0281
bSSFP Phase Contrast (PC-SSFP) at 0.55T for Aortic Flow1Department of Biomedical Engineering, Yale University, New Haven, CT, United States, 2Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States, 3Department of Radiology and Biomedical Imaging, Yale University, New Haven, CT, United States
Synopsis
Keywords: Flow, Low-Field MRI
Motivation: Aortic flow imaging at 0.55T has limited SNR, especially in diastolic phases, which can limit the accuracy of flow and regurgitant fraction measurements.
Goal(s): Our goal was to improve the SNR of phase contrast images at 0.55T using a bSSFP readout and maintain accurate flow quantification.
Approach: We developed a through-plane phase contrast sequence with bSSFP readout and tested it in phantoms and healthy volunteers.
Results: Significantly improved SNR (25.5±9.6 vs 8.2±2.9, p<0.001) and accuracy of velocities measurement were demonstrated in phantom. Accurate flow and constant high SNR were measured using our method in 8 subjects, for both breath-hold and free-breathing cases.
Impact: Our proposed phase contrast with bSSFP readout can reliably evaluate aortic flow at 0.55T with higher SNR and VNR leading to more accurate quantification compared to conventional GRE based phase contrast method.
Introduction
Lower field MRI systems may improve patient access to cardiovascular magnetic resonance (CMR). However, the challenge of reduced SNR at lower field is problematic for certain MRI sequences, e.g. phase-contrast (PC). Though vital tool for CMR (1), GRE-based PC provides low SNR even at conventional field strengths, especially in diastole when there is no inflow contrast. Balanced steady state free precession (bSSFP) has high SNR (2), and many studies have successfully combined PC with bSSFP. Recently, PC-SSFP methods were studied at 0.55T (3, 4) which provided a 2.9-fold increase in SNR vs. PC-GRE, and reasonable flow accuracy, except overestimation at high velocities (3). That study used a bSSFP pulse sequence with inversion of the slice-select gradient to generate the negative bipolar (5, 6). We previously presented an in-plane PC-SSFP method for 3T (7) with a different approach, by carefully designing M0 and M1 gradient moments at both the TR and TE to reduce velocity errors, similar to multi-echo PC-SSFP method (8) but with an optimized TR. Compared to other approaches, uncoupling the velocity encoding from slice-selection process yields more flexibility and accuracy. Here we translate this method for through-plane flow at 0.55T. We hypothesized that our method would yield similar flow but higher SNR vs. PC-GRE at 0.55T, which might permit imaging in one breath-hold without need for averaging.Methods
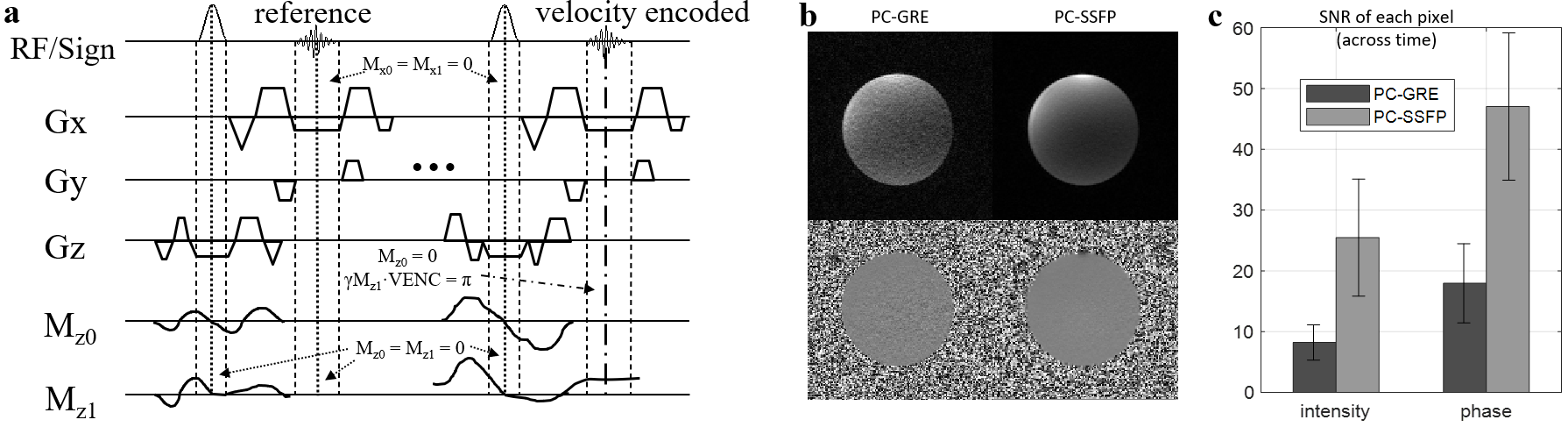
PC-SSFP was implemented for 0.55T (prototype Aera, Siemens Healthcare, Erlangen, Germany), with sequence diagram shown in Figure 1a. Gradients were carefully designed for specified VENC and to null M0 and M1 at the TE and TR. PC-SSFP used the following scan parameters: TR/TE/θ=5.6ms/2.5ms/60°, FOV=270*360 mm, slice thickness=8 mm, VENC=150cm/s, 60% asymmetric-echo, ECG-retrospectively gated, bandwidth =300Hz/pixel, temporal resolution 23ms, 3 averages, free-breathing. We compared to PC-GRE with similar parameters except TR/TE/θ=7ms/4.3ms/15° and temporal resolution 28ms. Breath-hold experiments were also conducted, with doubled temporal resolution and no averages. A 12-channel prototype cardiac and lung coil was used for signal reception (NeoCoil LLC, Pewaukee, WI, USA). Phantom studies: A static phantom was imaged at 0.55T with PC-GRE and PC-SSFP to compare SNR; the SD of the phase (with mean flow expected to be 0) was obtained over 30 acquired phases. To validate PC-SSFP’s through-plane flow quantification, a tap-water filled flow phantom was studied at 3T (mean velocities -60cm/s to +60cm/s). In vivo studies: 8 subjects were imaged at 0.55T. All subjects provided written informed consent, and the study was approved by the institution’s IRB. ROIs were drawn for velocity SD calculation, on static tissues where ideally phase should be zero. Aortic flow, net volumes, and velocity SD across the cardiac cycle were compared. Correlations between breath-hold and free-breathing were also studied.Results
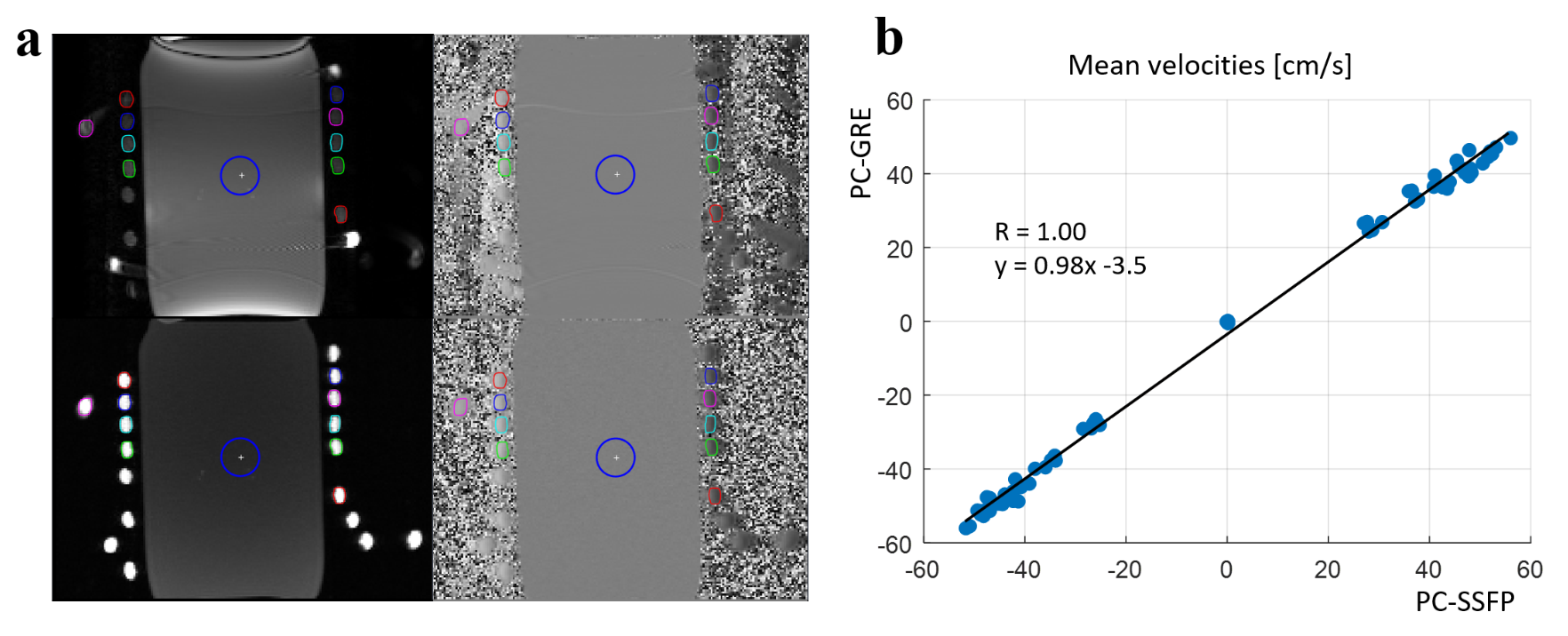
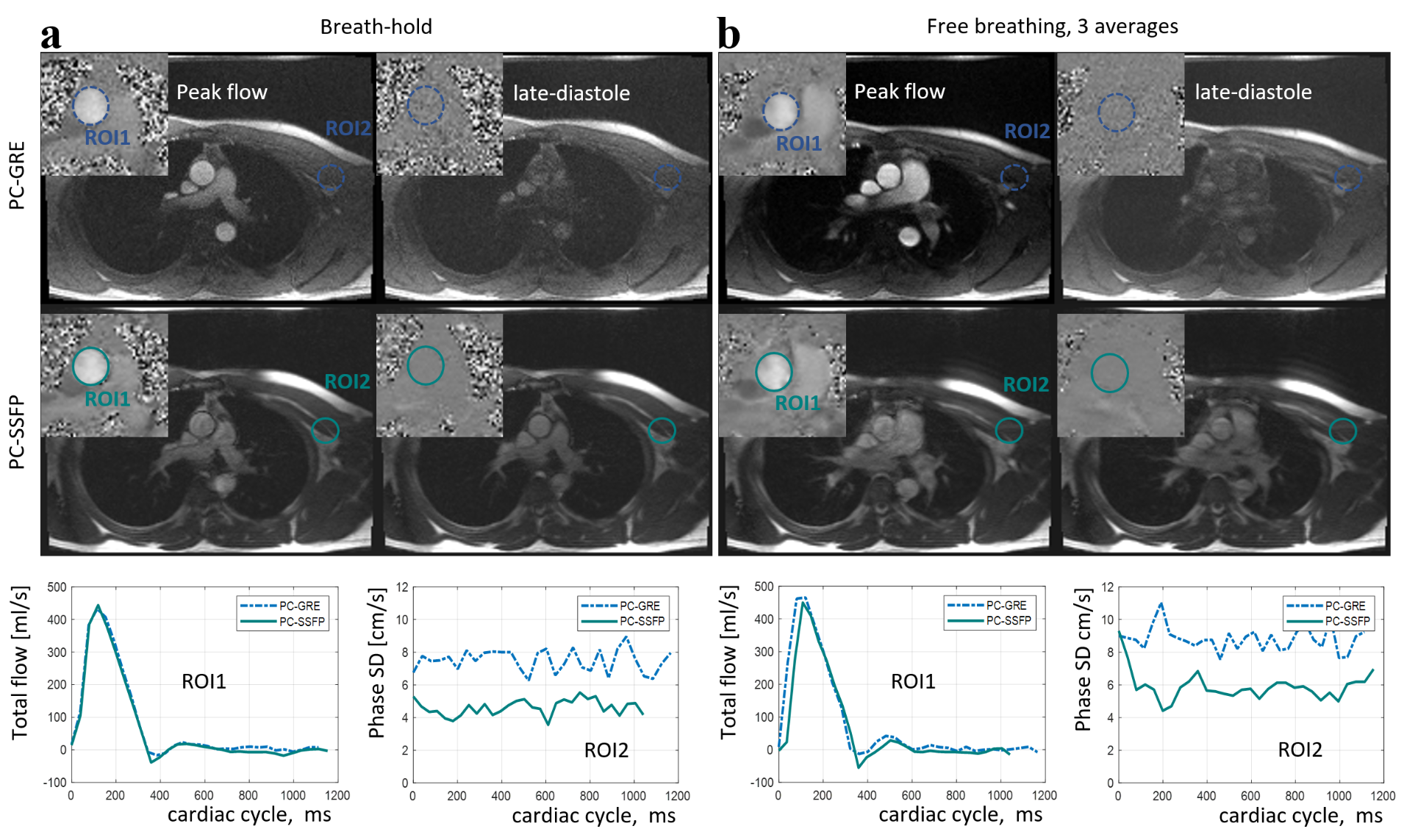
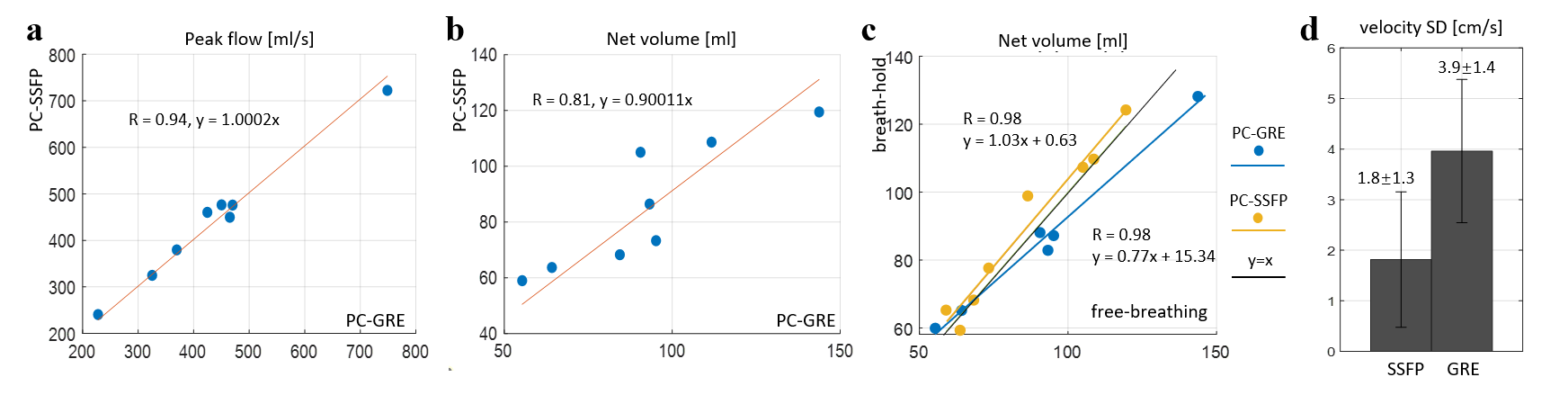
In static phantom experiment at 0.55T (Figure 1b), SNR was significantly improved using PC-SSFP vs PC-GRE (25.5±9.6 vs 8.2±2.9, p<0.001, 3-fold increase). The phase SD (mm/s) was much lower with PC-SSFP (18.0±6.5 vs 47.0±12.1, p<0.001). Figure 2 compares the measured mean velocities using PC-GRE and PC-SSFP in the flow phantom at 3T, for each ROI at different flow velocities, showing excellent agreement. Figure 3 compares PC-SSFP and PC-GRE at 0.55T in one example subject. The improved SNR with PC-SSFP vs. PC-GRE was evident, and PC-GRE exhibited low SNR even with 3-averages. For the breath-hold acquisitions, PC-SSFP still had consistently high SNR at 0.55T. Over the 8 subjects (Figure 4) imaged during free breathing, PC-SSFP measured similar peak flows but smaller net volumes (ratio=0.9, R=0.81) vs. PC-GRE. Breath-hold and free-breathing acquisitions correlated well in both PC-GRE and PC-SSFP, and PC-SSFP showed a slope close to unity, suggesting that breath-hold PC-SSSFP was not compromised by low SNR. The SD of the phase histograms (cm/s) in the static ROIs (see Figure 3, ROI2) demonstrated much improved VNR using our proposed PC-SSFP method (1.8±1.3 vs 3.9±1.4, p<0.001).Discussion
The developed PC-SSFP method was tested in phantoms and healthy volunteers at 0.55T, showing flow quantification agreement with conventional PC-GRE methods. Furthermore, our method provided greatly improved myocardium-blood contrast especially in diastole, and lower noise across the cardiac cycle, suggesting it a preferable approach at 0.55T. However, the measured net volumes differed from PC-GRE. This may be due to (1) a shorter TR thus higher temporal resolution, which better captured the negative flow at dicrotic notch (2) better SNR which might result in flow closer to zero in diastolic phases. PC-GRE with limited temporal resolution and SNR may overestimate net volumes.Conclusion
Our PC-SSFP method can improve the aortic flow image quality at 0.55T MRI, by providing much improved SNR and VNR.Acknowledgements
No acknowledgement found.References
[1] Dumoulin CL, Hart HR Jr. Magnetic resonance angiography. Radiology. 1986;161(3):717-720. doi:10.1148/radiology.161.3.3786721
[2] Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. Eur Radiol. 2003;13(11):2409-2418.
[3] McGrath C, Bieri O, Kozerke S, Bauman G. Self-gated cine phase-contrast balanced SSFP flow quantification at 0.55 T [published online ahead of print, 2023 Sep 5]. Magn Reson Med. 2023;10.1002/mrm.29837. doi:10.1002/mrm.29837
[4] Ramasawmy R, Herzka1 D, Lederman R, and Campbell-Washburn A. Spiral bSSFP Phase-contrast Flow at 0.55T. ISMRM 2020 proceding#1332
[5] Nielsen JF, Nayak KS. SSFP and GRE phase contrast imaging using a three-echo readout. Magn Reson Med. 2007;58(6):1288-1293. doi:10.1002/mrm.21276
[6] Markl M, Alley MT, Pelc NJ. Balanced phase-contrast steady-state free precession (PC-SSFP): a novel technique for velocity encoding by gradient inversion. Magn Reson Med. 2003;49(5):945-952.
[7] Xiang J, Lamy J, Qiu M, Galiana G, Peters DC, K-t PCA accelerated in-plane balanced steady-state free precession phase-contrast (PC-SSFP) for all-in-one diastolic function evaluation. Magn Reson Med. 2023. doi:10.1002/mrm.29897
[8] Nielsen JF, Nayak KS. SSFP and GRE phase contrast imaging using a three-echo readout. Magn Reson Med. 2007;58(6):1288-1293. doi:10.1002/mrm.21276
Figures