Porcine Model for Hydrodynamic Testing of Experimental Aortic Valve Procedures and Novel Medical Devices. J Vis Exp, doi:10.3791/65885 (2023).
Figures